Your phone rings after midnight. A parent, spouse, or patient is in a hospital far from home. The doctor says they may need to be flown to another facility, or they can’t safely travel by ground. The first question is medical. The second is financial. Families usually ask both at the same time.
That’s where Medicare gets confusing. Yes, Medicare can cover air ambulance. No, it doesn’t cover every flight. And the hardest part is this: a flight can be medically appropriate by medical standards and still get denied or only partially paid under Medicare’s rules.
That gap matters more now because air ambulance use is rising. From 2016 to 2020, air ambulance claim lines increased 30 percent as a share of all ambulance services, and that growth was concentrated among people 65 and older in the Medicare population, according to National Library of Medicine reporting on Medicare air ambulance data. If you’re sorting this out for a parent, a fragile senior, or a discharge patient, you’re not dealing with a rare edge case.
Families often know what an air ambulance is in broad terms, but they need practical clarity fast. A plain-language explainer on what an air ambulance really does and why it matters can help if you’re trying to understand the transport side while the billing questions are still unfolding.
When a Medical Crisis Demands a Flight
A hospital transfer request can sound straightforward. It rarely is. The sending team may be focused on stabilizing the patient, while the family is trying to understand whether Medicare will treat the flight as necessary care or as a noncovered convenience.
The emotional trap is common. A family hears “air ambulance” and assumes that if a physician recommends it, Medicare will pay. Sometimes that’s true. Often, the key question is whether Medicare agrees that ground transport would endanger the patient’s health and whether the patient is going to the nearest appropriate facility.
Coverage decisions usually turn on documentation and destination, not just urgency.
Case managers run into the same pressure from a different angle. They’re trying to move a patient safely, avoid a discharge delay, and prevent a giant bill from landing on the family weeks later. That’s why the Medicare standard matters before wheels-up, not after.
The Golden Rule Medicare Medical Necessity
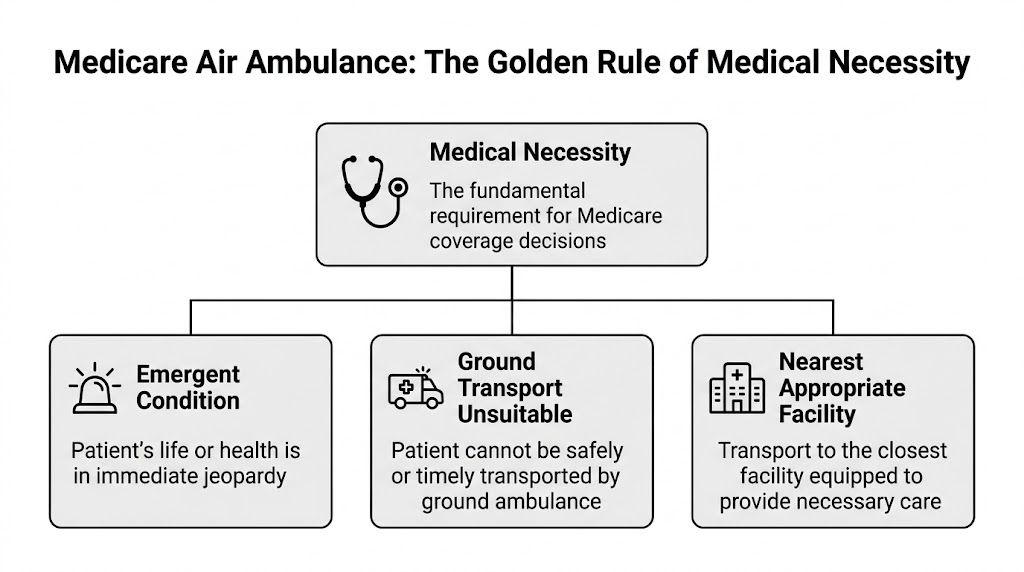
If you want the short answer to “does medicare cover air ambulance,” here it is: Medicare Part B may cover it only when the flight is medically necessary under Medicare’s standard.
What Medicare is actually looking for
Medicare’s rule is narrower than many families expect. Medicare Part B covers air ambulance services only when ground transport would endanger the patient’s health because of distance or terrain, and only when the patient is taken to the nearest appropriate facility. A physician’s certification of necessity is a major practical factor, and claims are often denied when a suitable hospital could have been reached by ground within a reasonable time, according to this Medicare air ambulance coverage explanation.
In practice, that usually means one of these situations:
- Ground access is not realistic. The patient is in a place a ground ambulance can’t safely or promptly reach.
- Time matters clinically. Ground transport would take too long for the patient’s condition.
- The receiving hospital is the nearest one that can provide the needed care. Not the preferred hospital. Not the one closer to family. The nearest appropriate one.
What gets claims into trouble
The biggest denial trigger is the destination. If a patient is flown past a capable local facility to a more distant hospital, Medicare may decide the extra distance was not covered. That’s true even when the farther hospital feels like the better choice for family reasons or continuity of care.
Another problem is thin documentation. “Patient needed air transport” isn’t enough. The record should explain why ground transport was unsafe, what level of care the patient needed during transport, and why the receiving facility was the nearest one that could provide that care.
Practical rule: If the chart doesn’t clearly answer “Why not ground?” and “Why this hospital?”, expect trouble.
Questions to ask before the flight
If the transport is not a pure scene emergency, ask these questions right away:
- What medical risk makes ground unsafe or too slow?
- Is the receiving hospital the nearest facility that can provide the required treatment?
- Has the physician documented medical necessity in writing?
- Is the transport provider enrolled with Medicare?
Those questions don’t guarantee payment. They do reduce avoidable denials.
Original Medicare vs Medicare Advantage Coverage
A family may hear, “The flight was medically necessary, so Medicare should cover it,” and assume the billing side is settled. It is not. The hard part is often the difference between Medicare’s coverage rules, the plan’s own rules, and the amount the air ambulance company bills.
How Original Medicare usually works
With Original Medicare Part B, a covered air ambulance claim is generally treated like other Part B services. After the Part B deductible, Medicare typically pays 80 percent of the approved amount, and the patient owes 20 percent coinsurance.
That sounds straightforward. The practical problem is that the approved amount and the provider’s charge are often far apart. Families hear “80 percent covered” and expect a modest bill, then learn Medicare paid its share of a much lower allowed amount. The provider’s charge does not disappear just because the transport met Medicare’s medical necessity standard.
That gap matters even more on long-distance or high-acuity transports. If you want a plain-language breakdown of the cost drivers, this guide to air ambulance pricing and the questions you’ll be asked when you call is a useful reference.
Why Medicare Advantage is more complex
Medicare Advantage plans must cover Medicare-covered services, but they can still impose plan rules that change the claim outcome and the member’s bill. Network status, authorization rules, and plan-specific cost sharing often become the deciding issues, especially for interfacility transfers and non-scene flights.
Families and case managers frequently find themselves caught. A hospital may confirm that the patient needs a flight. The plan may still question whether the air carrier was in network, whether prior authorization should have been obtained, or whether the receiving facility fit the plan’s transfer rules.
That risk is higher with specialized transfers. Ventilator flights, NICU transports, ECMO-capable teams, and bariatric transports often involve a limited pool of providers. The clinically appropriate operator may not be contracted with the patient’s Medicare Advantage plan. In practice, that can leave the member exposed to a denial, higher cost sharing, or a long appeal over out-of-network status.
If you need a refresher on plan design before sorting out a transport bill, this overview of what a Medicare Advantage Plan is is useful background.
Side by side comparison
| Feature | Original Medicare (Part B) | Medicare Advantage (Part C) |
|---|---|---|
| Basic coverage rule | Must meet Medicare medical necessity standard | Must meet Medicare standard and the plan’s own coverage rules |
| Provider network impact | Less central, though billing exposure can still exist | Often decisive, especially for interfacility and planned transfers |
| Cost sharing | Deductible and coinsurance apply to the approved amount | Varies by plan and may depend on network status |
| Prior authorization | Less common in true emergencies | Frequently important for planned or specialized transports |
| Big practical risk | Family assumes Medicare’s payment will match the provider’s bill | Member assumes medical necessity automatically overrides network and authorization rules |
A medically justified flight can still turn into a coverage dispute under Medicare Advantage.
What works before transport
For Part C members, the best protection is specific documentation and direct plan verification before any non-emergency or specialized transfer. Ask the ordering physician to document the medical reason ground is unsafe, the level of care needed during transport, and why the receiving facility is the nearest appropriate center for that service line. Then confirm the transport provider’s network status with the plan, ask whether authorization is required, and request the reference number for the call.
Verbal reassurance from someone outside the health plan is not enough. Good clinical coordination does not guarantee a paid claim. For Medicare Advantage members, the safest file is the one that shows medical necessity and proves the plan rules were addressed before the aircraft ever lifts off.
Calculating the Real Cost of an Air Ambulance Flight
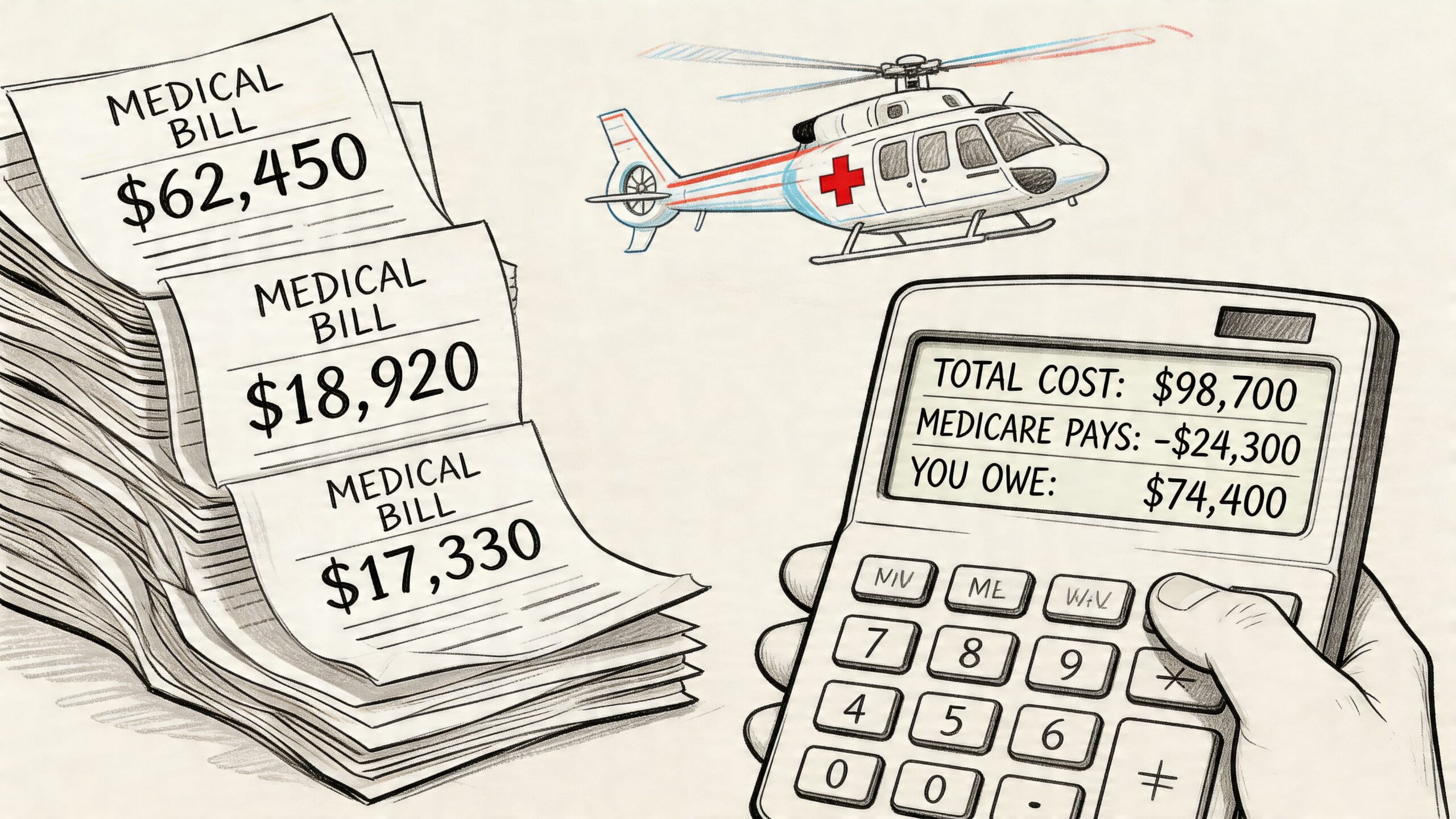
A family gets told, “Medicare should cover it,” and assumes the bill will be painful but manageable. Then the claim processes, Medicare pays its allowed amount, and the transport invoice is still far higher than expected. That gap is where significant financial risk sits.
The gap that catches families off guard
The number on the provider’s bill and the amount Medicare recognizes are often very different. For families, that distinction matters more than the general statement that air ambulance service is “covered.”
Under Original Medicare, payment is tied to the Medicare-approved amount. After the deductible, Medicare generally pays its share of that approved amount, and the patient is responsible for the remaining coinsurance. That can still leave a meaningful bill, especially if there are extra charges Medicare does not allow or the claim is only partly approved.
I tell families to ask two separate questions, not one. First, what amount does Medicare consider payable for this flight? Second, what is the provider’s full charge? If no one can answer both, the financial picture is still incomplete.
What out-of-pocket can still look like
Even on a covered claim, out-of-pocket costs can be significant. Coinsurance, deductible exposure, mileage-related charges, and onboard clinical staffing all affect the final balance.
The bigger problem is that coverage does not guarantee the provider’s full invoice will be satisfied. A medically necessary flight can still leave a patient responsible for charges above Medicare’s allowed amount, depending on how the claim is processed and whether any portion is denied.
For a practical overview of the factors that shape pricing before a quote is even discussed, this guide to air ambulance cost and what impacts the price is useful.
A quick explainer can also help if you’re trying to understand why pricing feels so opaque before you sign anything:
The term to know
Balance billing is the term families and case managers need to watch for. It means the provider is seeking payment beyond what the insurer allowed or paid.
That risk is often sharper for Medicare Advantage members. If the air carrier is out of network, if authorization was missing, or if the plan later disputes the level of medical necessity, the member can end up fighting both a coverage issue and a billing issue at the same time.
Before accepting financial responsibility forms for a non-emergency transfer, get the claim path documented. Ask for the provider’s full legal billing name, network status if a Medicare Advantage plan is involved, the expected CPT or HCPCS transport coding if available, and a written estimate of patient responsibility if the provider will give one. Those steps do not remove the risk, but they do make surprises easier to challenge later.
Navigating Planned and Specialized Medical Flights
Not every air ambulance request begins with a roadside emergency or a stroke alert. Many are planned interfacility transfers. These cases often involve a fragile senior, a patient who needs specialty care, or a discharge plan that can’t be handled safely by commercial travel.
Why planned flights are harder to approve
The challenge is that planned flights get more scrutiny. The sending team has more time to document the case, and Medicare expects that documentation to be specific.
Verified data states that 40 percent of air transports are non-emergency inter-facility transfers, and Medicare denies about 25 percent of these claims without strong physician documentation showing that ground transport poses a significant health risk, according to this summary on Medicare ambulance and air ambulance services.
That means a planned transfer needs more than a physician’s preference. It needs a clinical record that explains why the patient can’t tolerate ground movement, delay, or the level of care limitations associated with surface transport.
Documentation that actually helps
For case managers and families, these are the items that usually matter most:
- A physician certification with clinical detail. The note should describe the patient’s condition, why ground transport is unsafe, and what in-transit monitoring or treatment is required.
- A clear receiving-facility rationale. The chart should show why that hospital is the appropriate destination.
- Provider qualification checks. Confirm the transport vendor can supply the crew and equipment the patient needs.
- Billing questions before acceptance. Ask whether the provider accepts Medicare assignment and what happens if Medicare allows less than the billed charge.
If the patient may not need a full aircraft medical crew but still can’t travel commercially without help, a lower-intensity option may be worth discussing. In some cases, medical escorts fit the patient’s needs better than a full air ambulance.
The cleanest file wins. Medicare review goes better when the chart reads like a clinical necessity record, not a transportation preference.
Specialized transfers require plain documentation
Bariatric transport, oxygen dependence, ventilator support, and fragile post-hospital status all need clear language in the record. Avoid shorthand. If repositioning risk, airway issues, or monitoring needs make ground transport unsafe, those points should appear in the physician documentation before the trip whenever possible.
What to Do If Medicare Denies Your Claim
A denial letter feels final when you’re already dealing with a hospital stay or a difficult recovery. It isn’t final. Many denials turn on incomplete records, unclear medical necessity language, destination issues, or plan processing errors.
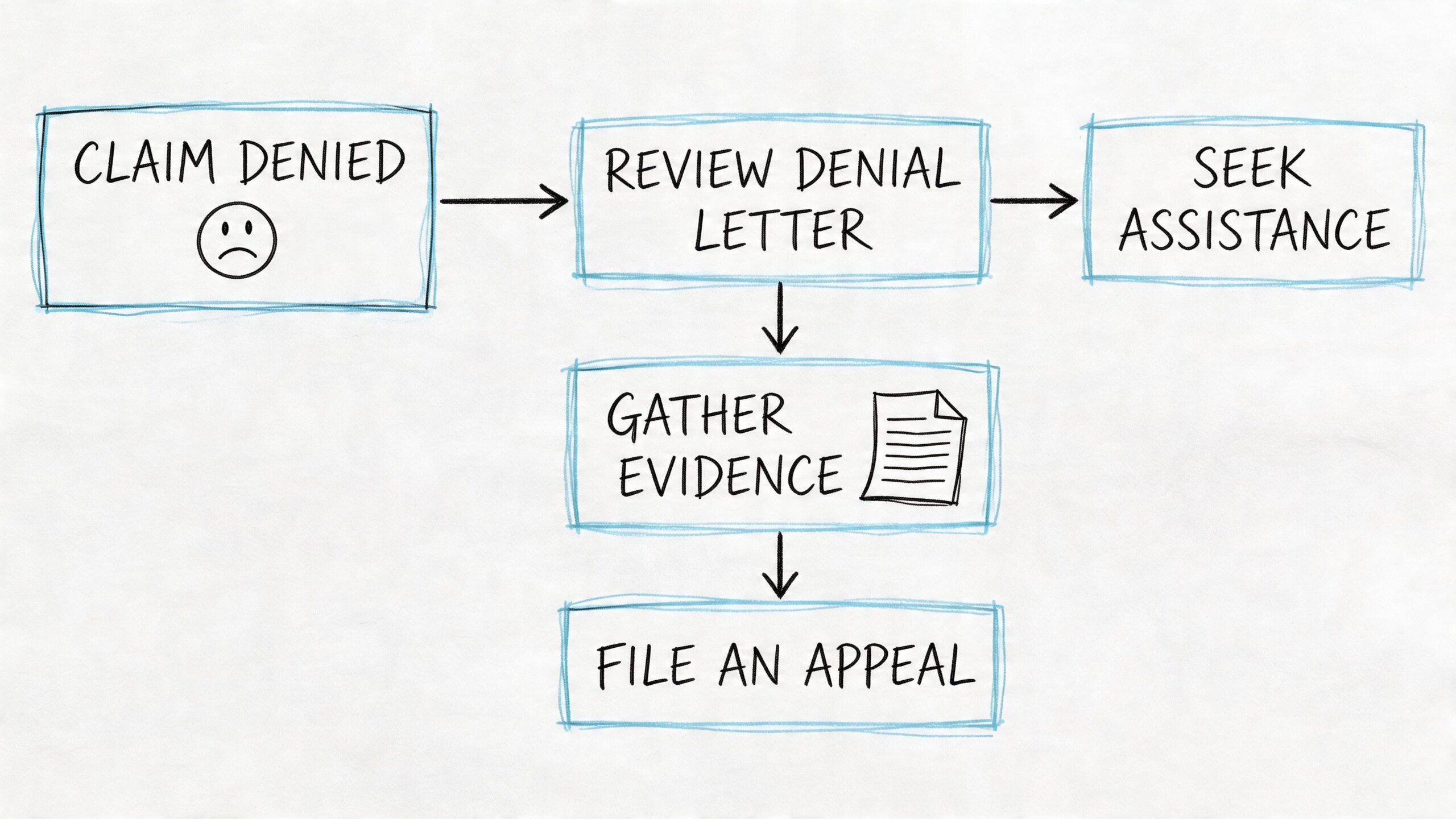
Start with the denial reason
Read the denial carefully and identify the exact issue. The usual questions are familiar:
- Medical necessity dispute. Medicare or the plan says ground transport would have been adequate.
- Destination problem. The receiving hospital wasn’t considered the nearest appropriate facility.
- Network issue. This shows up often with Medicare Advantage plans.
- Missing or weak records. The transport may have been appropriate, but the file didn’t prove it.
You can’t write a strong appeal until you know which of those problems you’re trying to fix.
Build the appeal around the chart
The appeal should be driven by records, not frustration. Gather:
- The physician certification or order
- Hospital notes describing the patient’s condition at the time of transport
- Transport records showing monitoring, interventions, or crew needs
- Receiving hospital information showing why that facility was appropriate
- Any prior authorization or plan communication, if applicable
Ask the air ambulance provider’s billing department for a complete claim packet. Good billing teams know what Medicare reviewers tend to ask for, and they may already have run into the same denial pattern before.
Keep every document in one file. When families appeal in pieces, important details get lost between letters, calls, and portal uploads.
Write the appeal clearly
A useful appeal letter is short and clinical. State what happened, why the patient could not safely go by ground, and why the destination was medically appropriate. Attach records that support each point.
Don’t rely on emotional language alone. “We were scared” is true, but it doesn’t answer Medicare’s coverage test. “Ground transport would have delayed required care and the sending physician documented that risk” is the kind of statement that belongs in the appeal.
Get help when the billing process gets messy
Families often need support beyond the provider’s own billing office, especially when a claim bounces between payer rules and medical records requests. If you’re trying to understand the denial workflow from the revenue-cycle side, this overview of medical billing denial management gives useful context on how denials are worked and corrected.
Don’t miss the practical follow-up steps
Also check whether the patient has Medigap coverage if they’re in Original Medicare. A supplemental policy may help with coinsurance on covered claims. It won’t solve every denied-flight problem, but it can matter when the dispute is about patient share rather than basic eligibility.
If the claim is under a Medicare Advantage plan, keep records of every plan call, reference number, and representative name. Those notes become valuable if the appeal turns into a dispute over network status, authorization, or plan handling.
Frequently Asked Questions
Does Medicare cover an air ambulance to a hospital closer to family
Usually not just for family convenience. Medicare’s rule focuses on the nearest appropriate facility that can provide the needed treatment. If a closer-to-family hospital is farther away than a capable local hospital, the extra distance can create patient liability.
Does Medicare cover a non-emergency flight home after hospitalization
Not automatically. A flight home may be medically understandable and still fail Medicare’s coverage standard if the patient could travel safely by ground or another lower-acuity option. For planned transports, the documentation has to show why ground would endanger the patient’s health.
Can a Medicare patient use a fixed-wing medical flight for an interfacility transfer
Sometimes, but approval still depends on medical necessity, not the aircraft type alone. The record should show why the patient needed that level of transport and why the receiving facility was medically appropriate.
What should a case manager verify before approving a planned transfer
At minimum, confirm the physician certification, receiving-facility rationale, Medicare or plan details, provider enrollment status, and expected billing method. For Medicare Advantage, confirm network status directly with the plan when time allows.
Will Medicare pay if the provider is out of network under Medicare Advantage
It depends on the plan and the circumstances. This is one of the highest-risk areas for surprise bills, which is why direct plan verification matters so much in non-emergency transfers.
Are air ambulance membership programs worth it
They can help in some situations, but families should read the fine print carefully. The key questions are which providers participate, what happens if another carrier flies the patient, and whether the program addresses coinsurance, denials, or balance billing exposure.
If you need help coordinating a flight, sorting through documentation, or understanding what information hospitals and families should gather before transport, Med Jets by Air Trek provides air ambulance transport coordination and support for emergency flights, planned transfers, and medical escort cases.