The call usually comes at the worst possible time. A parent fell and hit their head in another state. A spouse was taken to a small hospital after a crash. A case manager is telling you the patient is stable for now, but the current facility can’t provide the next level of care.
Then someone says the phrase medical golden hour.
That term can help people act quickly. It can also make families panic. Many hear it as, “If we don’t move this patient within exactly 60 minutes, it’s over.” That isn’t how real emergency medicine works.
I’ve spent enough time around trauma patients, helicopters, fixed-wing transfers, weather delays, and rushed bedside conversations to know where people get stuck. They want one simple answer to a hard question. Is this transfer urgent? Is an air ambulance worth it? If the flight takes longer than an hour, have we already missed the window?
The honest answer is more useful than the dramatic one. Speed matters. Continuous care matters. Getting to the right hospital matters most. And those three things are not always the same decision.
When Every Second Counts in a Medical Emergency
When your loved one is lying in an emergency department bed, the clock feels loud. You hear phrases like “higher level of care,” “neurosurgery,” “bleeding risk,” or “we need transfer acceptance,” and suddenly every minute feels like a verdict.

Families often ask the same questions.
- Is this a true emergency transfer? Sometimes yes. Sometimes the patient is temporarily stabilized but still needs services the current hospital can’t provide.
- Does “golden hour” mean we have exactly 60 minutes? No. It’s a useful trauma principle, not a universal countdown timer.
- Should we pick the closest hospital or the best hospital? In many serious cases, the best hospital is the safer choice if it can deliver definitive treatment the first hospital cannot.
Why this phrase causes so much confusion
The medical golden hour is meant to push teams toward fast intervention. That part is valuable. The confusion starts when people treat it like a hard expiration time.
A worried family member may hear “golden hour” and picture a switch flipping at minute 61. Real patients don’t work that way. Different injuries have different danger points, and what the transport team does during the trip matters too.
Practical rule: Don’t ask only, “How fast can we move?” Ask, “What care can this patient get here, during transport, and at the receiving hospital?”
What families and case managers need most
In urgent transfers, clear thinking beats dramatic slogans. The useful questions are usually these:
| Question | Why it matters |
|---|---|
| What can the current hospital not do? | This identifies whether the patient needs transfer at all. |
| What treatment does the receiving center offer immediately? | It focuses on definitive care, not just travel time. |
| Can the transport team manage the patient en route? | Continuous monitoring and intervention can protect a fragile patient during delays. |
If you remember one thing, remember this. The medical golden hour is best understood as a push toward rapid, appropriate care, not a reason to give up when logistics are messy.
Understanding the Medical Golden Hour's Origin
The phrase medical golden hour did not begin as a stopwatch rule for families to memorize. It began as a clinical warning. Dr. R. Adams Cowley introduced the concept in 1957 at the University of Maryland Medical Center after observing that badly injured patients often survived or declined based on what happened early, especially before definitive treatment was delayed. That history, along with later military research often tied to the idea, is summarized in Texas A&M's overview of the golden hour concept and battlefield findings.
A useful way to understand it is to picture a failing engine in flight. The first minutes matter because the crew must correct the problem before it cascades into a crash. Trauma care works in a similar way. Bleeding, airway problems, and shock can worsen quickly. Early action gives the patient a better chance of reaching the operating room, intensive care unit, or specialty center in a condition that can still be turned around.
How the idea shaped emergency systems
Cowley’s concept influenced how trauma systems were built. Hospitals, EMS agencies, and military planners used it to organize care around rapid recognition, fast transport, and early treatment instead of passive observation.
That shift mattered.
It helped drive the development of trauma centers, helicopter transport programs, and field protocols focused on getting the right patient to the right level of care without unnecessary delay. The central lesson was straightforward. Early care changes trajectories.
How the military reinforced the concept
The idea gained wider public attention during the wars in Iraq and Afghanistan. On June 15, 2009, U.S. Secretary of Defense Robert M. Gates directed the military to aim for transport of service members with life-threatening injuries to a medical facility within 60 minutes.
That policy changed operations, not just language. Aircraft placement, evacuation planning, and destination decisions were organized around shortening the time from injury to treatment. In other words, the golden hour became a planning target teams could act on.
What families should take from that history
The origin story matters because it explains both the strength and the limitation of the term.
The strength is clear. Serious injuries usually do better when skilled care starts early and continues without interruption.
The limitation is just as important. The original concept was never meant to suggest that recovery is possible at 59 minutes and hopeless at 61. It was a push toward urgency, coordination, and early intervention. For families and case managers arranging emergency air medical transport, that is the practical takeaway. Use the phrase as a prompt to ask, “How quickly can the patient get appropriate care, and what treatment is happening during the trip?” not “Can we beat an exact clock?”
Why the 60-Minute Rule Is a Guideline Not a Deadline
Relief and, at times, guilt are common emotions for many people. Relief because there isn’t a magical cliff at minute 61. Guilt because they’ve been told, directly or indirectly, that any delay means someone failed.
The evidence doesn’t support that kind of rigid thinking.
An extensive literature review in Academic Emergency Medicine and a prospective cohort study of 3,656 trauma victims found no definitive, peer-reviewed evidence supporting a strict 60-minute golden hour threshold as a predictor of mortality across all trauma cases, according to Journalist’s Resource’s review of the research.
What that means in plain language
If a flight takes longer than an hour because of distance, weather, aircraft availability, runway limits, or the patient’s size and medical needs, that fact alone does not tell you the outcome.
What matters more is a cluster of questions:
- Was the patient recognized as high risk early?
- Did the team begin stabilizing treatment quickly?
- Is the patient being taken to a hospital that can fix the problem?
- Can the transport crew maintain airway, circulation, sedation, and monitoring during the trip?
That’s why many clinicians prefer the term resuscitative hour. It shifts the focus from a stopwatch to the work that happens during that early period.
Why families misread the phrase
The phrase sounds precise, so people assume medicine proved the exact number. It didn’t. The original concept was useful because it made teams act with urgency. Over time, the slogan became more famous than the nuance.
Here’s the practical difference:
| Rigid myth | Clinical reality |
|---|---|
| Survival drops precisely after 60 minutes | Risk depends on injury type, physiology, and definitive care |
| Faster transport always wins | Sometimes a longer trip to the right center is safer |
| Any delay means failure | Some delays are unavoidable, and good care during them still matters |
What to tell a family member: “An hour is a serious target, not a death sentence if the trip runs longer.”
The better way to think about urgency
A patient can be moved quickly and still be moved badly. That happens when the destination can’t provide surgery, neurosurgery, or advanced critical care. It also happens when transfer begins before the patient is adequately stabilized for the trip.
A patient can also be moved a bit more slowly, but more safely and more effectively, if the team chooses the right receiving center and brings the right in-transit care.
For case managers, this changes the conversation. Instead of asking only for the fastest option, ask for the option that best balances:
- Current stability
- Transport risks
- Receiving hospital capability
- Continuity of care during transfer
The message for longer flights
If your transfer takes longer than you hoped, don’t assume the chance is gone. Ask what care is being delivered now, what the crew can continue in the air, and what the receiving team will be ready to do on arrival.
That’s a much better use of attention than staring at the clock and imagining a rule that trauma literature itself does not support as a universal law.
How Different Injuries Change the Timeline
Not all emergencies run on the same clock. That’s one of the hardest parts for families to understand, because from the waiting room every serious case looks equally urgent.
In the body, though, the problem changes the timeline. A patient bleeding internally, a patient with severe head trauma, and a patient with a painful but isolated fracture may all need transfer, but not for the same reason and not at the same pace.
The trimodal pattern in simple terms
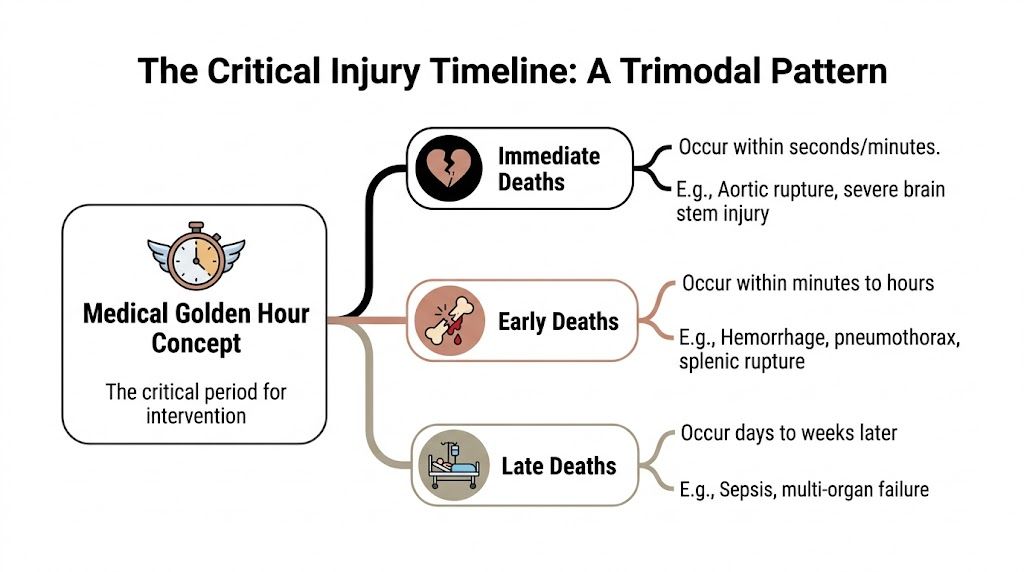
Trauma care often describes death after injury in three broad phases.
- Immediate deaths happen within seconds or minutes. These include unsurvivable injuries.
- Early deaths happen within minutes to hours. Severe bleeding and airway or chest problems often fall here.
- Late deaths happen days to weeks later. Infection and multi-organ failure are common examples.
That pattern matters because it explains why the medical golden hour isn’t one-size-fits-all. Some patients need intervention almost immediately. Others need careful stabilization and then transfer to a center that can prevent later complications.
Why head injuries need the right destination
For traumatic brain injury, the first hour is critical not because transport speed alone decides everything, but because teams need to start interventions such as intracranial pressure monitoring, cerebrospinal fluid drainage, and sedation-based management at specialized centers. Those early steps directly influence long-term outcomes, as discussed in the Journal of Neurointensive Care review on TBI timing and management.
That’s why a family may hear, “We’re bypassing a closer hospital.” It can sound alarming. Clinically, it may be the safest choice.
A smaller hospital might stabilize the airway and blood pressure. But if it can’t provide neurosurgery or advanced neurocritical care, the patient still hasn’t reached definitive treatment.
In severe head injury, the best question often isn’t “Which hospital is nearest?” It’s “Which hospital can treat rising pressure inside the skull the moment we arrive?”
A practical comparison by injury type
| Injury pattern | What matters most |
|---|---|
| Suspected severe bleeding | Rapid hemorrhage control and access to surgery |
| Suspected traumatic brain injury | Immediate access to specialized neuro care |
| Isolated fracture without major instability | Pain control, immobilization, and appropriate transfer planning |
What families should listen for
When clinicians describe urgency, listen for the reason behind it.
- “They need blood or surgery.” This usually points to a bleeding problem.
- “They need neuro monitoring.” This usually points to brain injury and a specialty center.
- “They’re stable but need a higher level of care.” This often means the patient is not crashing right now, but the current hospital can’t provide what’s needed next.
That difference can guide better decisions than the phrase golden hour by itself.
Why a longer trip can be the safer move
This is especially true for medically complex and bariatric patients. The right center may be farther away because it has the right operating room setup, critical care capacity, or specialty team.
So yes, speed still matters. But destination fit can matter more than shaving off a few travel minutes if the closer hospital can’t deliver the intervention that changes the outcome.
Making the Right Call on Interfacility Transfers
Interfacility transfer decisions usually happen after the first emergency work is done. The patient has reached a hospital. The team has identified the injury or illness. Then the limits of that facility become clear.
A common example is a rural or community hospital that can stabilize a patient but can’t provide neurosurgery, trauma surgery, advanced ICU support, or specialty services for medically fragile patients. In those moments, the transfer question isn’t abstract. It becomes, “Do we keep this patient here longer, or move them to where definitive care exists?”
When ground transport stops being realistic
In some rural settings, the usual timeline behind the medical golden hour breaks down. In areas like Montana, harsh weather and distance can push average trauma transport times to over 7 hours, as described in this discussion of rural trauma transfer delays.
That kind of reality changes the decision. You’re no longer choosing between a short drive and a short flight. You may be choosing between a prolonged ground delay and a clinically managed air transfer.
A simple framework for transfer decisions
If you’re a family member or case manager, these questions help cut through noise.
What can the current hospital do right now
Ask whether the present team can only stabilize, or whether they can also provide the next intervention the patient needs. Stabilization is important. It just isn’t always enough.
What does the receiving hospital offer on arrival
The value of transfer depends on what happens next. A Level 1 trauma center, specialty ICU, or advanced surgical program changes the equation.
What happens during the trip
A transfer is not just transportation. If you need a plain-language overview, this guide on what medical evacuation entails is useful because it explains the operational side families often don’t hear clearly at the bedside.
Decision checkpoint: Transfer makes the most sense when the current facility has reached its ceiling and the receiving facility can act immediately on arrival.
Questions worth asking before you consent
- Who accepted the patient at the receiving hospital? You want a confirmed destination, not a vague plan.
- What treatment is expected there that can’t happen here? This clarifies the purpose of the move.
- What are the transport risks for this patient specifically? Head injury, ventilator support, obesity, or unstable blood pressure all change planning.
- How will coverage and authorization be handled? Families often need practical guidance here, and a primer on whether Medicare covers air ambulance services can help frame the right financial questions early.
What case managers already know, and families often don't
The first hospital is not always the finish line. Sometimes it’s the holding point until the patient can be safely moved to where the right team and equipment exist.
That’s why “stable enough for transfer” can sound reassuring and frightening at the same time. It usually means the team has bought time, not solved the whole problem.
How Air Ambulances Bridge the Critical Time Gap
A patient is on a ventilator in a community hospital. The local team has done the hard first work. They have stabilized breathing, started medications, and called a larger center that can provide the next level of care. Now the clock matters, but not because some invisible buzzer goes off at minute 60. It matters because the patient still needs treatment during every mile between hospitals.
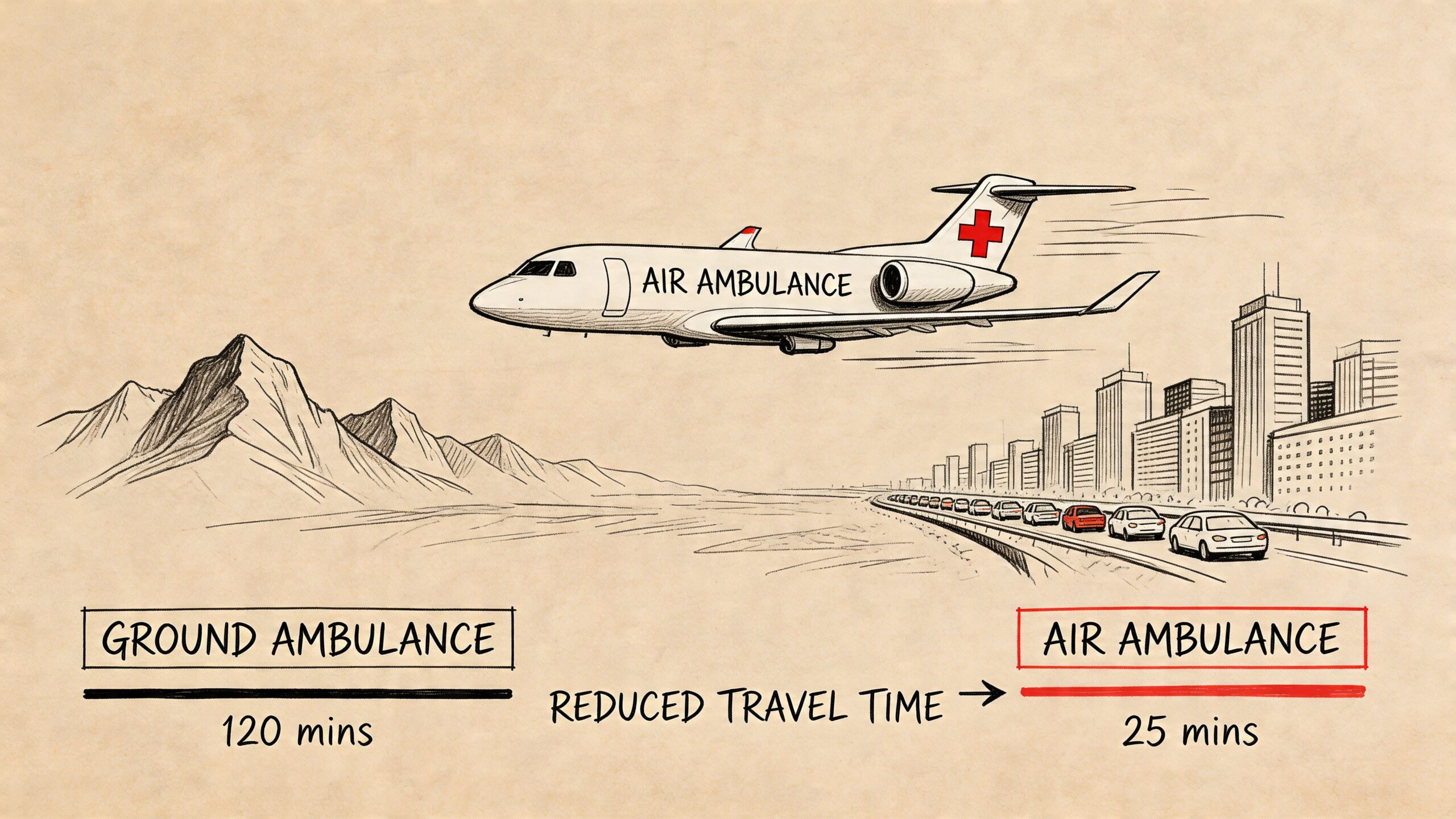
That is the gap air ambulances are built to close. They reduce travel time when geography, traffic, or distance would slow a ground transfer. Just as important, they carry ICU-level attention into the space between one bedside and the next.
The problems an air ambulance solves
Families often hear “flight” and picture speed alone. Speed matters, but the aircraft is only part of the answer. The primary value is getting the patient to the right hospital while keeping care active the whole way.
- Distance and access. Rural roads, mountain terrain, island locations, and congested urban routes can turn a transfer into a long delay. Air transport can shorten that gap.
- Continuous treatment. The patient is still being watched, assessed, and treated in transit. Oxygen, monitoring, medication infusions, airway support, and ventilator management do not pause for the trip.
- Better destination choices. A flight can make a stroke center, trauma center, burn unit, or pediatric specialty hospital realistically reachable.
- Higher-acuity transport. Some patients are too fragile for a basic ride. They need a crew and equipment set up for sudden changes in blood pressure, breathing, heart rhythm, or neurologic status.
The easiest way to picture it is this: a strong transport team works like a moving treatment room, not a taxi with sirens. If you want a clearer patient-focused explanation, this guide on what an air ambulance really does and why it matters more than people think explains that role well.
Why in-transit care changes the equation
A transfer can be one of the riskiest parts of a serious illness or injury. The patient leaves a controlled room, passes through elevators, loading areas, weather, vibration, altitude changes, and handoffs between teams. Every one of those steps can stress someone whose condition is already unstable.
Take a severe head injury. The crew may need to protect the airway, manage sedation, support blood pressure, and watch for neurologic decline during the trip. A patient with sepsis or heart failure may need oxygen changes, medication adjustments, and close cardiac monitoring. In other words, the goal is not only to arrive faster. The goal is to arrive without losing ground.
A short visual can help make that process easier to picture.
When air is the better tool
Air transport is the better choice when three things line up. The patient needs care the current hospital cannot provide, the receiving hospital is ready to act, and the trip itself needs to be shorter or medically more capable than ground transport can reasonably provide.
For families and case managers, that framework helps cut through the “golden hour” myth. The question is not, “Can we keep this under exactly 60 minutes?” The better question is, “What gets this patient to definitive care soonest while keeping treatment continuous and safe?”
Planning matters here too. Dispatch teams must coordinate aircraft availability, weather, landing logistics, hospital communication, and ground transport on both ends. Tools with optimized mapping capabilities can support that kind of route and resource planning.
A well-run transfer protects time by protecting the patient. That is what bridges the gap.
Your Urgent Medical Flight Questions Answered
People ask very direct questions when a transfer is being arranged. That’s appropriate. You don’t need jargon at that point. You need clear answers.
What information will the transport team ask for
Usually they’ll need the sending hospital details, receiving hospital acceptance, diagnosis or suspected diagnosis, current condition, equipment needs, and whether the patient is on oxygen, a ventilator, or critical medications.
They’ll also ask practical questions about weight, mobility, infection precautions, and whether a family escort is being considered. Those details affect aircraft setup and crew planning.
If the trip takes longer than an hour, is that a bad sign
Not by itself. The key issue is whether the patient is receiving appropriate monitoring and care during transfer and whether the destination can provide definitive treatment on arrival.
That’s the point many families need to hear twice. A longer transport is not automatically a failed transport.
How do hospitals and transport teams coordinate all this so fast
They use dispatch workflows, routing, weather review, aircraft availability, hospital communication, and ground coordination on both ends. Tools that improve situational awareness, such as optimized mapping capabilities, help emergency planners and coordinators visualize routes and operational constraints more clearly.
What about cost questions
Ask early. Coverage depends on medical necessity, policy details, destination, and the level of care required. Families often feel more in control when they understand the variables ahead of time, and this guide on air ambulance cost and what you’ll be asked when you call lays out the main factors in plain language.
Can family members or pets come along
That depends on the operator, aircraft configuration, patient condition, and safety requirements. It’s reasonable to ask. In some programs, family accompaniment is possible, and some services can also discuss pet-friendly arrangements when appropriate.
What should I say if I feel rushed and overwhelmed
Say this: “Please tell me what the current hospital can’t do, what the receiving hospital will do on arrival, and what support the patient will have during transport.”
That question gets you to the heart of the decision fast.
When people hear medical golden hour, they often hear fear. The better interpretation is urgency with judgment. Move quickly. Stabilize early. Choose the destination that can adequately treat the problem. Keep skilled care around the patient the whole way.
If you need help arranging an urgent flight, Med Jets by Air Trek provides 24/7 hospital-to-hospital air ambulance coordination, medical escorts, and specialized transfer support for families, case managers, and insurers.