When a hospital tells you a loved one needs an air ambulance, the first question usually isn’t about aircraft categories. It’s much more immediate. Can they travel safely? How fast can this happen? Will someone be with them? What happens if the weather changes? How many handoffs are involved between the sending room and the receiving hospital?
That’s where the fixed wing vs rotary wing decision gets misunderstood.
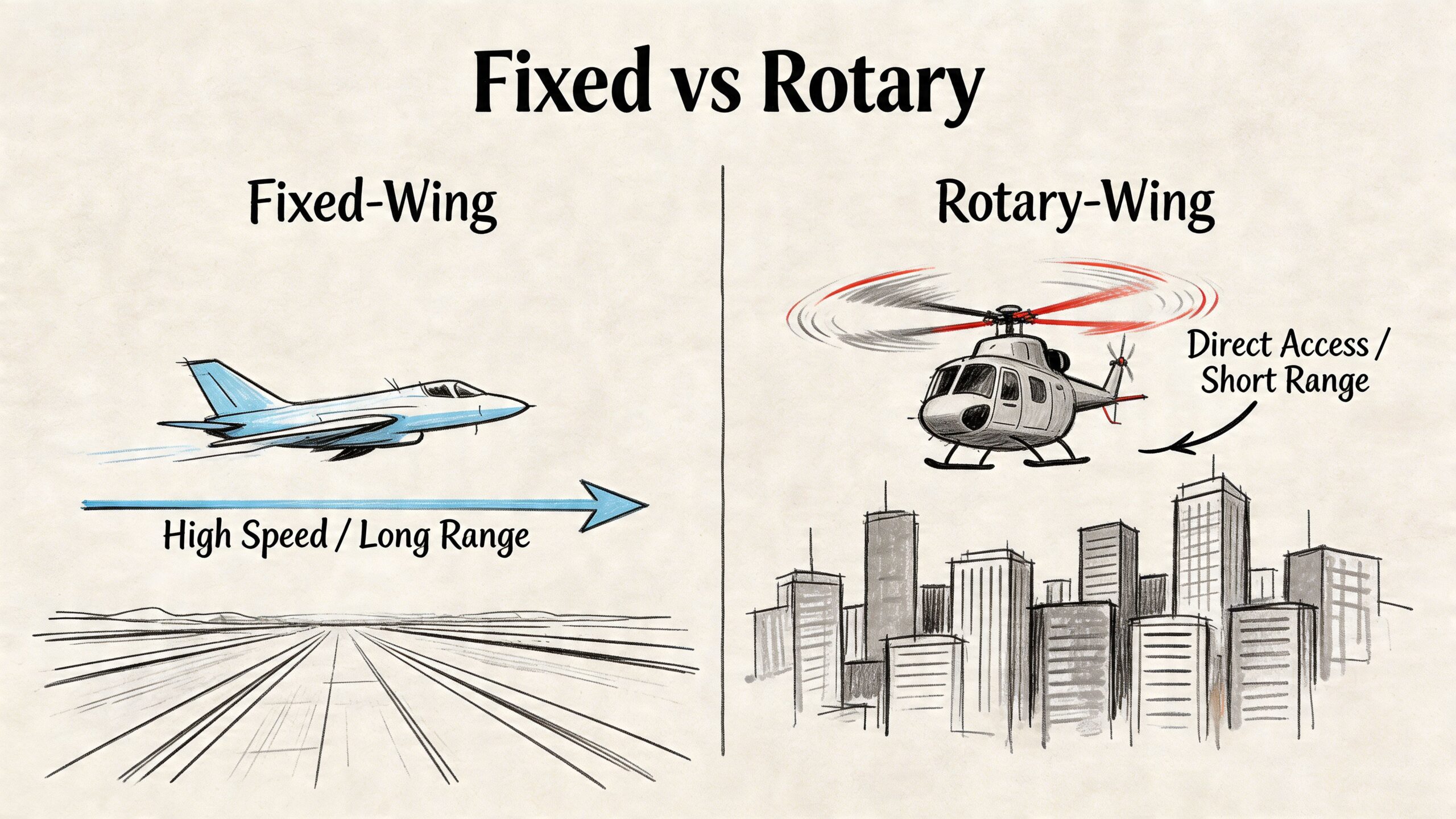
Families often hear “jet” and “helicopter” as if they’re interchangeable versions of the same service. They aren’t. They solve different transport problems. A helicopter is built for direct access into places an airplane can’t reach. A fixed-wing aircraft, meaning a medical airplane or jet, is built for longer transport where speed, endurance, cabin conditions, and total mission coordination matter more than rooftop access.
The right choice usually becomes clear once you stop thinking only about the aircraft and start thinking about the complete patient journey. In practice, bedside-to-bedside transport includes the sending unit, ground ambulance timing, airport or helipad access, loading and unloading, weather routing, clinical monitoring in flight, family accommodation, and the receiving team’s readiness on arrival.
Making the Right Choice in a Critical Moment
If you’re arranging transport right now, you’re probably juggling several conversations at once. A physician wants a transfer. A case manager needs medical records. Family members are asking if they can go. Someone is trying to compare a helicopter quote with a jet option, and all of it feels urgent.
That pressure is real. It also leads people to ask the wrong first question.
Instead of asking, “Which aircraft is better?” ask, “Which aircraft fits this patient’s full route, medical condition, and destination access?” That’s the question flight coordinators and clinical teams use every day.
Simple definitions that matter to families
A fixed-wing aircraft is an airplane or jet. In medical transport, that usually means a dedicated medical jet configured with a stretcher, medical equipment, and space for clinicians. It needs an airport or airstrip, so ground ambulances usually complete the first and last segments.
A rotary-wing aircraft is a helicopter. It can land much closer to the patient in some situations, including helipads and certain tight-access areas. That’s why helicopters are commonly associated with scene calls and short regional transfers.
The practical difference
For many hospital-to-hospital transfers, the aircraft itself is only one part of the decision. The main issue is whether the entire mission will be smooth for the patient.
What families usually need to know: the fastest-looking option on paper isn’t always the fastest bedside-to-bedside option, and the most direct-looking option isn’t always the safest or most comfortable.
Here’s the frame I use with families and discharge planners:
| Decision factor | Fixed wing | Rotary wing |
|---|---|---|
| Best fit | Long-distance hospital transfers | Short-distance direct-access missions |
| Landing needs | Airport or airstrip | Helipad or confined-access capable |
| Cabin environment | More room and a more controlled setup | Tighter clinical workspace |
| Weather flexibility | Better for routing around or above weather on longer legs | More limited by weather and altitude |
| Family logistics | Often better for accompanying travelers on planned transfers | Usually more limited |
| Total mission planning | Strong for coordinated bedside-to-bedside moves across regions | Strong for fast local pickup where direct landing matters |
Operational Speed Range and Access Explained
The biggest operational difference in fixed wing vs rotary wing comes down to how far the patient needs to go and what kind of access exists at both ends.
A fixed-wing medical aircraft is usually the stronger tool when the transfer is regional, cross-country, or international. According to the Rotor-Wing vs Fixed-Wing comparison from NB Trauma, fixed-wing jets can reach 531 km/hr, have a range of over 3,300 km, and fly at 35,000 ft in a pressurized cabin. In contrast, helicopters are limited to around 287 km/hr, about 761 km of range, and an unpressurized ceiling of 13,800 ft.
Those numbers matter because they change the entire mission profile.
What speed and range mean in real transport
If the patient is moving from one hospital to another several states away, a fixed-wing aircraft can often complete that trip with fewer interruptions. That means fewer fuel-related stops, fewer handoffs, and less time spent in transit.
For a family, this translates into a simpler question. Do you want the patient making a short local hop, or do you need a transport platform built to keep moving efficiently over long distance?
For certain time-sensitive conditions, transport teams also think in terms of the medical golden hour. That doesn’t mean every case automatically belongs on a helicopter. It means the transport mode has to match the distance, destination, and clinical urgency.
Access is where helicopters shine
Helicopters do something jets cannot. They can get closer to the point of need when there’s no practical runway access at the pickup location. If a patient is at a scene location, a rural helipad, or a hospital with direct rotor access and the destination is nearby, rotary-wing can be the right answer.
That advantage is real. But it’s only part of the story.
A fixed-wing mission usually involves coordinated ground ambulances on both ends. Families sometimes see that as a drawback until they understand how tightly those legs can be scheduled. A well-run bedside-to-bedside transfer doesn’t feel like disconnected pieces. It feels like one continuous mission with planned handoffs.
A jet may start and end at airports, but the patient experience should still feel like one coordinated transport, not three separate trips.
Here’s a quick operational comparison:
| Operational issue | Fixed wing impact | Rotary wing impact |
|---|---|---|
| Long-distance transfer | Strong advantage | Often impractical |
| Refueling on longer trips | Less likely to interrupt mission flow | More likely on extended routing |
| Weather routing | Better ability to work above or around weather | More operational limits |
| Pickup from confined area | Requires ground ambulance link | Strong advantage |
| Coast-to-coast planning | Well suited | Usually not preferred |
A short visual overview helps clarify the mission differences:
Inside the Aircraft Clinical Capabilities and Stability
Once the route makes sense, the next question is clinical. Can the aircraft support the patient well enough from departure to arrival without creating additional risk?
That’s where fixed wing vs rotary wing becomes more than an aviation discussion. It becomes a patient-care discussion.
Cabin conditions affect fragile patients
A fixed-wing medical aircraft provides a more controlled in-flight environment for longer transfers. The cabin is usually better suited for sustained monitoring, clinician movement, and equipment setup. For patients with respiratory compromise, cardiac issues, neurological concerns, or multiple infusions, that matters.
The clinical difference isn’t just comfort. It’s how manageable the patient remains in transit.
According to the fixed-wing endurance and transport comparison at Anvil, fixed-wing aircraft provide a more stable environment, can handle winds up to 40 knots better, and show lower vibration levels. The same source notes that on missions over 300 miles, fixed-wing jets can reduce total mission time by 40-60%, helping minimize hypoxia risks while supporting a cabin environment with space for advanced monitoring and care continuity.
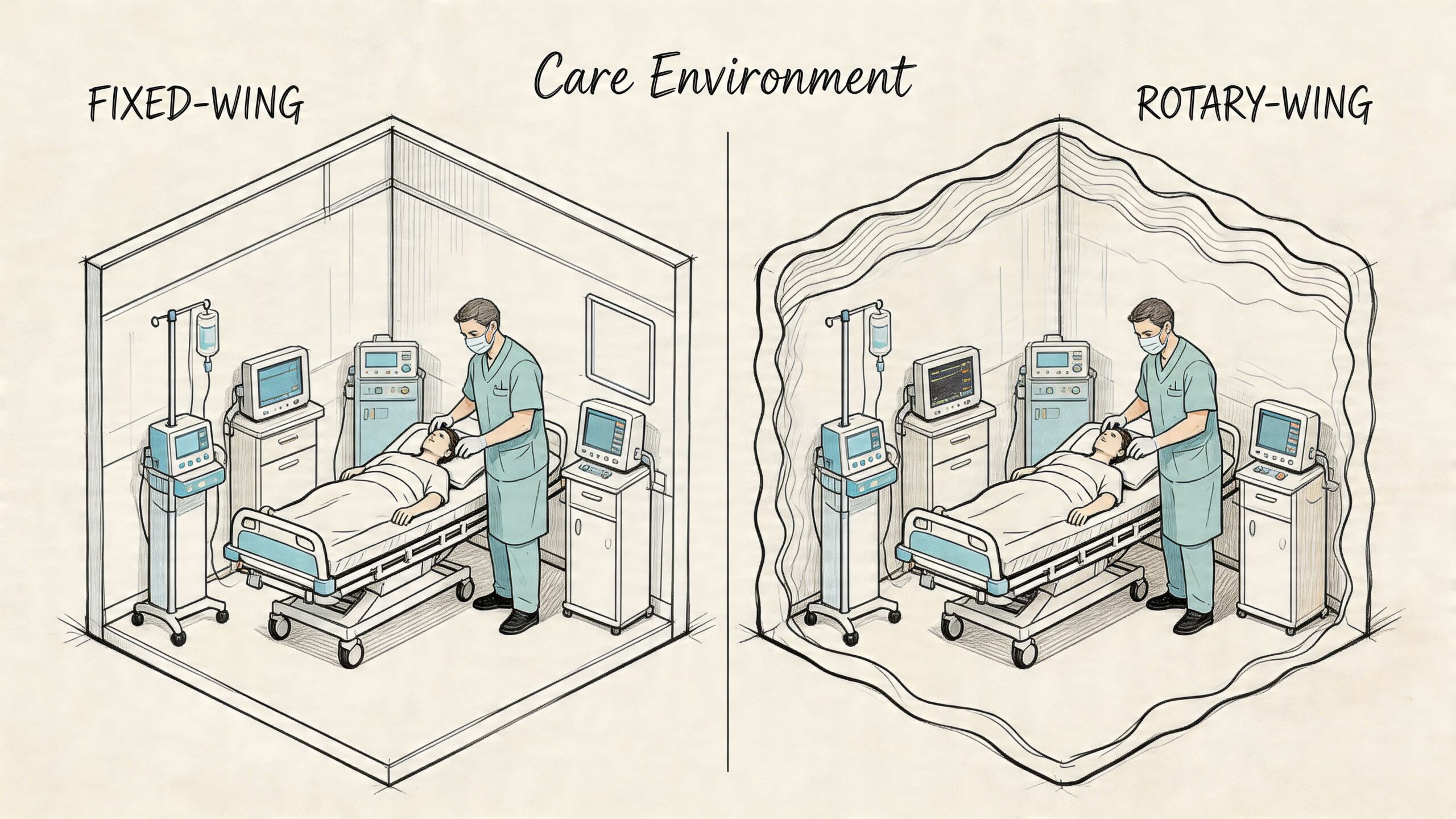
Space changes what crews can do
This is one of the most overlooked parts of the decision.
In a helicopter, crews often work in a tighter space with more noise and more vibration. That doesn’t make rotary-wing unsafe. It does mean some patients are harder to manage comfortably there, especially over a longer segment. Access to the patient can be more constrained, and small practical issues become major ones when the patient is unstable.
In a fixed-wing medical cabin, there’s usually more room to organize equipment and work deliberately. If you want a sense of the kind of onboard setup transport teams consider, this overview of air ambulance flight equipment shows why layout and access matter as much as the aircraft itself.
What works and what doesn’t
For planned ICU-level or specialty hospital transfers, fixed wing is often the better clinical environment. It gives the crew a steadier platform and a cabin that supports continuity of care across a longer route.
For short-distance pickup where direct access matters most, rotary-wing often works well, especially when the helicopter shortens the time from patient location to receiving facility.
Clinical rule: choose the aircraft that gives the medical crew the best working environment for the patient’s condition, not the aircraft that seems most dramatic or fastest from the ground.
A few patient situations that often favor a fixed-wing medical cabin:
- Respiratory fragility: Pressurized, more controlled cabin conditions can matter for patients who don’t tolerate physiologic stress well.
- Complex monitoring: Patients on multiple drips, advanced cardiac monitoring, or continuous respiratory support benefit from a workspace that gives clinicians room to move.
- Long transport time: If the route itself is substantial, stability and endurance become part of clinical safety.
- Bariatric transport: Larger cabin and payload flexibility can make the difference between a workable plan and a difficult one.
The Patient and Family Experience During Transport
Families rarely ask only about airspeed. They ask whether the patient will be comfortable, whether someone can go along, and whether the transport will preserve dignity during an already difficult day.
Those are the right questions.
What the patient actually feels
A helicopter is a highly useful medical platform, but it is typically more utilitarian in feel. The cabin is tighter. The environment is louder. Movement and vibration are more noticeable. For short emergency retrieval, that trade-off often makes sense.
A fixed-wing medical aircraft usually feels more like a controlled clinical room in motion. For a patient who is elderly, anxious, in pain, or medically fragile, that difference can shape the whole experience.
“The best transport is the one that protects the patient medically and reduces the family’s stress logistically.”
That becomes even more important in bariatric transport. Larger patients often need specialized loading plans, more room around the stretcher, and equipment placement that doesn’t compromise clinical access. In practice, fixed-wing options are often the more workable solution for those cases because the mission can be planned around the patient rather than forcing the patient into the aircraft’s limits.
Family seating and companion travel
One of the most common questions is simple. Can a family member go with the patient?
On planned fixed-wing medical transfers, that’s often more feasible than people expect. Some operators can also accommodate more than one companion depending on the mission, patient needs, and aircraft configuration. Helicopter missions are often more constrained because cabin layout and operational priorities leave less flexibility.
Families also ask about personal items, essential medications, and even whether a small pet can accompany the trip. Those policies vary by provider, but this is exactly why bedside-to-bedside planning matters. These details shouldn’t be last-minute surprises.
The handoffs shape the experience
The human side of transport often comes down to handoffs.
A rough mission feels fragmented. One ambulance is late. The airport transfer is unclear. A family member doesn’t know where to stand or what documents to carry. The receiving facility hasn’t been updated properly. Even if the flight itself is smooth, the day feels chaotic.
A strong mission feels guided. The sending team knows the pickup plan. Ground crews are sequenced. Family knows what to bring. The aircraft crew receives a clean clinical report. The receiving hospital is ready.
That’s why the fixed wing vs rotary wing choice can’t be made on aircraft specs alone. The patient remembers the whole chain, not just the airborne segment.
Understanding Costs Insurance and Financial Realities
A lot of families assume the helicopter must be cheaper because it looks smaller and more direct. On long-distance interfacility transport, that assumption often doesn’t hold.
Why the cheaper-looking option may cost more
For long routes, fixed-wing aircraft are often more cost-effective because they move faster over distance and do so more efficiently. According to the fixed-wing vs rotary-wing cost analysis from FlyHAA, fixed-wing jets can cost $5-10/nm versus $20-50/nm for helicopters. The same analysis states that this can reduce total mission expense by 40-60% on flights over 500 nautical miles, and that fixed-wing medevac missions are approximately 25% cheaper overall.
That doesn’t mean fixed-wing is always the low-cost answer. It means the cost has to be matched to the mission profile. If the patient needs immediate short-range access where a helicopter can land close by, rotary-wing may still be the appropriate tool. But for planned long-distance transport, the economics often favor the jet.
Insurance questions families should ask early
Insurance coverage depends on medical necessity, policy terms, authorization, and documentation. Still, reimbursement often follows the same logic as transport planning. If one mode is better suited and more efficient for the clinical route, payers may view that more favorably.
When families call, I usually encourage them to clarify:
- Medical necessity documentation: Ask what physician notes and transfer rationale are required.
- Mode justification: Confirm whether the insurer wants explanation for fixed-wing versus rotary-wing selection.
- Ground transport inclusion: Verify whether bedside pickup and receiving-side ambulance are billed separately or as part of the mission.
- Companion policies: Ask whether a non-patient traveler affects covered services or administrative handling.
A practical primer on the moving parts is this guide to what impacts air ambulance cost and what you’ll be asked when you call.
Financial advice: don’t compare quotes without comparing route design, ground legs, medical crew level, and contingency planning. Two transports can sound similar and be operationally very different.
Cost is only one part of value
The least expensive line item isn’t always the lowest total burden. A transport that reduces delays, avoids multiple stops, supports the patient clinically, and creates fewer disruptions for the family can be the better value even before reimbursement is finalized.
That’s especially true when the transfer is long, the patient is fragile, or the receiving facility is far enough away that endurance and clinical space become central to the mission.
Your Decision Checklist Choosing the Right Aircraft
If you need a practical answer quickly, use this checklist. It won’t replace a medical and flight review, but it will point you toward the right questions.
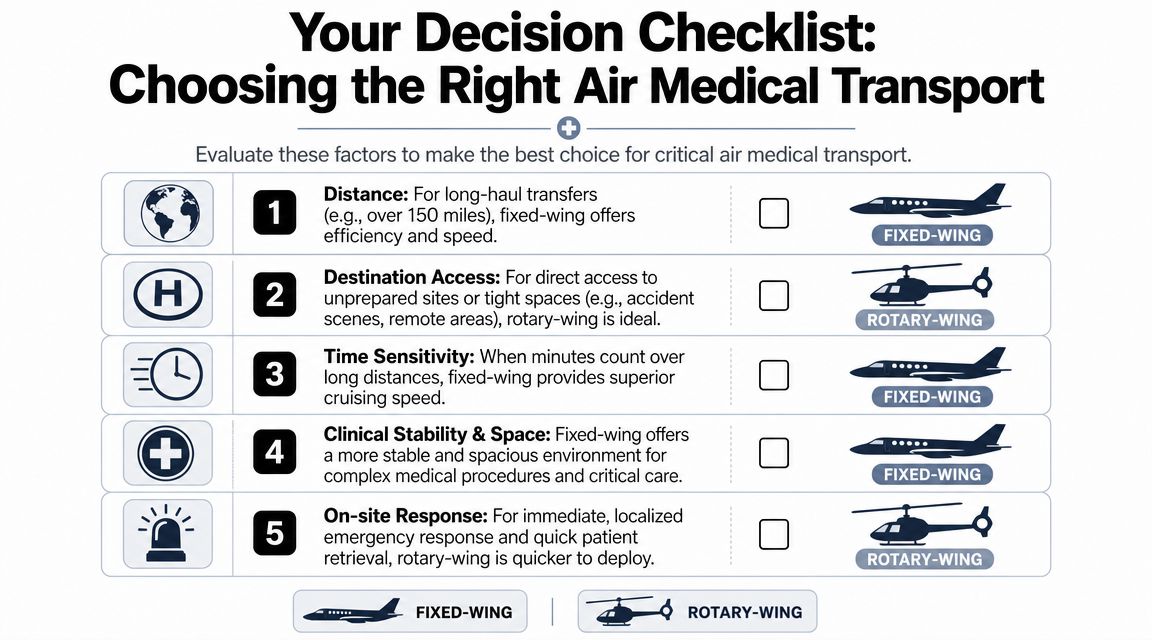
Start with the route
If the patient is traveling a long distance between hospitals, fixed-wing usually makes more sense. If the patient must be retrieved from a location without runway access and delivered nearby, rotary-wing may be the right fit.
Then look at the patient
Ask these in order:
Does the patient need a more controlled cabin environment?
If yes, fixed-wing deserves serious consideration.Will the crew need room for advanced monitoring or sustained in-flight care?
More cabin space usually helps.Is bariatric accommodation part of the plan?
Don’t leave this vague. Ask directly about loading, cabin access, and weight-related clinical setup.
Don’t forget the non-air segments
A bedside-to-bedside mission includes more than the flight. Confirm:
- Ground ambulance timing: Are both ends already coordinated?
- Hospital readiness: Has the receiving team accepted the patient and confirmed arrival logistics?
- Weather alternatives: If routing changes, who updates the family and hospital teams?
- Family travel plan: Is there room for an escort or companion, and what can they bring?
If a provider can explain the whole chain calmly and clearly, that’s usually a good sign the mission is being built correctly.
A simple rule of thumb
Use rotary-wing when direct access and short-range retrieval are the main need.
Use fixed-wing when the mission depends on distance efficiency, cabin stability, family accommodation, or long-range continuity of care.
The fixed wing vs rotary wing answer isn’t about which aircraft is more impressive. It’s about which one creates the safest, smoothest total transport.
Frequently Asked Questions for Families and Case Managers
Is bedside-to-bedside transport really one coordinated service
It should be. That means the sending location, ground ambulance legs, aircraft timing, receiving hospital coordination, and patient handoff are managed as one mission. If you’re arranging transport, ask who is responsible for each segment and who updates the family if timing changes.
What happens if weather changes after the mission is booked
A strong transport team reassesses routing, timing, and aircraft suitability. Sometimes that means a delay, a diversion, or an adjusted ground segment. Families should expect clear communication, not silence. Weather planning is part of safe transport, not a disruption to it.
Can a helicopter do a long-distance transfer if it stops to refuel
Technically, a route can be broken into segments. Practically, that often adds time, handoffs, and operational complexity. For long interfacility transfers, teams usually look for the option that better supports the patient over the full distance rather than the option that can complete it with more interruptions.
What if the patient’s condition changes before or during transport
The transport team should reassess whether the selected aircraft, crew configuration, and equipment remain appropriate. That may mean upgrading clinical support, changing timing, or altering the plan. The key question is whether the provider has the operational depth to adjust without losing control of the mission.
Can family members and personal items travel with the patient
Often yes, but policies vary by aircraft, medical requirements, and operator. Ask early about companions, medications, luggage, mobility aids, and any pet policy. Those details are easiest to solve before the crew is on the way.
Which is better in fixed wing vs rotary wing for most hospital transfers
For many planned long-distance hospital transfers, fixed-wing is the better fit. For short-range direct-access retrieval, rotary-wing may be the better fit. The patient’s condition, route, and destination access decide the answer.
If you’re evaluating a real transport need and want help thinking through the full bedside-to-bedside plan, Med Jets by Air Trek coordinates fixed-wing medical transport with ground logistics, clinical support, family accommodation, and 24/7 case review.