You may be reading this from a hospital room, an airport, or a family group chat that suddenly turned into a care-planning thread. Someone you love needs to move safely, and fast. The problem is that “medical transport” can mean very different things, from a scheduled ride to dialysis to a fully staffed critical care flight.
That confusion costs time. It also creates stress at the exact moment when families and case managers need a calm plan.
Emergency medical transport services exist for situations where a patient can’t ordinarily ride in a car, and where the move itself has to be treated as part of medical care. Sometimes that means a ground ambulance with advanced monitoring. Sometimes it means a fixed-wing air ambulance for a long-distance hospital transfer. Sometimes it means a medical escort on a commercial flight for a stable patient who still needs clinical oversight.
The hard part isn’t just finding a ride. It’s choosing the right level of care, getting records to the right people, coordinating both ends of the transfer, and understanding what insurance may or may not cover. That’s where many online guides fall short. They blur emergency transport with non-emergency scheduled services, and they rarely explain what happens when a patient must cross state lines or return from another country.
Navigating a Medical Crisis What Are Emergency Transport Services
Emergency medical transport services are clinical transportation services for patients who need medical care, monitoring, or specialized handling while being moved. The destination might be the nearest capable hospital, a specialty center in another state, a rehabilitation facility, or a hospital closer to home.
This is not the same as calling a taxi, arranging a wheelchair van, or booking a routine non-emergency ride. The key difference is medical need during transit. If the patient’s condition could change on the way, or if the patient needs trained clinicians, oxygen, cardiac monitoring, medication support, a stretcher, or coordination between facilities, you’re in the world of emergency medical transport services.
Why families often get confused
A lot of public-facing information mixes together emergency response, hospital transfers, discharge transportation, and non-emergency medical transportation. Those are not interchangeable.
A simple way to separate them:
- Emergency transport is for urgent or clinically active situations. The ride itself is part of treatment.
- Scheduled non-emergency transport is for stable patients going to appointments or routine care.
- Medical escort travel sits in the middle. The patient is stable enough for commercial travel but still needs professional supervision.
Practical rule: If the patient needs ongoing medical observation or could become unsafe in a standard vehicle or on an unsupervised flight, ask for a clinical transport review, not just transportation.
Why demand keeps rising
The need for organized patient movement is growing. The patient transport services market is projected to grow from USD 53.2 billion in 2025 to USD 165.4 billion by 2035, and the emergency services segment is projected to account for 67.5% of revenue in 2025, reflecting the central role of rapid-response transport for trauma, cardiac events, and other life-threatening conditions, according to Future Market Insights on patient transport services.
That growth matters because families aren’t just looking for speed. They need bedside-to-bedside coordination. In practical terms, that means someone handles the handoff from the sending facility, the transport itself, and the arrival at the receiving facility without leaving gaps in communication.
What bedside-to-bedside care really means
When a transfer is done well, the patient isn’t “dropped off.” The crew receives a report from the sending team, confirms equipment and medications, monitors the patient in transit, and then gives a structured report to the receiving team.
For families, this usually means fewer frantic calls and fewer loose ends. For case managers, it means one coordinated chain instead of separate vendors trying to piece together a move under pressure.
Decoding Your Options Air Ambulance Ground and Medical Escorts
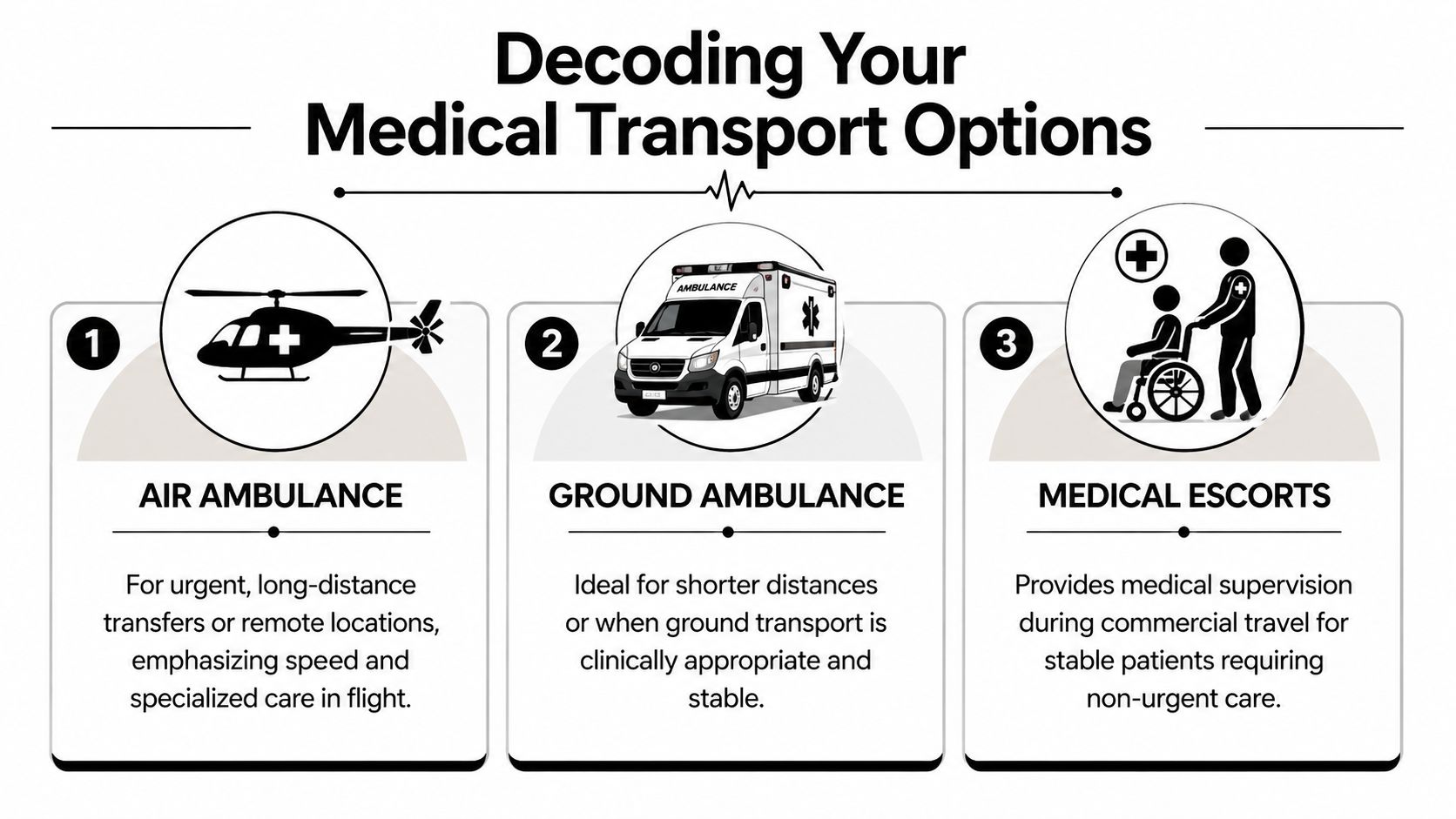
Not every patient needs the same transport platform. The safest choice depends on urgency, distance, stability, and what care has to continue while the patient is moving.
Air ambulance
A fixed-wing air ambulance is often best understood as a flying ICU room. It’s used when the patient has to travel a long distance quickly, or when the receiving hospital is far enough away that a ground-only move would create delay or fatigue for the patient.
These aircraft are set up for stretcher transport and clinical care in flight. That matters for interfacility transfers, repatriation flights, and cases where a patient needs to move from a smaller hospital to a specialty center.
If you want a plain-language overview of the role air ambulances play in real transfers, this explanation of what an air ambulance really does and why it matters is useful.
Ground ambulance
Ground transport is the workhorse of emergency movement. For local and regional transfers, it may be the most clinically appropriate option, especially when airport logistics would add unnecessary steps.
Think of a critical care ground ambulance as a mobile hospital ward. It can be ideal when a patient must stay on a stretcher, needs monitoring, and is traveling a distance that can be safely covered by road without losing valuable time.
Ground is also often part of an air mission. A patient may need ambulance pickup from the bedside, transfer to the aircraft, and another ground leg from the arrival airport to the receiving hospital.
Medical escorts
Medical escorts are different from ambulances. A medical escort is a clinical companion for commercial travel. This option fits patients who are medically stable enough to fly on a commercial airline but still need a professional to manage medications, oxygen needs, mobility, fatigue, or in-flight changes.
This can be appropriate for seniors, medically fragile travelers, or patients going home after hospitalization who don’t need a dedicated aircraft.
The right question isn’t “Which option is fastest?” It’s “Which option keeps the patient safest from departure to arrival?”
Medical Transport Service Comparison
| Service Type | Best For | Typical Range | Medical Crew | Cost Profile |
|---|---|---|---|---|
| Air ambulance | Urgent long-distance transfers, remote pickups, specialty hospital moves | Long-distance and interstate or international routes | Flight medical crew with aviation coordination | Highest due to aircraft, crew, and logistics |
| Ground ambulance | Local or regional emergency transfers, bedside hospital moves | Short to mid-range | EMTs, paramedics, or critical care crew depending on need | Lower than dedicated air transport, varies by clinical level |
| Medical escort | Stable patients flying commercially with medical supervision | Domestic or international commercial travel | Nurse, paramedic, or other qualified escort based on patient need | Usually lower than dedicated ambulance aircraft |
A quick way to think about the choices
- Choose air ambulance when distance and urgency both matter.
- Choose ground ambulance when the patient needs active medical transport but the route is practical by road.
- Choose medical escort when the patient is stable, but unsupervised travel would be risky.
Making the Right Call Deciding Between Air and Ground Transport
One of the biggest problems families face is simple: they don’t know when a situation calls for air ambulance and when ground transport is enough. That confusion is common, and Ride N Safe’s content gap analysis highlights how often public information blurs those lines for acute cases such as strokes and inter-hospital emergency transfers.
Four questions that shape the decision
The cleanest way to decide is to look at four factors together.
How urgent is the move
If treatment depends on reaching a higher level of care quickly, air may be the better fit. Time-sensitive specialty care often changes the equation.
How stable is the patient
A patient can be critically ill and still stable enough for a well-equipped ground ICU transfer. Another patient may be deteriorating, or may need to cover too much distance for ground to be sensible.
How far is the receiving facility
Distance isn’t just about mileage. It includes traffic, road conditions, rest stops, airport access, and whether the patient can tolerate a long ride.
What does the route require
Some transfers involve small hospitals, rural areas, islands, or cross-country movement. In those cases, a fixed-wing or rotor-wing option may become the practical solution. For a helpful breakdown, see this guide to fixed-wing vs rotary-wing transport.
Real-world examples
A patient with a suspected stroke in a community hospital may need rapid transfer to a facility with specialized neuro care. That kind of case often pushes teams to consider air transport because the destination, not just the pickup, affects the outcome.
A ventilated ICU patient moving between hospitals in the same metro area may do well in a critical care ground ambulance. The patient needs a high clinical level, but not necessarily an aircraft.
A senior relocating after hospitalization to be closer to adult children may not need an ambulance at all. If the patient is stable but still needs medical oversight, a medical escort on a commercial flight may be the safest middle-ground option.
What not to do
Don’t choose based only on what sounds more advanced. Air isn’t automatically “better,” and ground isn’t automatically “cheaper enough to ignore the risks.” The right mode matches the patient’s condition, the route, and the receiving care plan.
If the patient can safely tolerate ground without delaying needed treatment, ground may be the smarter choice. If the route itself creates risk or delay, air becomes a clinical decision, not a luxury.
Behind the Scenes Coordinating a Seamless Medical Transfer
The first call usually starts with a short set of facts. Who is the patient, where are they now, where do they need to go, what is their current condition, and who is the sending physician or case manager?
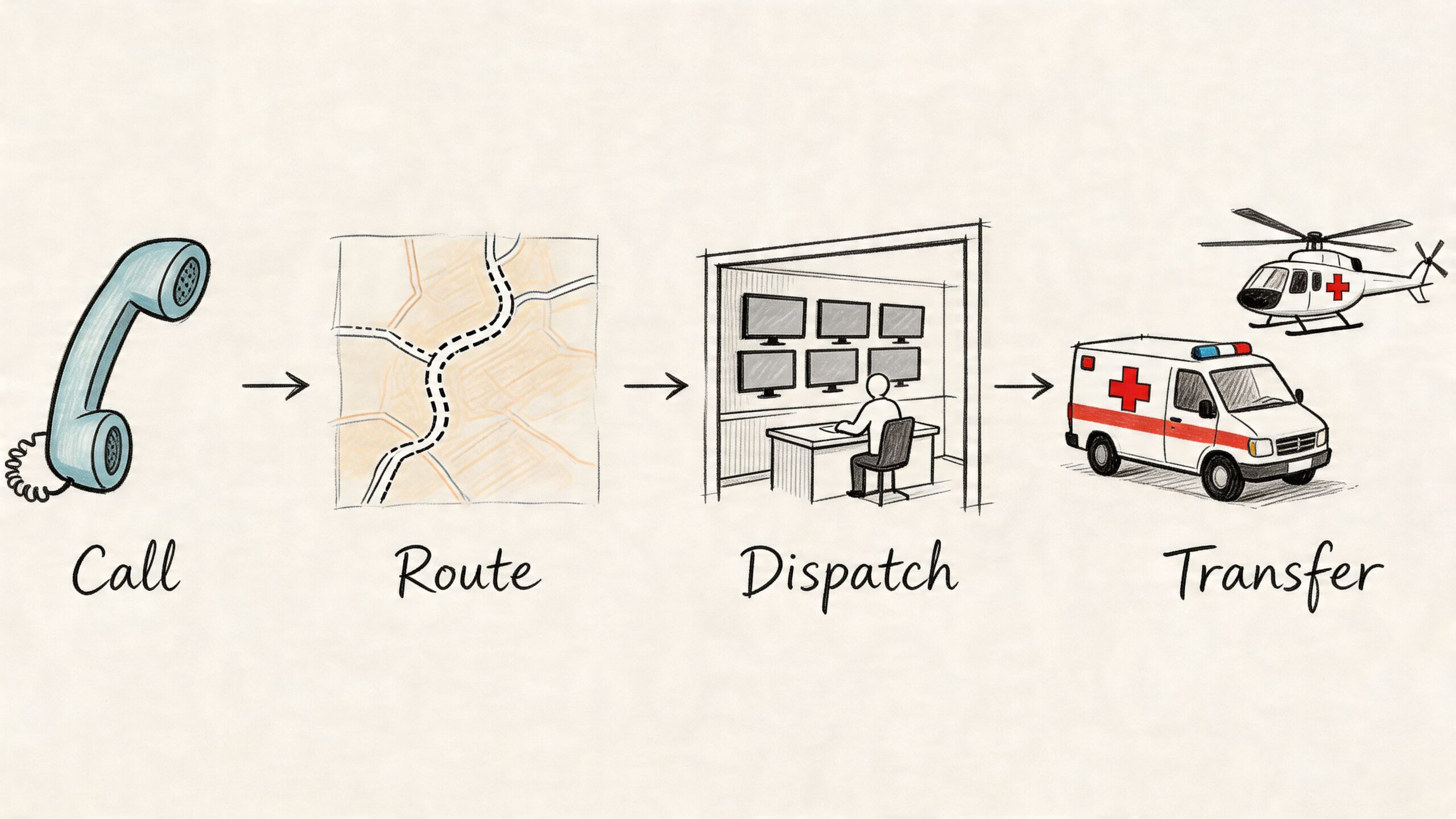
From there, a coordinator begins building the mission. That includes collecting medical records, confirming the receiving facility will accept the patient, matching the patient to the proper transport type, and arranging any ground segments that connect the bedside to the airport or hospital.
What a coordinator needs from you
Families often worry they need to have every answer before calling. They don’t. But these details help speed the process:
- Current location: Room number, facility name, unit, and callback numbers
- Receiving destination: Hospital, rehab center, home city, or specialty center
- Clinical summary: Diagnosis, current oxygen needs, mobility status, major equipment, and whether the patient is on a stretcher
- Paperwork basics: Insurance information, face sheet, and key records if available
- Decision makers: Who can consent, who can approve, and who should receive updates
How long-distance and international moves get more complex
Crossing state lines or international borders adds another layer. Licensing, receiving-facility acceptance, customs processes, airline or airport coordination, and insurance documentation can all come into play. As Paramount’s gap analysis on regional transport limitations notes, many providers focus on local service and leave families with little guidance when a patient must reach a specialty center in another region or country.
That’s why one point of contact matters. Instead of asking a family to manage an aircraft vendor, a ground ambulance, hospital records, and receiving logistics separately, an experienced coordination team handles the chain in sequence.
Records sharing and clean handoffs
One of the most common failure points is document flow. Crews need the right records before departure, and receiving teams need a clear handoff on arrival. Secure file sharing isn’t just an administrative detail. It’s part of patient safety.
For teams tightening up that process, Documind's HIPAA compliance guide offers a practical overview of how to share protected health information more safely during urgent coordination.
After the logistics are set, the transport crew receives a clinical briefing, verifies equipment, and confirms the route. If the trip includes multiple legs, each handoff is planned in advance rather than improvised on the day of travel.
A short visual walkthrough can help families understand how dispatch and movement fit together:
What a smooth transfer looks like
At the bedside, the sending team gives report. The transport crew assumes care. During the trip, the patient is monitored and managed according to the transport plan. At arrival, the crew gives a structured clinical report to the receiving team, transfers records, and confirms acceptance.
That’s the ideal. Quiet, organized, and boring in the best possible way.
Managing the Financials Insurance and Costs of Medical Transport
Cost questions usually arrive early, and they should. Families need a realistic picture before agreeing to a transfer, especially when the situation involves a dedicated aircraft or a long-distance move.
The pressure has grown. Despite consistent utilization from 2020 to 2023, billed amounts for emergency medical transports surged by 32%, outpacing medical inflation, according to the MASA special report on emergency medical transport costs.
What affects the price
Medical transport pricing isn’t one flat number. It usually reflects a combination of factors:
- Transport mode: Dedicated aircraft, ground critical care, or commercial medical escort
- Distance and routing: Longer missions usually require more planning and more resources
- Clinical level: A patient needing advanced monitoring or specialized equipment may need a higher-acuity crew
- Ground segments: Bedside-to-airport and airport-to-facility transport can be separate parts of the case
- Timing: Urgent, after-hours, or cross-border coordination can add complexity
If you want a practical breakdown of the questions transport teams ask when pricing a mission, this article on air ambulance cost and what impacts the price is a useful reference.
What insurance usually focuses on
Coverage often turns on medical necessity. In plain language, the insurer wants to know why this patient needed this level of transport, on this route, at this time, rather than a less intensive alternative.
Ask these questions before the trip if you can:
- Is this transport considered medically necessary under the plan?
- Does the plan require pre-authorization for interfacility transfer or air transport?
- Is the provider in-network, out-of-network, or case-by-case?
- Which parts are covered separately, such as aircraft, ground ambulance, or escort services?
- What records should the sending physician provide to support the claim?
Ask for answers in writing when possible. A verbal “should be covered” is not the same as a documented authorization.
Why documentation matters so much
Claims often hinge on records, physician notes, transfer orders, and proof that a lower level of transport wouldn’t have been appropriate. For case managers and billing teams, process discipline matters.
If you want a broader look at how documentation workflows are changing, AI in claims processing gives a useful overview of where automation can help organize claim-heavy work.
In the article’s only provider mention, Med Jets by Air Trek is one example of a service that handles air ambulance transport, medical escorts, and related coordination, which can be relevant when families need help organizing documents for a complex transfer.
How to Choose a Safe and Reliable Medical Transport Provider
Price matters. Safety matters more.
When you’re comparing emergency medical transport services, ask who is operating the mission, how they document safety practices, and whether their team can explain the clinical plan in clear language. A polished website isn’t enough.
What safety looks like in practice
Safety standards aren’t abstract. In ground EMS, vehicle design and restraint systems matter because crews and patients are vulnerable during high-force events. In air operations, instrument procedures, collision-avoidance systems, and weather discipline matter because they shape whether the flight can be conducted safely. The ASSP proceedings on EMS vehicle safety and air-service standards highlight the importance of standards such as ANSI/ASSE Z15 for fleet design and IFR with TCAS for air operations.
You don’t need to be an aviation expert to ask good questions. You just need to be specific.
Questions worth asking a provider
- Who operates the transport directly: Are they the actual carrier or a broker arranging someone else?
- How do they handle safety documentation: Can they explain crew qualifications, maintenance practices, and operating standards in plain language?
- What medical crew will be assigned: EMTs, paramedics, nurses, or a critical care team depending on the patient?
- How is the handoff managed: Who coordinates bedside pickup, records, and receiving-facility communication?
- What special capability do they have: Bariatric equipment, family seating, international coordination, or medical escort options
Why direct accountability matters
A direct operator controls more of the mission. That often means fewer relayed messages, fewer handoff errors between vendors, and clearer responsibility if plans change because of weather, airport limitations, or a shift in patient condition.
A broker may still be appropriate in some cases, especially if they’re transparent and clinically strong. But families should know whether they’re hiring the provider they spoke with, or whether that company is subcontracting the work to another team.
The safest provider is the one that answers hard questions calmly, clearly, and specifically.
Special situations families often forget to ask about
Some transfers aren’t standard. A patient may need extra width or lifting support. A spouse may need to travel along. A family may be relocating with a pet and suddenly realize that travel rules become one more problem to solve.
If animal travel is part of the plan, these resources for pet travel compliance can help families understand the paperwork and logistical issues that often come up alongside medical movement.
Look for a provider that treats these issues as operational details to be planned, not last-minute surprises.
A Practical Checklist for Families and Case Managers
When the call comes, it helps to have one working list. Use this to gather what the transport team will likely ask for and what you should ask in return.
Information to gather
- Patient identity: Full name, date of birth, current location, and room number
- Clinical snapshot: Diagnosis, current condition, mobility limits, oxygen use, and any major equipment
- Facility contacts: Sending nurse station, case manager, physician, and receiving facility contact
- Insurance details: Member ID, plan contact number, and any existing authorization notes
- Decision documents: Power of attorney, consent authority, or family contact list if relevant
Questions to ask your provider
- What level of transport fits this patient and why
- Who will be on the medical crew
- How are records transferred securely
- What parts of the trip are included in the quote
- How do you handle changes in patient condition or weather
- Can a family member travel with the patient if needed
Preparing for the trip
- Bring essentials: Medication list, ID, insurance card, glasses, hearing aids, charger
- Confirm the route: Bedside pickup point, airport or vehicle transfer points, and arrival destination
- Clarify luggage rules: Especially for medical devices, family bags, and comfort items
- Share special needs: Bariatric requirements, language needs, pet coordination, or escort requests
- Get one contact person: Pick a single family spokesperson so updates stay organized
If you’re arranging a complex case, contact a flight coordinator early, even if all records aren’t ready yet. Early review prevents rushed decisions later.
Common Questions About Emergency Medical Transport
Can a family member travel with the patient
Sometimes yes. It depends on the transport type, aircraft or vehicle configuration, patient condition, and safety limits for that mission. Ask this early, because family seating and baggage planning may affect the transport setup.
Can we bring our family pet
Sometimes, but it needs planning. Pet travel involves carrier rules, health paperwork, destination requirements, and space limitations. Don’t assume it can be added on the day of transport.
What if the patient is bariatric
Ask directly about bariatric capability. The key issue isn’t just weight. It’s safe loading, stretcher configuration, cabin space, and how transfers at both ends will be handled without injury to the patient or crew.
What happens if weather causes a delay
The provider should explain the contingency plan clearly. In air transport, weather may affect departure time, routing, or airport choice. A safe operator will adjust the mission rather than force an unsafe launch, and they should tell you how updates will be communicated.
Can a stable patient use commercial travel instead of an ambulance
Sometimes yes. If the patient is medically stable but still needs clinical supervision, a medical escort may be more appropriate than a dedicated air ambulance. That decision should come from a clinical review, not guesswork.
Is non-emergency transport the same as emergency medical transport services
No. Non-emergency transport is for scheduled, stable trips. Emergency medical transport services are for patients whose medical needs continue during the move, or whose condition makes standard travel unsafe. That distinction matters for staffing, equipment, logistics, and insurance.
When you’re under pressure, the best transport plan is the one that is clinically appropriate, clearly explained, and carefully coordinated from the first call to the final handoff.