When a doctor says your child needs an air medical transport, the room can seem to narrow all at once. You hear important words, but your mind jumps to simpler questions. Is my child safe? Who will be with them? What happens in the air? Can I help?
Those questions are normal. I’ve found that families feel a little steadier when they understand what a pediatric flight nurse does. This role isn’t just about riding on an aircraft with medical equipment. It’s about bringing skilled pediatric critical care into a moving, noisy, tightly controlled environment, then guiding a child safely from one bedside to another.
If you’re reading this while trying to make decisions quickly, start with this reassurance. A pediatric medical flight is built around preparation, monitoring, communication, and calm problem-solving. The equipment matters. The aircraft matters. But the person watching your child’s breathing, circulation, comfort, and response every minute matters just as much.
When Your Child Needs to Fly for Medical Care
The moment usually starts with a gap between what your child needs and what the current hospital can provide. Maybe your baby needs a higher level NICU. Maybe your child needs pediatric surgery, pediatric intensive care, or a specialist at another hospital. The transfer isn’t about inconvenience. It’s about getting your child to the right team fast and safely.

A lot of parents hear “flight” and picture speed alone. Speed matters, but that’s only part of it. The bigger issue is continuous critical care during the transfer. A child who is stable in a hospital bed still needs careful support while moving through hallways, ambulances, runways, and an aircraft cabin. That’s why the flight team plans each step before the child ever leaves the room.
You may also hear people talk about the medical golden hour in emergency transport. In plain language, that means early access to the right care can shape what happens next. For children, especially those with serious illness or injury, the transport itself becomes part of treatment.
Why families often feel overwhelmed
Parents usually have to absorb several realities at once:
- A sudden change in plan: You expected treatment in one hospital, and now another facility is involved.
- A new team: Nurses, doctors, dispatch staff, and pilots may all enter the conversation quickly.
- Unfamiliar equipment: Monitors, pumps, oxygen, ventilators, and transport stretchers can look intimidating.
- Questions about your role: You may wonder whether you can ride along, what to bring, or how to comfort your child.
The transfer can feel fast from the family’s side, but the clinical team is slowing things down where it counts. They check details, equipment, medication, and communication before movement starts.
The pediatric flight nurse is often the person who turns a frightening process into something understandable. They explain what they’re watching, what they’re adjusting, and why certain steps can’t be skipped. For many families, that calm explanation is the first moment they feel they can breathe again.
Who Is a Pediatric Flight Nurse
A pediatric flight nurse is a registered nurse with deep critical care experience who specializes in transporting infants and children during medical flights. These aren’t brand-new nurses learning on the job. They are usually seasoned ICU clinicians who already know how fast a child’s condition can change and how to respond without delay.
Research highlighted by the National Pediatric Readiness Project found that ill children treated by pediatric specialists had a 76% lower mortality rate, and injured children had a 60% lower mortality rate compared with care by general providers, which helps explain why pediatric specialization matters so much in transport situations (KOAA report covering pediatric specialist outcomes). That same reporting also notes that pediatric flight nurses often need at least five years of ICU experience before qualifying.
Think of it as an ICU in motion
Families often ask, “So are they just a nurse who travels with my child?” Not quite.
A better picture is this. A pediatric flight nurse works inside a moving ICU. The room is smaller. The noise is louder. The child may be on oxygen, medication infusions, or a ventilator. The nurse has to assess, treat, and anticipate problems while the aircraft is climbing, descending, vibrating, and working on a schedule tied to weather, safety, and distance.
That’s why the role requires a different mindset than bedside nursing alone.
- Independent judgment: The nurse can’t just step into a hallway and pull in a full hospital team.
- Pediatric focus: Children aren’t small adults. Their airway, circulation, medication dosing, and stress responses are different.
- Transport awareness: The nurse has to think about altitude, cabin conditions, securing equipment, and what could change mid-flight.
What makes this role different from other clinicians
The pediatric flight nurse often works alongside other transport professionals, but their nursing role is distinct. They combine bedside critical care, pediatric emergency response, and transport logistics in one continuous job.
Here’s what that often looks like in practice:
| Role need | What the pediatric flight nurse does |
|---|---|
| Assess instability | Interprets subtle changes in breathing, skin color, pulse, comfort, and responsiveness |
| Manage treatment | Adjusts medications, oxygen, and other support within protocol and the transport plan |
| Protect continuity | Carries key clinical information from the sending team to the receiving team |
| Support the family | Explains what’s happening in plain language during a highly emotional moment |
Practical rule: A strong pediatric flight nurse is always doing two jobs at once. Caring for the child you can see, and preparing for the problem that could happen next.
Parents also ask whether this role is mostly for dramatic emergencies. Sometimes it is. But many pediatric flights involve inter-facility transfers where the child needs advanced care, closer monitoring, or access to a pediatric specialty center that isn’t available locally. In those moments, the nurse is both a critical care clinician and a steadying presence for the people who love that child most.
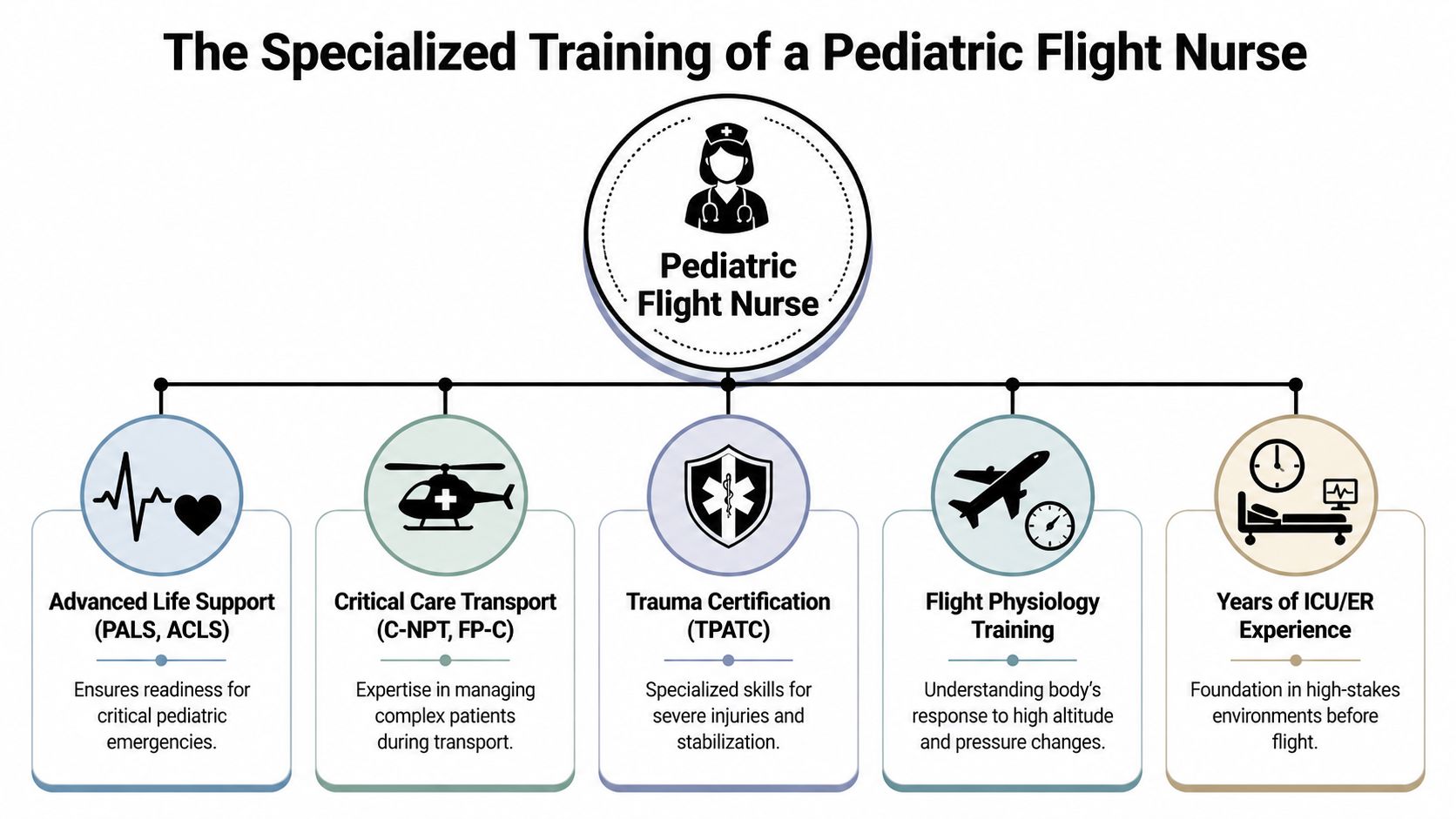
The Specialized Training of a Pediatric Flight Nurse
By the time someone becomes a pediatric flight nurse, they’ve already built a strong foundation in high-acuity nursing. Flight work adds another layer. It asks that nurse to keep the same level of clinical precision while adapting to altitude, vibration, tight spaces, and limited hands-on help.
The profession has grown sharply. The Certified Flight Registered Nurse program, known as CFRN, saw annual initial certifications increase by an average of 22% since 2012, with a fourfold rise from 2012 to 2022. The same survey found that 35% of CFRNs have more than 10 years of flight nursing experience (BCEN 2022 CFRN Pulse Survey findings). For families, that matters because it points to a field with a substantial number of experienced clinicians, not a niche built on improvisation.
You can also review air ambulance team qualifications and training standards if you want a better sense of what established programs look for.
What the acronyms mean for your child
Families get handed a lot of letters during a crisis. Here’s the plain-English version.
- CFRN: This means the nurse has validated knowledge specific to flight nursing. It focuses on the challenges of treating patients safely in the air.
- PALS: Short for Pediatric Advanced Life Support. This prepares clinicians to recognize and treat pediatric emergencies such as breathing failure, shock, and cardiac arrest.
- NRP: Short for Neonatal Resuscitation Program. This is especially important for newborns and fragile infants who may need immediate support with breathing and circulation.
Those credentials aren’t just resume items. They tell you the nurse has trained for the exact kinds of problems parents worry about most.
Flight training changes how care is delivered
An aircraft cabin can affect the body in ways that are easy to overlook. Less available oxygen, motion, noise, and vibration can all increase the stress on a child who is already sick. A trained pediatric flight nurse plans around that.
For example, they don’t just “bring the hospital monitor along.” They adapt care to transport conditions by checking how lines are secured, how equipment will be powered, how the child will be positioned, and what to do if a reading changes during takeoff or descent.
Advanced transport training teaches a nurse to think one move ahead. If a child needs suction, medication, warmth, or a ventilator adjustment, the nurse plans for that before the cabin environment makes simple tasks harder.
Experience still matters most
Certifications are important, but experience is where judgment becomes calm. A pediatric flight nurse learns how to notice small warning signs quickly. A child becoming quieter, breathing a little harder, or showing a subtle color change can mean a lot. In transport medicine, noticing those changes early is one of the most valuable skills anyone can bring onboard.
What Happens During a Pediatric Medical Flight
Once a flight is approved, families often ask the same question in different ways. What will you do for my child from the first hospital to the next one? The answer is usually more detailed and more reassuring than parents expect.
Think of the transport as a chain of care with no gaps. The flight nurse doesn’t “pick up” a patient the way a driver picks up a passenger. They receive a medical handoff, assess the child directly, stabilize what needs attention, prepare equipment, monitor throughout the flight, and then give a structured handoff at arrival.
Evidence from specialized transport teams shows that pre-flight stabilization reduces in-transit deteriorations by 40% to 50% (Life Flight Network clinical transport guidance). That’s why transport teams don’t rush out the door the second they arrive. They work methodically first.
Before the aircraft leaves the ground
Let’s use a simple example. A critically ill infant needs transfer to a pediatric center for higher-level care. Before anyone moves that baby, the pediatric flight nurse checks the essentials.
They review the diagnosis, medications, recent vital signs, oxygen needs, lab concerns, and airway status. If the infant is in an isolette, the nurse checks temperature support, line security, monitor leads, and whether the transport setup will stay stable during movement.
The nurse may also adjust care before departure. Specialized teams use Pediatric Advanced Life Support principles during transport and may fine-tune vasoactive medications or ventilator settings. In the flight environment, teams may adjust mechanical ventilation to maintain PaO2 above 60 mmHg and EtCO2 between 35 and 45 mmHg as cabin conditions change, according to the same clinical guidance linked above.
In the air
Inside the aircraft, the nurse keeps doing what good ICU nurses always do. Watch trends, not just snapshots.
That means tracking breathing, heart rate, blood pressure, oxygenation, comfort, response to medication, and any sign that the child is tiring or becoming unstable. The difference is that all of this happens in a compact space with aircraft noise and motion in the background.
If you’re comparing aircraft types, this overview of fixed-wing versus rotary-wing medical transport can help clarify why some pediatric transfers are done by jet rather than helicopter.
A short video can make the environment easier to picture.
Why the in-flight environment changes care
An aircraft cabin is a bit like caring for a child inside a small treatment room that hums, shakes, and changes pressure. Even a well-supported child can react differently there.
That’s why the nurse pays close attention to things families may not notice right away:
- Breathing support: Oxygen and ventilator settings may need adjustment as altitude changes the environment.
- Medication delivery: IV pumps must be secured, accurate, and easy to monitor during vibration.
- Positioning and safety: Infants in isolettes and children on stretchers must be secured without compromising comfort or access.
- Early signs of trouble: Capnography, oxygen saturation, heart rhythm, and physical assessment all help the nurse spot problems early.
A well-run pediatric transport rarely looks dramatic. The best flights often feel quiet because the team prepared carefully and keeps correcting small issues before they become big ones.
When the aircraft lands, the nurse’s work doesn’t stop. The final handoff is part of treatment. The receiving team needs a clear summary of what happened before flight, during transport, and on arrival so they can continue care without losing momentum.
Coordinating Care from Bedside to Bedside
Families sometimes think of air medical transport as a series of handoffs. One hospital ends its role. A flight team takes over. Then another hospital starts. In reality, the safest transports feel more like one connected line.
The pediatric flight nurse often serves as the air traffic controller for patient care. Not for the aircraft itself, of course, but for the medical mission. They help make sure the sending physician, bedside staff, transport team, pilots, dispatch, and receiving hospital are all working from the same picture.
The communication chain
A smooth transport depends on clear, repeated communication. The nurse helps close the gaps that can happen when many professionals are moving quickly.
A typical chain may look like this:
- Sending physician and bedside team share the child’s diagnosis, current treatment, recent changes, and reason for transfer.
- Flight nurse confirms the child’s condition, equipment needs, medication plan, and transport priorities.
- Pilot and operations staff coordinate the practical side of the mission, including route, timing, and safety factors.
- Receiving physician and unit prepare for arrival based on the child’s needs and any updates from transport.
Every one of those conversations matters. If a medication was changed shortly before departure, the receiving team needs that information. If the child needed more respiratory support in transit, that detail can shape what happens the moment the stretcher enters the next unit.
Why continuity matters to families
When communication is done well, parents notice something important. Fewer surprises.
You’re less likely to hear conflicting information. You’re less likely to repeat the same history over and over. And you’re more likely to feel that someone is carrying the full story of your child, not just a single task.
Good pediatric transport isn't only clinical skill. It's memory, structure, and disciplined communication under pressure.
What bedside to bedside really means
“Bedside to bedside” sounds like a slogan until you watch it happen. It means the child is treated as one ongoing patient journey, not separate events stitched together. The pediatric flight nurse helps preserve that continuity by carrying forward the details that can easily get lost in motion.
That includes things families care immensely about:
- Comfort details: What soothes the child, what frightens them, and how they’ve been tolerating movement.
- Parent concerns: Recent changes the family noticed, even if they seem small.
- Clinical nuance: Trends, not just numbers. Was the child steadily improving, or were they stable only after significant support?
That kind of coordination is often invisible when it works well. That’s exactly how it should be.
Your Role in a Smooth and Safe Medical Transport
Parents often feel helpless during a transfer. You’re not helpless. You may not be managing oxygen, medications, or aircraft logistics, but you still have an important role. You know your child. You can help the team understand what calms them, what scares them, and what practical details might matter during the trip.
There’s also a real support gap around the emotional side of pediatric air transport. Guidance for families on reducing fear before, during, and after a flight is often limited, even though psychological preparation can improve overall outcomes, as noted in guidance for concerned parents about pediatric transport.
What you can do before transport
Some of the most useful parent actions are simple.
- Bring comfort items: A favorite blanket, stuffed animal, pacifier, or small familiar object can help anchor a child in an unfamiliar setting.
- Keep your explanation short: Younger children usually do better with simple truth. “We’re taking a special airplane to help you get to the doctors who know exactly how to care for you.”
- Share routines: Tell the team if your child settles with certain words, songs, positions, or sensory supports.
- Pack essentials, not everything: Medications, identification, phone chargers, and one small bag are usually more useful than several large bags in a transport setting.
If your child is old enough to understand, avoid long technical explanations. Children often do better when they know who will stay with them, what they might hear, and that the equipment is there to help.
Questions worth asking
A worried parent doesn’t need to “stay out of the way” completely. Clear questions are appropriate and useful.
Here’s a practical checklist:
| Question Category | Specific Question to Ask |
|---|---|
| Clinical team | Who will be caring for my child during the flight? |
| Pediatric capability | What pediatric equipment will be onboard for my child’s age and condition? |
| Parent involvement | Can a parent travel with the child, and if not, how will updates be given? |
| Monitoring | How will my child be watched during the flight? |
| Comfort | What can we bring that may help calm our child? |
| Handoff | Who will receive my child when the aircraft lands? |
| Communication | How will the receiving hospital be updated during transport? |
| Special circumstances | If my child has complex needs, what additional preparations are made? |
Helping your child emotionally
Children take cues from adults. That doesn’t mean you need to hide your feelings perfectly. It means your tone helps shape the room.
Try to:
- Use calm repetition: “You’re safe. The team is helping you. I’m here.”
- Name what they’ll notice: “It may be noisy. You’ll see lights and hear machines. That’s normal.”
- Avoid accidental alarm: Instead of “Don’t be scared,” try “The nurse will stay close and explain things.”
- Ask about family policies: Some programs can accommodate a parent companion, and some family-centered services may even discuss special travel needs such as pets in certain circumstances.
Children usually cope better when the adults around them sound organized, honest, and steady.
If your child seems more upset after the flight, that doesn’t automatically mean something went wrong. Medical transport can be stressful. A child may become clingy, quiet, tearful, irritable, or have trouble sleeping. If those changes concern you, tell the receiving care team. Emotional recovery deserves attention too.
Common Questions About Pediatric Air Transport
Families and case managers often need quick answers. These are some of the questions that come up most often.
Why would a child go by jet instead of helicopter
It depends on distance, weather, clinical needs, and where the child is going. For longer inter-facility transfers, a fixed-wing aircraft such as a medical jet may be the better fit because it’s designed for distance and can support a more structured cabin setup for critical care. Helicopters are often useful for shorter routes or scenes where direct access matters more than range.
Can a parent always fly with the child
Not always. It depends on the child’s condition, aircraft setup, safety limits, and the provider’s policies. The best approach is to ask early and clearly. If a parent can’t ride along, the team should explain how updates will be handled and where reunification will happen.
Will my child be asleep during the flight
Sometimes yes, sometimes no. Some children are already sedated because of their medical condition or treatment. Others remain awake and are comforted, monitored, and supported throughout the trip. The plan depends on what is safest and most appropriate medically, not on making the flight seem easier from the outside.
What if my child has a very complex condition
That’s where advanced transport capability matters most. Some teams can consult with specialists in real time during flight. Telemedicine is beginning to change pediatric transport by allowing flight nurses to connect with remote specialists during complex cases, especially in rural situations, though specific adoption rates and condition-by-condition data are still emerging (overview of telemedicine in pediatric transport).
What should I listen for when choosing a provider
Listen for specifics. You want to hear clear answers about pediatric experience, equipment, bedside-to-bedside coordination, communication with the receiving hospital, and family support. If the answers stay vague, keep asking.
A strong provider should be able to explain:
- Who staffs the mission
- How pediatric needs are handled
- What happens before takeoff
- How updates are shared
- How the bedside handoff is completed
Is it normal to feel shaken even after a safe flight
Yes. Families often stay in “crisis mode” even when the transport goes well. That reaction is common. Once your child reaches the receiving hospital, you may finally have room to feel how stressful the transfer was. Ask questions, write things down, and let the team know what you still don’t understand.
When you need pediatric air ambulance support, calm coordination matters as much as speed. Med Jets by Air Trek has provided complete medical transportation solutions since 1978, with bedside-to-bedside coordination, experienced clinical crews, and family-centered support available around the clock.