A dedicated fixed-wing medevac flight usually costs $25,000 to $75,000 domestically, and transatlantic flights can run $90,000 to $220,000. If you're arranging transport right now, the number you need to plan for is the all-in cost, not just the airplane, because ground transfers, medical crew, and specialized equipment can change the final quote fast.
You’re probably reading this because someone you care about is in the wrong hospital, too far from home, or not stable enough for normal travel. That’s when families get hit with two problems at once. First, a medical crisis. Second, a bill they don’t understand.
I’ve seen the same pattern over and over. A case manager needs a transfer today. An adult child wants a parent moved closer to family. A spouse is trying to compare a dedicated jet with a commercial medical escort while doctors are waiting for an answer. In that moment, vague articles aren’t useful. You need to know what drives the cost of medevac flight, what questions to ask, and where hidden charges show up.
The hard truth is that medevac pricing is rarely simple. The good news is that it can be understood. If you know how quotes are built, you can tell the difference between a fair all-inclusive transport plan and a low number that turns into multiple bills later.
Air medical transport has been handled by family-run operators for decades, and companies that have been doing this since 1978 tend to understand the practical side better than anyone. Experience matters because this isn’t just an aircraft booking. It’s medical coordination, airport timing, bedside handoff, ground logistics, and insurance paperwork, all under pressure.
The Urgent Call No One Expects
The call usually sounds the same.
Your father fell while traveling. Your wife had a stroke away from home. Your patient has outgrown what a small facility can manage. The doctor says, “We need to transfer now,” and suddenly you’re being asked about aircraft, medical records, and payment responsibility before you’ve even processed what happened.
That’s why families freeze when they hear the first quote. Not because air medical transport is unnecessary, but because the number arrives without context.
What families usually misunderstand
It is often assumed that the flight is the whole service. It isn’t. In a real transfer, someone has to coordinate the sending hospital, the receiving hospital, the ambulance on the ground, the airport handling, the onboard care team, and the handoff on arrival.
Practical rule: If a quote sounds simple, ask what is not included.
That’s especially important when the patient can’t tolerate delays, layovers, extra transfers, or a long drive to and from commercial terminals. In those cases, the cheapest-looking option can become the most disruptive one.
What case managers need immediately
If you’re a discharge planner or hospital case manager, you need four answers fast:
- Clinical fit: Can the patient fly safely on a dedicated jet, or is a commercial medical escort enough?
- Operational timing: How quickly can the operator mobilize aircraft, crew, and ground transport?
- Bed-to-bed scope: Does the quote include both ground legs and hospital coordination?
- Financial clarity: Is this a single coordinated invoice, or will the family get separate bills?
Long experience matters. Teams that have coordinated transports since 1978 usually know what slows transfers down, what documents insurers ask for, and where families get blindsided. That doesn’t make the flight cheap. It makes the process clearer.
Understanding Medevac Price Ranges
A family usually hears one number and assumes that is the flight price. In practice, the actual question is the all-in transport cost from bedside to bedside.
For a dedicated fixed-wing air ambulance, families should expect a broad domestic range that often starts in the tens of thousands and climbs sharply for longer routes, higher-acuity patients, and more complicated coordination. Pricing guidance from Paraflight’s fixed-wing medevac pricing overview also notes that fixed-wing transport often makes more operational and financial sense on longer trips, especially when helicopters would require extra stops.
That range exists for a reason. You are not buying a seat. You are paying for an aircraft, a medical crew, dispatch coordination, airport handling, and two ground transfers that have to line up without delays.
Domestic flights
Domestic pricing usually splits into two very different categories. A dedicated medevac jet costs more upfront, but it gives you control. The aircraft departs on your schedule, the care team is assigned to your patient, and the transport can be arranged as one coordinated mission.
A commercial medical escort costs far less when the patient is stable enough to fly on a commercial airline. That option works well for patients who can sit up, tolerate airport screening, handle longer transfer times, and do not need intensive monitoring in the air. If you want a practical overview of the questions operators ask before quoting, review what impacts air ambulance pricing and what families are asked when they call.
Here is the decision rule I give families and case managers. Choose a dedicated jet when speed, privacy, infection control, pain control, or continuous medical support will change the patient’s safety or comfort. Choose a commercial medical escort when the patient is medically stable and the main goal is to reduce cost.
International and transatlantic flights
International flights get expensive fast because the quote expands beyond flight time. Analysts at Global Rescue outline that difference clearly in their medical jet transport cost guide, with transatlantic transport rising far above typical domestic trips.
Families should expect extra cost from permits, customs handling, longer crew time, fuel planning, airport fees, and overnight logistics if the routing requires it. Ground ambulances on both ends can also be harder to coordinate internationally, especially if the receiving facility has narrow intake windows or document requirements.
Why the lowest quote is often the wrong one
The cheapest number on paper often excludes the parts that cause the most stress later. Ask whether the quote includes bedside pickup, bedside delivery, ambulance transfers, oxygen, airport handling, waiting time, and after-hours coordination.
That is the hidden-fee problem.
A useful way to frame it is to compare it to other high-service transport. If you have ever reviewed a guide to executive chauffeur pricing, you have seen the same pricing logic at a simpler level. The vehicle is only part of the bill. Timing, route changes, standby time, and service level change the final total.
Teams that have handled air medical transports since 1978 usually spot these cost traps early and explain them before the family commits. That experience does not make the transport inexpensive. It makes the quote honest.
An Itemized Breakdown of Medevac Costs
A medevac quote is only useful if it shows the full move, not just the flight.
Families get into trouble when they compare a flight number to an all-in transport number. Those are not the same thing. A real bedside-to-bedside transfer can include the aircraft, medical crew, ground ambulances, airport handling, records coordination, oxygen, specialty equipment, and timing-related charges if the handoff runs late or the receiving facility is not ready.
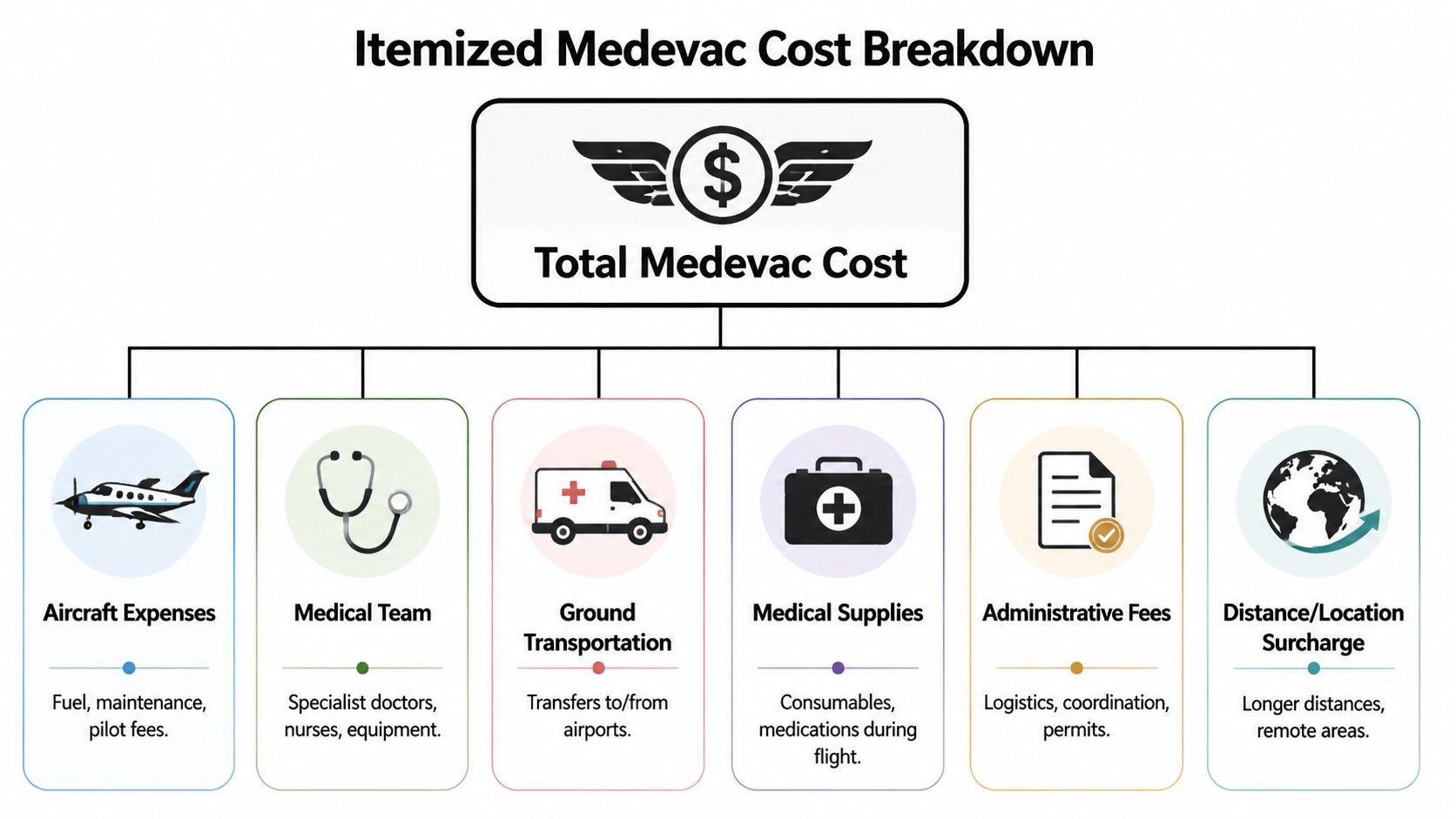
Typical medevac cost components
| Cost Component | Typical Price Range (USD) | What It Covers |
|---|---|---|
| Base flight charge | Varies by mission | Aircraft positioning, flight crew, standard onboard setup, dispatch |
| Medical team | Varies by acuity | RN, paramedic, respiratory therapist, or higher-acuity clinical staffing |
| Specialty equipment | Varies by need | Ventilator setup, neonatal gear, bariatric equipment, pumps, monitors |
| Ground ambulance legs | Often separate | Hospital-to-airport and airport-to-hospital transport |
| Airport and handling fees | Often separate or bundled | Ramp access, handling, coordination, after-hours arrangements |
| International paperwork and permits | Case by case | Overflight permits, customs coordination, clearances, documentation |
What you are actually paying for
The aircraft is the biggest line item, but it is not the whole service. You are paying for a coordinated medical move under time pressure. That includes clinical review, aircraft selection, staffing, dispatch, communication with both facilities, and a realistic plan for every handoff.
That is why two quotes for the same city pair can look very different.
One operator may quote only the flight. Another may quote the full bedside transfer. The second number often looks higher at first and saves money, delay, and confusion later.
The charges families miss most often
These are the items I tell families and case managers to ask about right away:
- Ground ambulance on both ends. This is part of the transport, not an afterthought.
- Bedside pickup and bedside delivery. Airport-to-airport pricing leaves major gaps.
- Medical oxygen and disposable supplies. These can be bundled or billed separately.
- Specialty staffing. Higher-acuity patients may require a larger or more specialized team.
- Waiting time and schedule changes. Delayed discharge, late acceptance, or aircraft repositioning can affect the total.
- International handling. Customs, permits, and document review add work and cost.
Ask for one number for the entire trip. If the provider cannot tell you who is handling the patient at the sending hospital, on the aircraft, and at the receiving hospital, the quote is incomplete.
Dedicated medevac jet vs. commercial medical escort
At this point, families can save a great deal of money, or make an expensive mistake.
A dedicated medevac jet makes sense when the patient needs continuous monitoring, oxygen beyond standard airline limits, a stretcher setup, urgent timing, or direct airport access close to the hospital. It costs more, but it reduces handoffs and gives the medical team control.
A commercial medical escort is often the smarter buy for stable patients who can sit upright, tolerate a normal airline cabin, and do not need intensive onboard equipment. The flight cost is lower, but you still need to price the escort, airline arrangements, and both ground legs. For many non-critical repatriations, that option is the right call.
If you want a plain-language checklist of the intake questions that shape the quote, read this air ambulance cost guide explaining what impacts pricing and what you’ll be asked when you call.
Teams that have handled these transports since 1978 usually catch missing cost items before a family wires money. That experience matters because the goal is not a low opening quote. The goal is an honest all-in plan.
Key Factors That Change Your Final Price
Two patients can travel roughly the same route and receive very different quotes. That’s normal. The cost of medevac flight changes because the mission changes.
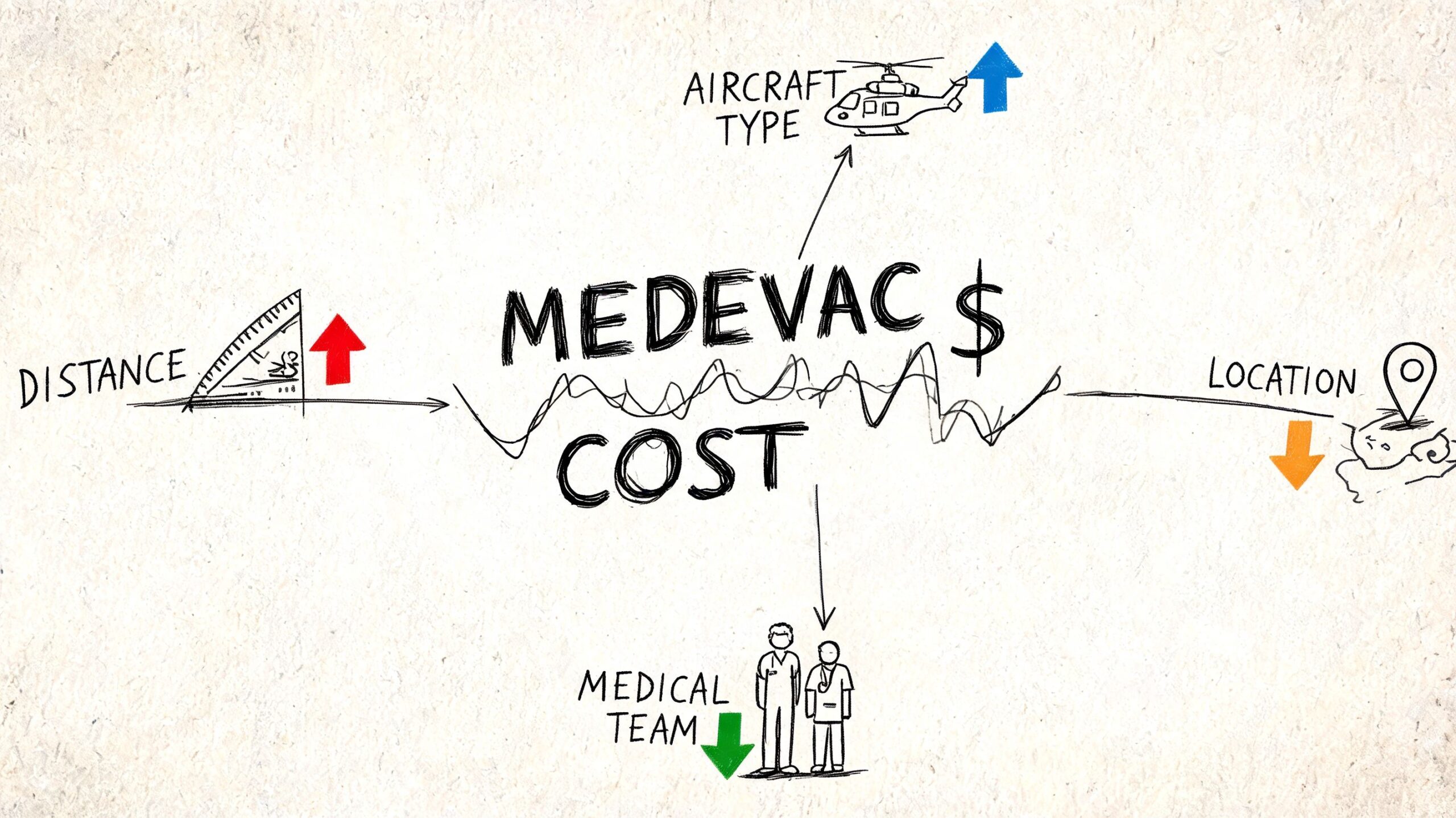
Patient condition changes everything
The fastest way a quote goes up is clinical complexity.
A patient who needs standard monitoring is easier to move than a patient who needs intensive respiratory support, specialty equipment, bariatric accommodation, or a higher level of onboard care. The aircraft may be similar, but the staffing plan and medical setup aren’t.
Distance matters, but aircraft choice matters more
Longer flights cost more, but the wrong aircraft can cost you in other ways. For transfers over longer distances, fixed-wing transport often makes more operational sense than rotary options. If you need a plain-language comparison, this fixed-wing vs rotary-wing explanation helps families understand why the aircraft type changes both logistics and pricing.
What I tell families is simple. Don’t ask which option is cheaper in theory. Ask which option reduces handoffs, delay risk, and patient stress for this transfer.
The factors that push quotes up
Here are the big ones:
- Urgency: Same-day or highly compressed scheduling creates more operational pressure.
- Positioning: If the aircraft and crew aren’t already nearby, the mission may involve additional movement before patient pickup.
- Ground complexity: Urban congestion, rural airport access, and hospital coordination can all complicate timing.
- International routing: Border clearance and permit issues create more administrative work.
- Patient size and mobility: Bariatric setup or special loading requirements increase complexity.
My blunt advice on quote shopping
Don’t shop medevac quotes the way you shop hotel rates.
One provider may show a lower number but exclude one or both ground legs. Another may assume a lower level of care than the sending physician expects. Another may price the flight cleanly but leave the family to coordinate hospital acceptance and records.
Lower isn’t cheaper if the patient misses the transfer window, needs rebooking, or ends up generating separate bills from three vendors.
If you’re comparing providers, compare the scope first and the number second.
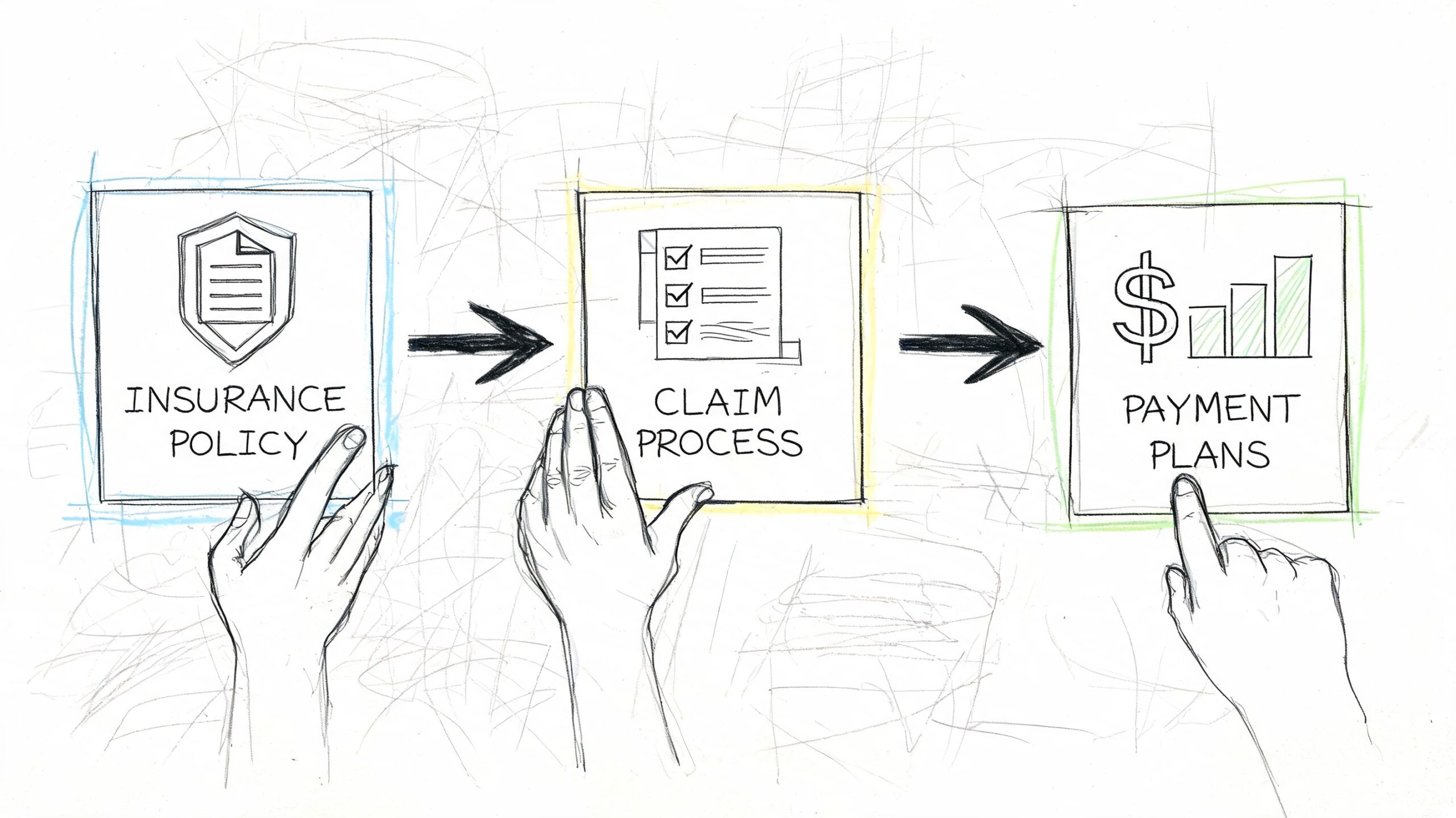
Navigating Insurance and Payment Options
The payment problem usually starts after the clinical decision is already made. A hospital says the patient should move. The family hears a quote. Then someone assumes insurance will sort out the rest.
That assumption gets expensive fast.
What insurance usually cares about
Insurance carriers pay attention to medical necessity, physician documentation, and whether the transport level matches the patient’s condition. Emergency flights usually have a cleaner path than scheduled transfers, but planned moves can still qualify if the chart clearly shows why the patient cannot travel by a lower-acuity method and why the receiving facility is appropriate.
For families dealing with Medicare questions, this guide on whether Medicare covers air ambulance is a useful starting point because it explains coverage around medical necessity and transport criteria.
Approval alone is not enough. You also need to know what the approval covers.
A family may hear that the flight is authorized and assume the bill is handled. Then the ground ambulance to the departure airport is billed separately. The arrival-side ambulance is separate too. In some cases, a medical escort, oxygen, waiting time, or extra clinical staffing is carved out from the main invoice. If you want the accurate number, ask for the all-in transport scope, not just the aircraft charge.
Out-of-network and split billing problems
The hardest bills to fix are the ones nobody asked about up front.
Even when a flight is covered in principle, the provider may be out of network, or only part of the trip may fall under the approval. That leaves the patient or family arguing about balance bills, uncovered legs, or services that were never clearly listed before departure.
Ground transport often creates the second surprise bill. If the transfer starts after a crash or roadside event, that payment issue can overlap with auto insurance or injury claims. In that situation, families often benefit from a separate legal overview like this guide for Florida ambulance accident payments, which explains how ambulance billing can interact with auto and injury claims.
Dedicated jet versus commercial medical escort
Families and case managers should make this decision with a simple filter. Start with patient tolerance, then confirm total cost.
According to Emergency Assistance Plus on air ambulance cost comparisons, commercial stretcher flights with a flight nurse can cost $25,000 to $30,000, often because the trip requires extra seat purchases, while dedicated air ambulances can range from $12,000 to $80,000.
That pricing range surprises people for a reason. Commercial medical escort service can look cheaper until you add airline seating blocks, airport handling, longer transfer times, overnight risk, and separate ground legs. A dedicated medevac jet can look higher at first glance, but sometimes it produces the cleaner all-in plan, especially when the patient needs close monitoring or cannot tolerate delays.
Choose a commercial medical escort if the patient is medically stable, can handle airline timing, and does not need ICU-style equipment or strict infection control. Choose a dedicated medevac jet if the patient is fragile, elderly, bariatric, post-surgical, or moving under tight hospital direction where fewer handoffs matter.
That is the true comparison.
Med Jets by Air Trek is one example of a provider that handles both dedicated medical flights and medical escorts, with hospital-to-hospital coordination and documentation support since 1978. That kind of experience matters because the transport itself is only part of the job. Records, acceptance timing, bedside coordination, and billing clarity decide whether the move stays on track.
A short visual can help if you're discussing the process with family members or administrators:
Clear payment advice
If you are paying privately, waiting on reimbursement, or covering a gap that insurance will not confirm in time, do these three things first:
- Get the full quote in writing. Ask whether it includes bedside pickup, both ground ambulance legs, clinical crew, oxygen, airport fees, permits, and after-hours coordination.
- Ask who sends separate invoices. Ground ambulance, receiving facility charges, and some clinical add-ons may not appear on the flight bill.
- Build the file before wheels up. Get the sending physician’s note, case management records, and medical-necessity explanation together before transport, not after the claim is denied.
My advice is simple. Do not ask only, “Will insurance pay?” Ask, “What exactly is covered, who bills the rest, and what does the patient owe if this claim goes sideways?” That is how you avoid the worst surprises.
Real-World Scenarios and Case Studies
Individuals don’t need another abstract explanation. They need to know what this looks like when a real family or hospital has to decide.
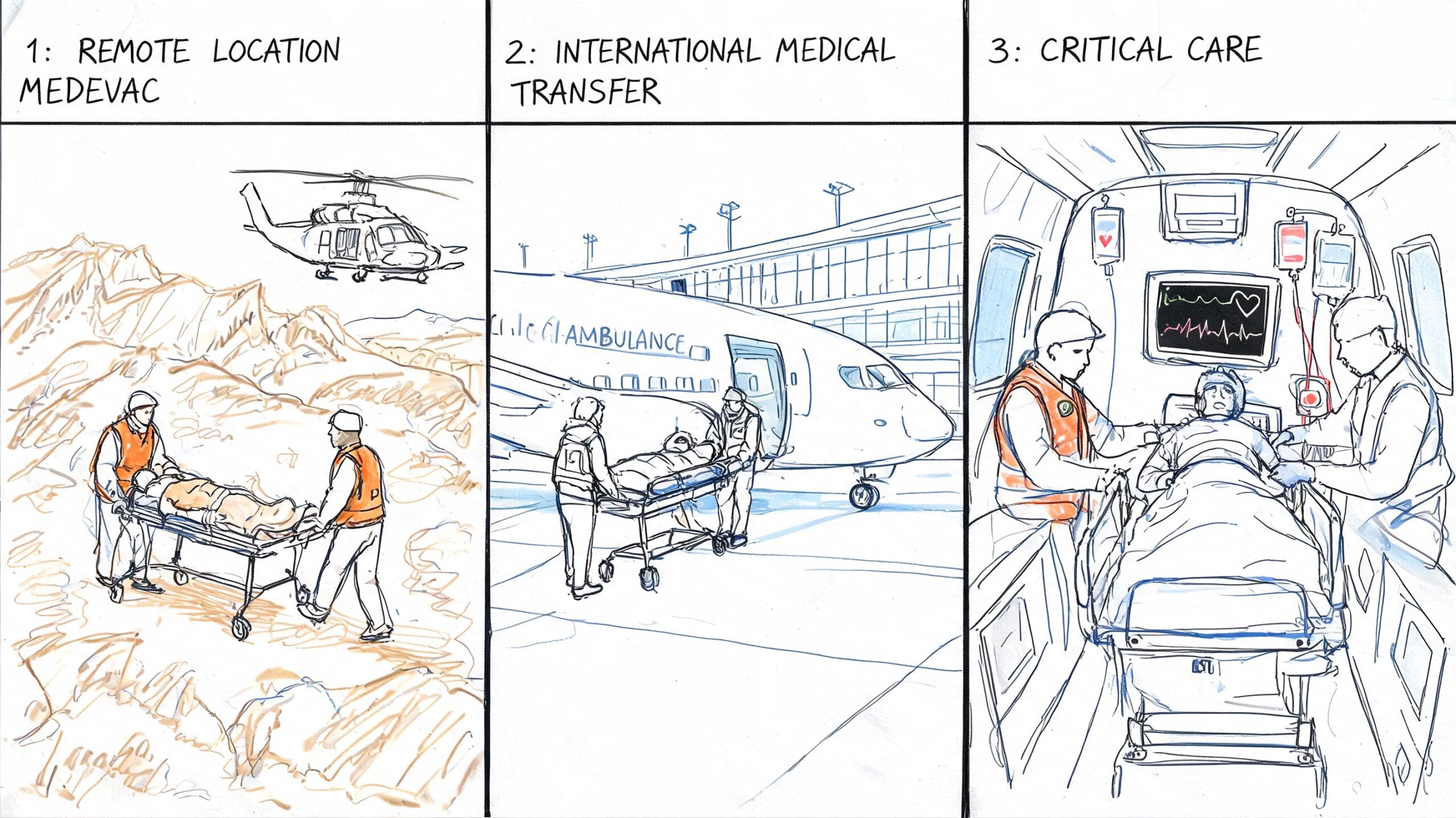
A senior transfer closer to family
An older parent fractures a hip while in Florida. Surgery is done locally, but the family wants recovery near adult children in New York. The patient is stable, but not stable enough for ordinary commercial travel.
This is usually where families start with the wrong question. They ask, “Can’t we just book a first-class ticket?” Often, the better question is whether the patient can tolerate airport handling, sitting upright, pain during transfers, and delays. If the answer is no, the dedicated medevac quote may look higher at first but make more sense clinically and operationally.
A bariatric ICU move between hospitals
A hospital case manager needs to transfer a bariatric patient from one ICU facility to another with tighter specialty support. This is not a routine stretcher transfer. Equipment, loading, and onboard setup all matter.
The mistake here is choosing a provider before confirming the aircraft configuration and patient handling plan. A cheap quote that doesn’t account for bariatric requirements isn’t a good quote. It’s a transfer risk.
Ask one direct question: “Have you moved this type of patient under this kind of clinical requirement before?”
An international repatriation after sudden illness
A couple is in the Caribbean when one partner becomes seriously ill. The local hospital stabilizes the patient, but the family wants transfer back to the United States for ongoing treatment.
People often underestimate the all-in problem. They focus on the long flight but forget the airport ambulance legs, border paperwork, receiving-hospital acceptance, and the fact that international transport has less room for improvisation. A dedicated fixed-wing jet is often the cleanest option when the patient needs monitored, uninterrupted movement.
What these stories have in common
Different patients. Different distances. Same lesson.
The right transport choice depends on four things:
- Clinical tolerance: Can the patient handle commercial travel conditions?
- Transfer complexity: How many handoffs are involved?
- Timing pressure: Is there room for airline schedules and delays?
- Financial structure: Are you comparing one coordinated service against multiple fragmented bills?
When families or case managers answer those four questions openly, the best option usually becomes obvious.
Frequently Asked Questions About Medevac Costs
Why has the cost of medevac flight risen so much
Because you are not paying for fuel and flight time alone.
You are paying for a medically configured aircraft, trained flight clinicians, maintenance, scheduling, insurance, dispatch, permits when needed, and a team that can move a patient safely with very little margin for error. Air medical transport has gotten more expensive for the same reason hospital care has. The staffing, equipment, and compliance costs are real, and they exist before the aircraft ever leaves the ground.
Does the quote usually include ground ambulance
Sometimes. Often it does not.
Ask one direct question: “Is this quote bed-to-bed, including both ground ambulance legs?” If the answer is unclear, expect extra charges. Families get into trouble when they compare a flight-only quote against a coordinated transport quote that includes bedside pickup, airport transfers, and delivery to the receiving facility.
How do I know whether we need a dedicated medevac jet or a commercial medical escort
Use a simple decision filter.
Choose a dedicated medevac jet if the patient needs continuous monitoring, oxygen or suction beyond standard airline limits, a stretcher, infection control precautions, or tight timing with minimal handoffs. Choose a commercial medical escort if the patient is stable enough to sit upright, can tolerate airline delays and terminal transfers, and does not need an ICU-style setup in the air.
The cheaper option is not the right option if it adds transfer risk, missed connections, or extra ground handling. A lower flight quote can become the more expensive choice once delays, added vendors, and clinical complications show up.
Can a family member travel with the patient
Often yes, but clinical care comes first.
On a dedicated aircraft, space depends on the patient setup, crew size, and weight limits. On a commercial medical escort trip, it depends on airline rules, seat availability, and whether the escort needs full access to the patient during the trip. Ask early, not the day of transport.
Can the patient bring luggage or a pet
Usually some luggage is possible, but only within weight and space limits.
Pets are a separate question and should never be assumed. Dedicated aircraft usually offer more flexibility than airline-based transport, but approval still depends on safety, aircraft configuration, routing, and any import or health rules if the trip crosses borders.
How quickly can a flight be arranged
Fast, if the paperwork and medical decision-making are in order.
The delays usually come from incomplete records, no accepting physician, late insurance questions, or slow ground coordination. Since 1978, we have seen the same pattern again and again. The families and case managers who move quickest are the ones who send records early, confirm the receiving facility, and ask for one coordinator to manage the full trip.
What documents will the transport team ask for
Have these ready:
- current medical records
- physician notes and recent clinical updates
- medication list
- sending and receiving facility contact information
- accepting physician or unit details
- passport or travel documents for international trips
- insurance information, if applicable
- responsible party contact for payment and consent
Missing documents slow down quotes and can delay departure.
If we can’t afford the full amount upfront, should we still call
Yes.
Call first and get the transport plan defined correctly. Once the clinical requirements, aircraft type, routing, and ground legs are clear, you can discuss insurance, payment timing, and what can be arranged. Guessing before that point wastes time and often leads families toward the wrong transport method.
What hidden fees should we ask about
Ask about:
- ground ambulance on one or both ends
- waiting time for ground crews
- after-hours or weekend coordination
- airport handling fees
- international permits or customs support
- oxygen, ventilator, or specialty equipment charges
- extra clinical staff if the patient needs a higher level of care
- costs tied to route changes or weather-related repositioning
If a quote looks unusually low, one of these items is often missing.
What’s the single best question to ask when comparing options
Ask this: “What is included in the all-in quote, from bedside pickup to bedside arrival?”
That question cuts through marketing fast. It tells you whether you are comparing one coordinated medical transport plan or a partial quote that leaves your family to sort out ambulances, airport transfers, and extra invoices later.
If you’re comparing options for the cost of medevac flight, ask for a written all-in quote, confirm whether the transport is bed-to-bed, and choose based on the patient’s clinical tolerance for delays, handoffs, and airline conditions. In this field, the safest plan and the clearest financial plan are usually the same plan.