
The phone usually comes at the worst moment. A nurse says your father needs a higher level of care. A rural hospital can stabilize him, but not keep him. A case manager asks whether air transport is being arranged. Your mind jumps to the same questions most families ask. Is this only for trauma? Is it safe? Who decides? How fast can they move him? What will this cost?
That’s where michigan survival flight enters the picture for many Michigan families and hospital teams. It’s not just a helicopter in the sky. It’s a clinical transport system built for patients who need ICU-level support while moving from one place of care to another.
If you’re trying to understand what happens next, it helps to think in layers. First, what Survival Flight is. Then, what its crews can do in the air. Then, how the transfer gets approved, launched, and completed. Finally, when a helicopter-based emergency system is the right answer, and when a dedicated fixed-wing medical flight is the better fit.
That Urgent Call Understanding Your Airmobile Lifeline
A common Michigan scenario goes like this. Your loved one is in a smaller hospital after a stroke, severe infection, trauma, or sudden heart problem. The local team is doing what they can, but they need to get the patient to a tertiary care center quickly. Ground transport may take too long, or the patient may need a level of monitoring and intervention that’s hard to maintain on the road.
In that moment, families often hear a name before they understand the system. Survival Flight.
Michigan Survival Flight serves as an airmobile link between hospitals, scene locations, and advanced care centers. For the family, it can feel abrupt. For the clinical team, it’s part of a larger chain of survival where minutes, equipment, and crew skill all matter. If you’ve ever heard clinicians talk about the importance of early definitive care, the broader concept behind the medical golden hour in emergency transport helps explain why these decisions happen so quickly.
What families usually worry about first
The initial focus isn’t on the aircraft. Instead, they ask:
- Is my loved one stable enough to fly
- Will the flight crew be able to manage emergencies in the air
- Where will the patient go
- Can I ride along
- How is this being arranged so fast
Those are reasonable questions. They come from the same fear. You’re being asked to trust a process you can’t see.
Practical rule: Air medical transport is usually chosen because the sending team believes the patient will be safer reaching the right level of care sooner, with advanced support available during the trip.
That doesn’t mean every patient needs a helicopter. It means the transport choice is tied to urgency, geography, weather, and the medical resources required in transit.
What Is Michigan Survival Flight
Michigan Survival Flight is the University of Michigan’s hospital-based air ambulance program. The simplest way to understand it is this. It functions like an emergency room and intensive care transport team that flies, rather than a basic ride from one facility to another.

Its job is centered on patients who need high-acuity movement between locations. That can include scene responses, transfers from smaller hospitals, pediatric and neonatal missions, and specialty transport linked to advanced services at Michigan Medicine.
Why the program matters in Michigan
For families, the biggest point is trust. This isn’t a new or experimental service. According to the University of Michigan, Survival Flight is recognized as the world’s first air ambulance system and has safely transported more than 57,000 patients since its inception, while logging about 7.9 million flight miles over 32 years by 2018, which the health system compares to 34 trips from Earth to the Moon in its Survival Flight patient transport history.
That history matters because air medicine is not just flying. It’s dispatch coordination, weather judgment, aircraft maintenance, crew training, patient packaging, medication management, and handoff discipline. A mature program tends to build all of those pieces into one system.
What Survival Flight is not
It helps to separate Survival Flight from other forms of medical aviation.
It is not the same as a non-medical charter flight. It is not just a hospital shuttle. And it is not always the same kind of service a family might arrange later for a planned, long-distance return home.
Here’s a simple distinction:
| Service type | Primary purpose |
|---|---|
| Hospital-based air ambulance | Emergency and critical interfacility or scene transport |
| Dedicated fixed-wing medical flight | Longer-distance or planned medical relocation with expanded cabin options |
| Medical escort on a commercial flight | Appropriate only for selected stable patients |
Michigan Survival Flight is best understood as a critical care response system first, and a transport option second.
That framing clears up a lot of confusion. The aircraft matter, but the primary asset is the combined medical and operational capability.
A Look Inside Survival Flight's Clinical Capabilities
A family often sees the aircraft first. The sending and receiving hospitals are focused on something else. They need to know whether the patient can keep getting ICU-level care during the minutes or hours between beds.
That is the primary question behind Survival Flight’s clinical capability.
According to Metro Aviation’s Survival Flight fleet summary, the program uses three Eurocopter EC-155B1 helicopters and a Bombardier Learjet 75. Those aircraft matter, but only as treatment spaces. The helicopter is built for urgent regional access. The jet extends range when the transfer is longer and time still matters.
A simple way to picture it is this. The aircraft is the room. The crew, equipment, medications, and monitoring are what make that room function like a transport ICU.
What care can continue in the air
Patients sent by air are usually not stable enough for a basic ride. They may need a ventilator, continuous medication infusions, close neurologic checks, or advanced monitoring that cannot pause just because the patient left the hospital.
Program materials describe capabilities such as:
- Advanced ventilatory support for patients who need controlled breathing throughout transport
- Neonatal transport equipment including isolettes for fragile newborns
- Invasive monitoring to track pressure changes and other critical trends in real time
- Specialty configurations for pediatric and other high-acuity patients
- Equipment consistency across aircraft so care changes as little as possible if the mission uses the jet instead of a helicopter
That matters because transport is not passive observation. It is active treatment in a smaller, louder, more physically demanding environment.
If a family is hearing terms like troponin, ischemia, or cardiac rule-out while a transfer is being arranged, a plain-language reference such as the Troponin I Rapid Card can make one piece of the medical picture easier to understand.
Why crew experience matters as much as the aircraft
The aircraft carries the team. The team carries the patient safely through the unstable part of the move.
University of Michigan Health describes Survival Flight as staffed by specially trained nurses, paramedics, pilots, mechanics, and communication specialists in its Survival Flight patient transport history. For a hospital case manager, that staffing model means the patient is not merely accompanied. The patient is being managed by clinicians used to high-acuity transport decisions.
In practical terms, that includes recognizing when blood pressure support needs adjustment, when an airway is becoming harder to manage, or when a newborn or pediatric patient needs tightly controlled temperature and respiratory support.
Where a dedicated fixed-wing service may be the better fit
This is also where families and discharge planners can get confused. A hospital-based program like Survival Flight is built first for urgent critical transport. That does not mean it is always the best answer for every transfer.
A dedicated fixed-wing service such as Med Jets by Air Trek can be the better choice when the mission is planned rather than emergent, when the patient must go a long distance, or when the patient needs more cabin space, including some bariatric transports. In those cases, the medical question is not only, "Can the patient fly?" It is also, "Which aircraft and crew setup will let the patient travel with the fewest compromises?"
That distinction helps avoid a common mistake. People compare helicopter versus jet as if speed alone decides the issue. In reality, patient size, destination distance, weather, runway access, family goals, and the expected level of in-flight care all shape the right choice.
Why hospitals trust this kind of setup
Hospitals trust air medical programs when the clinical handoff stays intact from one bedside to the next. That trust comes from three things working together.
- The aircraft matches the mission
- The onboard equipment supports active critical care
- The crew can assess and intervene during transport, not just observe
For families, the aircraft is the visible part. For clinicians, continuity of care is the point. The best transport option is the one that fits the patient’s condition, distance, and timing without forcing the care team to cut corners in the air.
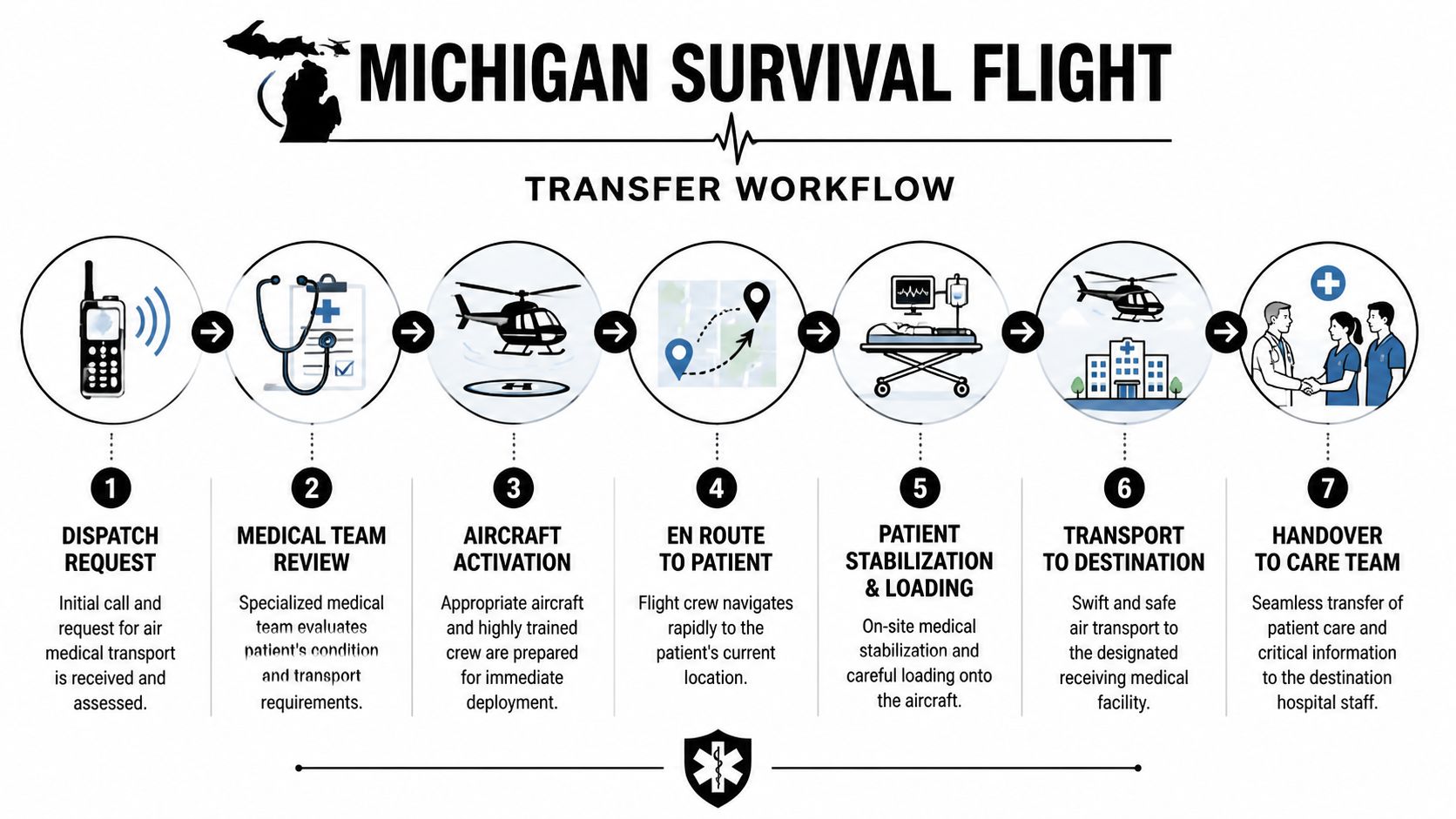
From Dispatch to Bedside The Transfer Workflow
At 2 a.m., a community hospital decides a patient cannot stay where they are. The family hears, “We’re calling flight.” From that point, the process can feel fast and hard to follow. Under the surface, though, it works like a relay. One team gathers the medical facts, another matches the patient to the right aircraft, and the receiving hospital prepares for arrival.
That structure matters because air transport is not only about getting off the ground. It is about getting the patient from one bedside to the next without losing time, information, or treatment continuity.
How the request usually starts
The call usually begins at the sending hospital. A physician, transfer center, emergency department, or case manager identifies a gap in local care and requests transport to a higher-level facility.
Dispatch then works through two tracks at once. The first is clinical. How sick is the patient, and what support will they need during the trip? The second is operational. Where is the patient going, what aircraft can safely make that trip, and what weather or landing limits apply?
For a worried family, this can look like delay. In practice, it is sorting. The goal is to avoid sending the wrong aircraft or launching a crew without the setup the patient needs.
What happens before wheels up
Before departure, the transport team reviews the patient’s condition, current treatments, destination, and loading requirements. That review is one of the points where the helicopter versus jet question becomes practical, not theoretical.
A rotor-wing program such as Survival Flight is often the right fit for urgent regional moves. A planned transfer may point in a different direction. Long-distance travel, airport-to-airport routing, extra cabin room, or bariatric needs can make a fixed-wing aircraft the safer and more workable choice. This fixed-wing vs rotary-wing air ambulance comparison gives a useful side-by-side view of how those decisions get made.
The workflow usually follows this order:
- A transport request is placed by the sending hospital or emergency system.
- Clinical screening confirms the mission and the receiving destination.
- Dispatch assigns the aircraft and crew based on urgency, range, weather, and patient needs.
- The sending team prepares the patient with records, medications, infusions, and imaging or lab information.
- The flight crew arrives and reassesses the patient before loading.
- Transport begins with monitoring and treatment continuing in the aircraft.
- The receiving team accepts a bedside handoff with the transport crew reporting what changed in transit.
A short explainer can also help if you need to brief family members or staff:
Why communication can make or break the transfer
The aircraft is only one part of the handoff chain. The other part is communication. Orders, medication times, vent settings, code status, and receiving-bed details all have to stay aligned while several teams are working quickly.
That is why hospitals depend on structured transfer-center workflows and secure updates. Many health systems support that coordination with the kinds of tools reviewed in top healthcare communication platforms, especially when case management, bedside staff, and receiving units all need the same information at the same time.
For families, the simplest way to understand responsibility is this. Once the patient is accepted and loaded, the flight crew becomes the active medical team in transit. When the patient reaches the receiving unit, care shifts again at the bedside through a direct report, questions, and confirmation of the current treatment plan.
A good transfer feels fast. A safe transfer is organized.
Helicopter vs Jet Which Air Ambulance Do You Need
Many people often get confused here. They assume “air ambulance” means one thing. It doesn’t. A helicopter and a fixed-wing medical jet solve different transport problems.
The most useful question isn’t “Which is better?” It’s “Which fits this patient, this distance, and this timeline?”
The quick comparison
| Factor | Helicopter (e.g., Survival Flight) | Fixed-Wing Jet (e.g., Med Jets by Air Trek) |
|---|---|---|
| Best use | Immediate regional response, scene work, urgent interfacility transfer | Longer-distance transfer, state-to-state movement, planned medical relocation |
| Access | Can reach hospital helipads and some direct scenes | Requires airport operations and ground coordination on both ends |
| Distance fit | Better for shorter and medium missions | Better for long-haul transport |
| Cabin space | More limited | More room for equipment, patient positioning, and support needs |
| Bariatric flexibility | Often limited by cabin and loading constraints | Better suited when size, bed configuration, or specialized loading matters |
| Family accompaniment | Often restricted | More likely to work in planned settings, depending on operator and mission |
| Mission style | Urgent and time-compressed | Planned or semi-urgent, especially across larger regions |
When the helicopter is the right answer
A helicopter shines when the patient needs to move now, the sending location is relatively close, and direct access saves time. That’s why rotor-wing transport is closely associated with trauma, strokes, cardiac emergencies, and high-acuity hospital transfers within a practical regional radius.
It’s also useful when hospital helipad access avoids the delay of ambulance-to-airport-to-ambulance transitions.
When a jet becomes the better tool
A fixed-wing medical jet is often the better choice when the patient is going a long distance, when the transfer is planned rather than scene-emergent, or when the patient’s body size and equipment needs make helicopter space too restrictive.
One of the clearest examples is bariatric transport. According to the program profile cited by Simple Flying, Survival Flight’s Learjet 75 can support bariatric configurations for patients up to 450 kg, and the article notes that 42% of U.S. adults exceed 300 lbs, making specialized transport design an important issue in real-world medical movement, as outlined in this guide to Survival Flight’s Learjet and specialty capabilities.
That point matters because families often think, “If a helicopter can move a trauma patient, why not everyone?” The answer is geometry, loading, cabin access, fuel planning, and the need to keep the patient medically manageable throughout the trip.
Communication changes the outcome
The transport choice also depends on how well hospitals, dispatchers, and families share information. If the sending team misses key facts such as weight, oxygen requirement, isolation status, or whether a parent needs to accompany a child, the first aircraft plan may not be the right one.
For case managers trying to tighten those handoffs, a practical review of top healthcare communication platforms can help teams think more clearly about how transport-related information gets shared across departments.
If you’re weighing helicopter versus plane for a real transfer, this plain-language overview of fixed-wing vs rotary-wing air ambulance differences is also useful.
The right aircraft is the one that matches the patient’s medical needs, body size, trip length, and time pressure all at once.
Navigating Insurance Consent and Financial Questions
This is usually the hardest conversation because families want a straight number, and many programs don’t publish one clearly for every mission type. That includes michigan survival flight.
The important thing to know first is that cost and clinical need are separate questions. A physician may determine that the patient needs air medical transport before anyone can give the family a final estimate of insurance coverage or out-of-pocket responsibility.
What’s known and what isn’t
The University of Michigan materials leave a meaningful information gap around transport pricing, insurance acceptance details, and balance billing specifics. One summary of that gap notes that this stands in contrast to a national average of $30,000 to $50,000 for air medical transports, while also emphasizing that Survival Flight-specific pricing details are not laid out in the public-facing materials reviewed in this overview of the cost information gap.
That means families should expect to ask direct questions rather than assume the financial side is fully explained at the moment of transfer.
Questions to ask before or after transport
If the patient is stable enough for financial review, or if you’re a case manager handling a planned transfer, ask:
- Who is billing for the flight. Hospital program, aviation operator, or another entity.
- Was prior authorization attempted if the situation allowed it.
- Is the transport considered medically necessary under the patient’s plan language.
- What part of the trip is covered. Air segment only, or also ground ambulance on either end.
- Will there be separate professional or facility charges tied to the move.
- Who can help with documentation if the insurer asks for medical records, physician notes, or transfer rationale.
Consent and paperwork basics
Consent usually covers the transport itself, medical treatment in transit, and release of information needed for coordination and billing. If the patient can’t sign, the hospital works through the appropriate decision-maker under its policies.
Families also ask about Medicare. Coverage depends on medical necessity and plan details, so it helps to review a plain-language resource on whether Medicare covers air ambulance services.
Ask for the name and direct number of the person handling transport authorization or billing follow-up. One informed contact can reduce a lot of confusion later.
When time is short, the transfer may go forward before all insurance answers are finalized. That’s stressful, but it’s common in urgent care. The key is getting the clinical documentation organized early.
Michigan Survival Flight FAQ Your Questions Answered
Can a family member ride with the patient
Sometimes, but not always. Space, patient condition, aircraft type, weight limits, and safety policy all affect that decision. On urgent helicopter missions, the answer is often no. On some planned fixed-wing transports, accompaniment may be more workable.
What can the patient bring
Usually only essential items travel with the patient. Think identification, medication list, critical paperwork, and necessary medical devices. Larger personal belongings usually go separately with family or the sending facility.
What if weather becomes a problem
Air medical crews don’t launch just because a transfer is urgent. They also have to decide whether it’s safe. If weather prevents a flight, the team may delay, choose a different aircraft type, or move the patient by ground if that’s the safest workable option.
Are pediatric and neonatal patients handled differently
Yes. These patients often need highly specific equipment and careful temperature, airway, and monitoring support. That’s why specialized transport capability matters so much for newborns and children.
How are bariatric patients handled
Bariatric transport requires more than a wider stretcher. Teams have to think about loading, cabin access, positioning, pressure protection, and aircraft configuration. That’s one of the clearest situations where a fixed-wing service may be the better fit.
Who usually arranges the transfer
In urgent cases, the sending physician, transfer center, or hospital team usually starts the process. Families are part of communication and consent, but they often are not the people making the first operational call.
Is michigan survival flight the right option for every air transfer
No. It’s a strong fit for many urgent and high-acuity missions. But if the trip is long-distance, planned, bariatric, or needs a different cabin setup, a dedicated fixed-wing provider may be more appropriate.
If you’re comparing options for a long-distance, planned, or bariatric medical flight, Med Jets by Air Trek can help you review the transport fit, explain logistics clearly, and coordinate a safe bedside-to-bedside solution.