When a doctor says an ICU patient needs to move to another hospital, families usually hear two things at once. First, this is serious. Second, everything now feels urgent.
That combination is hard. People want a clear answer to a simple question: how do you transfer an ICU patient to another hospital safely, without losing time, information, or control? The good news is that this isn't an improvised process. Good transfers follow a disciplined sequence. The patient is stabilized, the receiving team is confirmed, transport is matched to the clinical situation, paperwork is handled, and the handoff is closed carefully at the bedside.
Families and case managers don't need to run the medicine. They do need to understand the checkpoints. That makes it easier to ask the right questions, catch delays early, and support the team without adding confusion.
The Moment a Hospital Transfer Becomes Necessary
The call often comes in the middle of everything else. A physician explains that the current hospital has done the immediate work, but the patient now needs another ICU, a higher level of specialty care, or a bed in a facility that can continue treatment without interruption. Families hear "transfer" and think danger. In practice, transfer is also a normal part of critical care operations.
That matters. During one pandemic period alone, 2,793 patients were transferred between ICUs across the UK, and research from a study on ICU transfer patterns and outcomes found that while some patients had a temporary physiological decline after transfer, there was no long-term mortality increase when transfers were managed properly.
So the first mental shift is this. A transfer is not automatically a sign that something has gone wrong. It often means the team is trying to put the patient in the right place for the next phase of care.
Why hospitals move ICU patients
The reasons are usually practical and clinical:
- Specialized treatment is needed: The receiving hospital may have a service the current hospital doesn't.
- Capacity has changed: The patient may need an ICU bed, equipment, or staffing that isn't available where they are now.
- Continuity matters: Some patients need to be moved to a center that can manage the full course of care, not just the emergency phase.
Families also want to know how fast this should happen. The honest answer is that speed matters, but unsafe speed is a mistake. The right transfer is coordinated, not rushed blindly.
Practical rule: The safest transfer is usually the one that leaves a little later, but leaves with the right team, the right equipment, and a confirmed receiving bed.
There is also a timing question people rarely ask clearly enough: "Is this transfer urgent because of the patient's condition, or because the current hospital's resources are limited?" Both are valid reasons, but they shape the plan differently. If you're trying to understand urgency in a crisis context, the idea of the medical golden hour helps frame why some moves need to be organized quickly while still protecting stability.
What families should ask immediately
In the first conversation, ask short, concrete questions:
- Why this hospital? Is it because of specialty care, ICU capacity, or both?
- Has the receiving physician accepted the patient?
- Is the patient stable enough to move now, or are you stabilizing first?
- What transport type are you considering?
- Who is coordinating communication with the family?
Those questions lower confusion fast. They also tell you whether the process is already structured, which is one of the strongest signs that the transfer is being handled well.
Confirming Medical Stability for the Journey
Before anyone talks about road miles, flight time, or signatures, the clinical team answers one question: can this patient tolerate movement? ICU patients don't travel well just because a vehicle is available. They travel well when the team has corrected the problems most likely to worsen in transit.
Expert guidance for critical care transport sets practical pre-transfer targets. A patient should generally have a pulse of 60 to 120 bpm, systolic blood pressure over 100 mmHg, and urine output above 0.5 ml/kg/hr, according to LITFL guidance on transferring the critically ill. The same guidance notes that hemodynamic instability can occur in 20 to 30% of transfers if not properly managed.
What "stable for transport" usually means
Families often hear that the patient is "stable" and assume that means "well." In ICU transport, it means something narrower. It means the team believes the patient's condition can be maintained during movement.
A practical bedside checklist often includes:
- Blood pressure is supported: Low pressure is corrected before departure, not chased after the ambulance or aircraft leaves.
- Heart rhythm is acceptable: Teams want a rhythm they can monitor and manage reliably in transit.
- Oxygenation is controlled: Ventilator settings, oxygen supply, and airway security are reviewed before wheels move.
- Lines and tubes are secured: IV access, arterial lines, feeding tubes, drains, and the endotracheal tube must be taped, checked, and protected from accidental dislodgment.
- Enough supplies are packed: Oxygen, medications, batteries, suction capability, and backup equipment must cover the trip with margin.
Questions that get useful answers
If you're a family member or case manager, ask these in plain language:
- What's the main thing you're stabilizing before transfer?
- Is the patient intubated, and if so, is the airway secure for transport?
- What medications must continue without interruption during the trip?
- Do you have backup oxygen and power if there is a delay?
- Who on the transport team can manage sudden deterioration?
That last question matters more than is often realized. The vehicle doesn't make a transfer safe. The team and equipment package do. If the patient requires advanced monitoring or ventilator support, the transport setup needs to mirror ICU capability as closely as possible. For readers comparing what travels with the patient, aeromedical supplies and transport equipment give a useful picture of what specialized teams prepare before departure.
"Full patients travel better."
Critical care teams use that phrase for a reason. If blood pressure is borderline, oxygen reserves are thin, or sedation is inconsistent, the road or flight tends to expose the weakness fast. Waiting long enough to stabilize is often what prevents a mid-transport crisis.
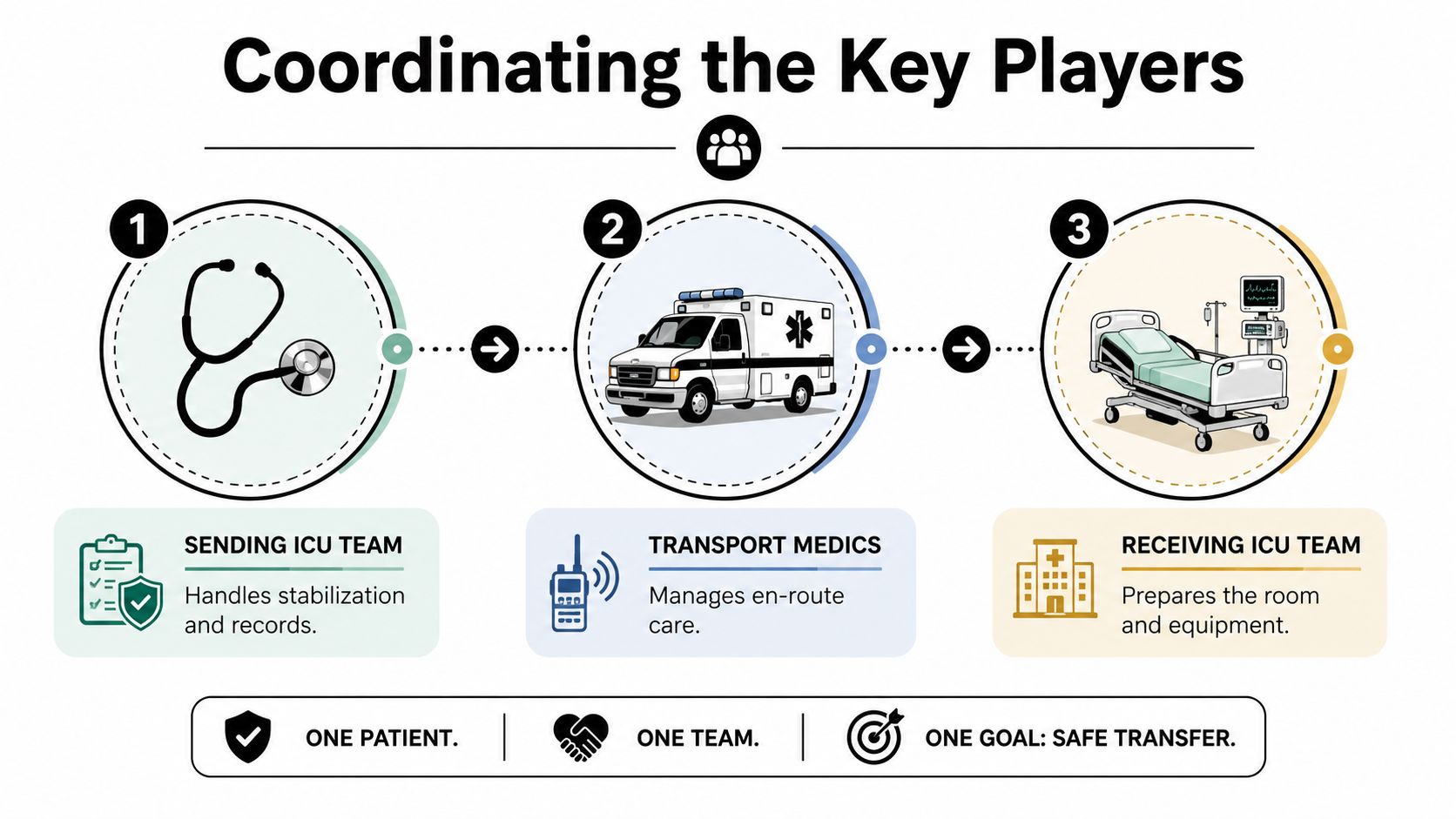
Coordinating the Key Players for a Seamless Handoff
A good ICU transfer doesn't depend on one heroic clinician. It depends on several people doing ordinary things with precision. When transfers go poorly, the failure is often not dramatic. It is usually a missing medication list, an unclear receiving plan, an undocumented ventilator setting, or a family that was told one thing while the transport team was told another.
Evidence-based transfer protocols emphasize structured communication. Standardized handoffs such as SBAR can reduce transfer-related errors by up to 50%, and a multidisciplinary process with checklists and designated coordinators can cut transfer delays by as much as 40%, according to evidence-based strategies for improving patient transfers.
Who does what
The handoff is cleaner when each role is explicit.
- Sending ICU physician: Confirms the need for transfer, stabilizes the patient, summarizes current condition, and speaks directly with the receiving physician.
- Receiving ICU physician: Accepts the patient, confirms bed availability, and prepares the unit for arrival.
- Case manager or discharge planner: Coordinates authorizations, records, consent flow, and family communication.
- Transport team: Reviews clinical needs, checks equipment, and manages the patient between facilities.
- Family or legal decision-maker: Confirms consent, shares key history when needed, and keeps contact information current.
Why SBAR works
SBAR stands for Situation, Background, Assessment, Recommendation. It sounds simple because it is. That's its strength.
A strong ICU transfer handoff usually covers:
| SBAR element | What must be clear |
|---|---|
| Situation | Why the patient is being transferred right now |
| Background | Diagnosis, recent events, procedures, medications, allergies |
| Assessment | Current vitals, airway status, support devices, active concerns |
| Recommendation | What the receiving team should be ready to do on arrival |
A short visual can help families understand the chain of custody during a transfer.
What actually prevents mistakes
The safest teams don't rely on memory. They rely on disciplined redundancy.
The transport team should know the exact ICU destination, not just the hospital name.
That means room, unit type, accepting service, key contact numbers, and whether radiology, blood products, or isolation precautions are expected on arrival. Families can help by making sure one person is designated to receive updates. When five relatives call five departments separately, signal turns into noise.
Navigating Transport Options and Financial Paperwork
Once the patient is medically ready and the receiving hospital has accepted the case, the decision usually narrows to ground or air. Families often feel pressure to choose quickly at this stage. The better approach is to compare the options against the patient's condition, distance, weather, road realities, and time sensitivity.
For some ICU transfers, ground is entirely appropriate. For others, especially long-distance moves or situations where specialty care is far away, fixed-wing air transport becomes the practical option.
Comparing the transport modes
| Factor | Ground Ambulance | Air Ambulance (Fixed-Wing Jet) |
|---|---|---|
| Best use case | Regional transfer when drive time is reasonable | Long-distance transfer or when time and range matter |
| Environment | More stops, traffic effects, road vibration | Faster over long distances, but requires airport coordination |
| Access to patient | Usually straightforward in the vehicle | Must be planned around cabin layout and equipment placement |
| Weather impact | Road and traffic delays | Weather and airport operations can affect timing |
| ICU capability | Depends on crew level and vehicle setup | Often chosen when advanced in-transit support is needed |
The right question isn't "Which is better?" It's "Which option preserves the patient's care best from bed to bed?"
For families evaluating specialized flight coordination, emergency medical transport services can help illustrate how fixed-wing transfers are organized alongside ground segments at both ends.
The paperwork people underestimate
The transport choice is only half the job. The administrative side can delay care if nobody owns it clearly. Common documents and approvals include:
- Physician transfer orders
- Receiving hospital acceptance
- Consent for transport
- Clinical records and medication list
- Imaging and reports
- Insurance authorization or case review
- Financial responsibility forms
If the patient lacks decision-making capacity, confirm who has legal authority to sign. If there is a healthcare proxy or power of attorney, have that document available early.
The cost question families need to ask directly
Many hospitals explain the clinical need for transfer well. Fewer explain the billing risk with the same clarity. That's a problem, especially in air transport.
According to information summarized in the RWJBarnabas transfer center context, air ambulance flights can average $30,000 to $50,000, and nearly 80% of cases historically involved out-of-network providers, which led to surprise bills. The same source notes that only 25% of providers fully comply with No Surprises Act regulations. Those numbers are exactly why families should ask for billing details before launch when time allows.
Ask these questions plainly:
- Is the transport provider in network for this plan?
- Who is obtaining prior authorization, if required?
- What happens if insurance denies part of the claim?
- Will I receive a written estimate or transparent quote?
- Who is my single point of contact for billing questions?
One practical option in this space is Med Jets by Air Trek, which coordinates hospital-to-hospital air transfers, insurance navigation, and related ground segments as part of the transport process. That kind of end-to-end coordination doesn't remove every billing issue, but it can reduce the number of separate conversations families must manage during a crisis.
Billing checkpoint: If nobody can tell you who is handling authorization, assume authorization is not truly being handled yet.
The Human Element Preparing Patient and Family for the Journey
The hours before departure are clinical, but they are also personal. Families are trying to absorb medical language, decide who rides where, notify relatives, pack chargers, locate insurance cards, and answer a question no one likes asking out loud: "Will they be alone?"
That question matters because transfer stress isn't only emotional. It affects communication, decision-making, and sometimes the patient's comfort during a vulnerable stretch of care.

What families can expect before departure
Near departure time, the room often gets busier, not calmer. The bedside team reconciles medications, secures lines, confirms monitors, prints or transmits records, and gives the transport crew a final update. Families sometimes misread that activity as chaos. Usually, it's the opposite. It means the checklist is active.
A family member can help by focusing on a few jobs:
- Keep one phone on and charged: The receiving hospital or transport team may call during movement.
- Choose one family communicator: One person updates the wider circle so the clinical team isn't fielding repeated calls.
- Pack only essentials: ID, insurance card, legal documents, phone charger, medication list, and comfort items if allowed.
- Ask about destination logistics: Which entrance, which ICU, and who can receive you on arrival.
Can a family member travel with the patient
Sometimes yes. Sometimes no. The deciding factors are usually aircraft configuration, infection control, patient acuity, and safety rules.
A 2025 Air Medical Journal survey indicated that 70% of air ambulance patients are at an ICU level, and a majority of families request to travel with them, according to the cited article on transport and family concerns. Standard protocols often overlook that request, even though reducing anxiety can matter to the transfer experience.
If accompaniment isn't possible, ask these instead:
- Where should the family meet the patient?
- Will someone call when the aircraft or ambulance departs?
- Will someone call again after arrival?
- Can the receiving ICU expect the family the same day?
A clear answer about family presence is better than a hopeful maybe. Families plan better when the rule is explicit.
What about pets, lodging, and support tasks
These details seem secondary until they become obstacles. A spouse may need help getting to the destination city. An elderly parent may need hotel coordination. A medically fragile traveler may need someone to manage non-medical logistics while the clinical team focuses on care.
For families who need help coordinating travel, lodging, and high-touch practical support around a hospital move, Approved Lux Personal Assistant is a useful example of the kind of concierge-style operational help that can reduce friction during a transfer.
Pet transport is more variable and must be asked about directly. Don't assume a hospital, ambulance service, or flight crew can accommodate it. If the patient relies heavily on that support animal or the family is traveling under strain, bring it up early so alternatives can be arranged if needed.
Ensuring a Safe Arrival and Continuity of Care
A transfer isn't finished when the wheels stop. It is finished when the receiving ICU has accepted responsibility, understood the current condition, and resumed treatment without gaps.
This final handoff should be deliberate. The transport crew gives a bedside report, the receiving clinicians verify key facts, monitors are switched over, medications are reconnected, and any immediate concerns are addressed before the transport team steps back.
What should happen on arrival
The cleanest arrivals usually follow a simple sequence:
Bedside report first
The transport clinician summarizes what happened during the trip, including any medication changes, airway issues, pressure changes, or events en route.Equipment transition second
Ventilator support, infusion pumps, and monitors are transferred to hospital equipment carefully, not all at once.Questions before departure
The receiving ICU team asks clarifying questions while the transport crew is still present and can answer them directly.
What families should listen for
You don't need to decode every medical term. Listen for continuity.
- Is the receiving team repeating back the diagnosis and current concerns correctly?
- Do they know what support the patient is on right now?
- Have they acknowledged any events that happened during transport?
- Do they tell you who the attending team is and how updates will work?
A calm arrival doesn't always look tidy. It often looks focused. Several people may speak briefly at once while tasks happen in sequence. What matters is whether there is a clear chain of responsibility from transport crew to ICU bedside.
Safe transfer means no dead space in care. Someone is always responsible for the patient, and everyone knows when that responsibility changes hands.
When families ask how to transfer ICU patient to another hospital safely, this is the answer in practice: stabilize first, communicate precisely, match the transport mode to the case, clear the paperwork early, and close the handoff carefully at the receiving bed.
Common Questions About ICU Patient Transfers
Below are the questions families and case managers ask most often when the basics are already in motion.
| Question | Answer |
|---|---|
| Can an ICU patient get worse during transfer? | Yes. That's why stabilization, monitoring, and an appropriately trained transport team matter so much. The goal is to make the transport environment function as close to ICU care as possible. |
| Who decides that a patient should be moved? | Usually the sending physician and the accepting physician make that decision together. The case manager then helps execute the plan, and the family is included in consent and logistics. |
| Does the receiving hospital have to accept the patient first? | Yes. A safe ICU transfer requires an accepting physician and a confirmed place for the patient to go. Moving before that is a setup for confusion and delay. |
| Is air ambulance always faster? | Over longer distances, often yes. But total transfer time also includes ground legs, airport coordination, weather, and bedside preparation. Faster in the air doesn't automatically mean faster from ICU to ICU. |
| Can a patient on a ventilator be transferred? | Yes, if the airway is secure, the patient is stabilized, and the transport team has the right ventilator, oxygen supply, monitoring, medication capability, and backup plans. |
| What if the patient is bariatric or needs special handling? | Say that early. Bariatric transfers require the right stretcher setup, loading plan, staffing, and vehicle or aircraft configuration. This should be confirmed before dispatch, not improvised at pickup. |
| What happens if there is an emergency during the trip? | The transport clinicians treat the patient in transit using the equipment and medications they carry, then coordinate with medical control and the receiving facility as needed. This is why crew capability matters more than the vehicle alone. |
| Can ICU transfers be international? | Yes, but they are more complex. In addition to the medical plan, teams may need passport documentation, customs coordination, receiving hospital acceptance across borders, and careful timing around airport and ground operations. |
| Will insurance cover the transfer? | Sometimes fully, sometimes partially, sometimes after review. Ask who is handling authorization, whether the provider is in network, and what financial responsibility remains if the claim is denied or reduced. |
| Can a family member ride along? | Sometimes. It depends on the patient's condition, vehicle configuration, and safety policy. If a family member can't accompany the patient, ask how departure and arrival updates will be communicated. |
If you are managing this situation right now, keep the process simple. Ask who is accepting the patient, whether the patient is stable for transport, what vehicle is being used, who owns the insurance paperwork, and how the bedside handoff will occur. Those questions reveal very quickly whether the transfer is ready.