The call usually comes when two clocks are already running. One is in the donor hospital, where recovery timing is narrowing by the minute. The other is in the recipient center, where a surgical team is standing by and every handoff has to work the first time.
The Race Against Time An Introduction to Organ Recovery Transport
Organ recovery transport isn't just about moving a cooler from one city to another. It's the operational bridge between a successful donor recovery and a viable transplant. If that bridge fails at any point, through delay, miscommunication, poor packaging, or the wrong aircraft choice, the mission can fail long before the recipient reaches the operating room.
The scale of the need is enormous. More than 90,000 Americans remain on the waiting list for kidney transplants alone, and over 100,000 people nationally are waiting for lifesaving organ transplants. In 2025, the United States performed 49,064 organ transplants according to UNOS transplant activity reporting. Those aren't abstract figures to operators. They represent a constant stream of missions where timing, packaging, routing, and accountability all matter at once.
The crucial pressure points are often overlooked. It's not only in the air. It's in the handoffs. The transfer from recovery team to preservation team. The release from hospital loading area to courier. The decision to hold for weather or reroute. The choice between waiting on a commercial connection or launching a dedicated aircraft now.
Where minutes are won or lost
A transport plan succeeds when the entire chain is built backward from the organ's viability window. That means choosing the airport closest to the recipient center, limiting ramp time, and avoiding fragile itineraries with too many dependencies. In aviation terms, small operational gains matter. A useful parallel appears in this discussion of hangar optimization for faster jet travel, because aircraft readiness and ground access often affect mission timing as much as flight time itself.
Practical rule: The fastest mission isn't always the one with the shortest airborne leg. It's the one with the fewest failure points between recovery and surgical handoff.
Families often ask, “Isn't this just expedited shipping?” It isn't. Organ recovery transport is a medical logistics mission under clinical time pressure, with chain of custody, preservation requirements, and no room for casual assumptions. Every decision has consequences, and the margin for error is much smaller than most nonmedical transport teams realize.
The Organ's Journey Deconstructing the Transport Process
The cleanest way to understand organ recovery transport is to think of it as a relay race. No single team “does the transport.” One team recovers the organ. Another preserves and documents it. Another moves it. Another receives it and confirms identity, condition, and readiness for implantation.
If one runner is late, the baton doesn't move.
Recovery starts the transport clock
The process begins when the donor case has advanced far enough that transport planning can't wait. Surgical recovery timing, recipient readiness, and destination logistics all begin converging at once. From an operations standpoint, experienced teams stop thinking in broad estimates and start locking in exact people, routes, and contingencies.
The first handoff usually happens inside the donor hospital. The organ is recovered by the surgical team, then passed into a preservation workflow that includes packaging, labeling, and transport documentation. That handoff has to be disciplined. If a container isn't sealed correctly or the paperwork package isn't complete, the mistake follows the mission downstream.
Preservation and dispatch happen together
A common misconception is that transport gets arranged after packaging is complete. In strong programs, those tracks run in parallel.
While clinicians package and document, logistics teams are confirming:
- Pickup location details so the courier or air crew isn't losing time in a large hospital footprint
- Airport access and curfews that could affect departure or arrival windows
- Ground transfer timing at both ends so the organ doesn't sit on a ramp or in traffic
- Receiving team availability so delivery matches operating room readiness
That parallel planning is what keeps the relay smooth.
The dangerous part of organ transport isn't usually one dramatic failure. It's a stack of small delays that nobody corrected early.
Transit is only one leg
Once the organ leaves the donor site, the mission shifts to controlled movement. That may involve a ground courier, a commercial itinerary, or a dedicated aircraft. During this phase, the most important work is often invisible: status verification, ETA updates, confirmation that preservation conditions remain intact, and preparation for the next handoff before the current one is finished.
On arrival, the transport team does not just “drop off” the organ. The receiving clinical team verifies identity, documentation, package integrity, and the immediate transfer path into the transplant workflow. The arrival handoff must be just as precise as the departure handoff.
The shortest summary
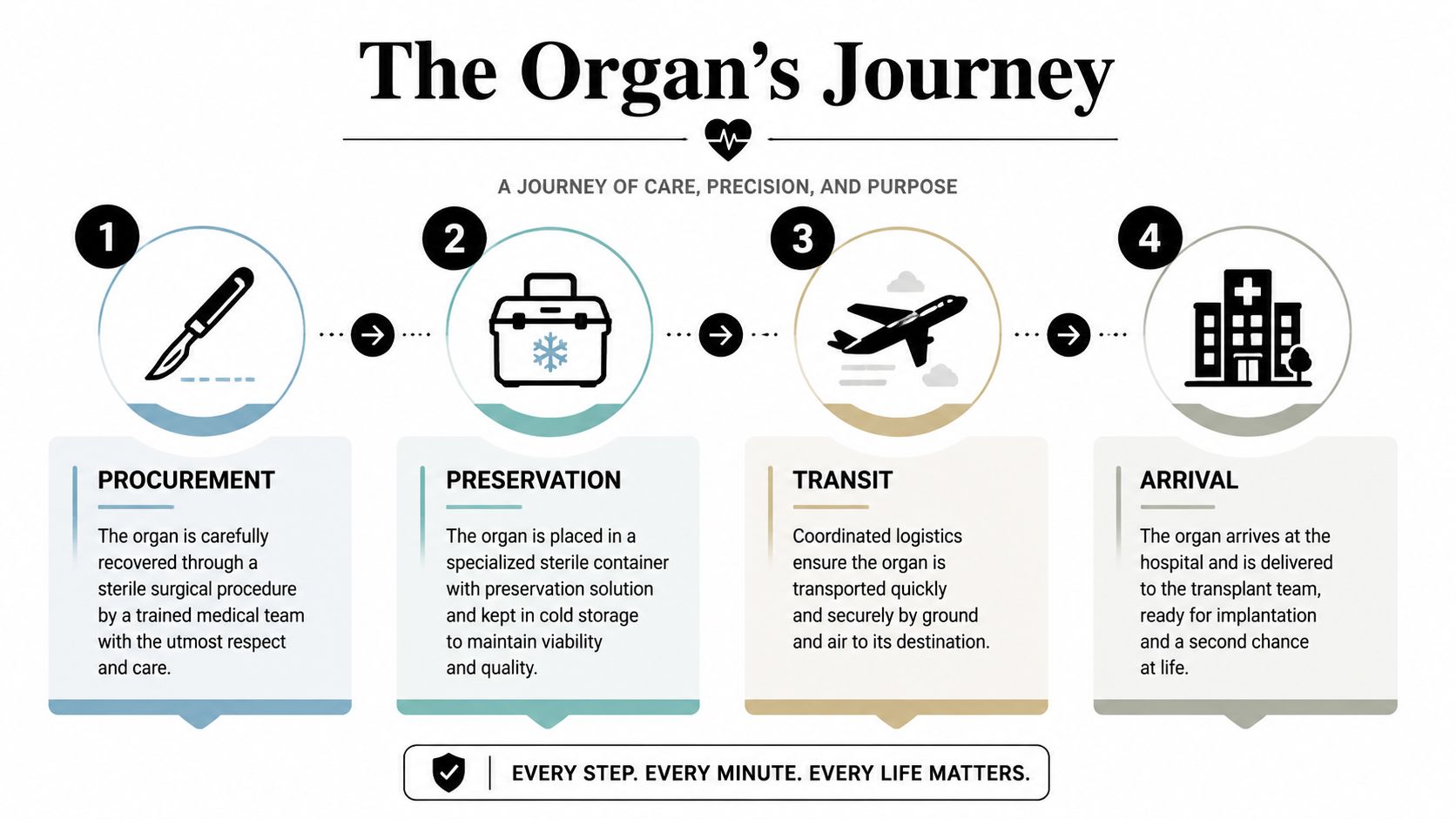
The journey looks like four simple steps. In practice, it's a tightly managed sequence:
- Recovery inside the donor hospital
- Preservation with packaging and documentation
- Transit using the fastest reliable mode for the clinical window
- Arrival with immediate, documented handoff to the recipient center
That's the whole mission. Keep the baton moving. Don't improvise at the exchange points.
The Players Who Coordinates Organ Transport
A successful organ recovery transport mission depends less on heroics than on role clarity. Problems start when teams assume someone else has already handled a detail. Strong missions work because each party knows exactly what it owns, what it must confirm, and when it must speak up.
The industry around this work keeps expanding. The global Organ Transport Service Market was valued at USD 3.68 billion in 2026 and is projected to reach USD 5.25 billion by 2030, driven by increasing transplant procedures, expanding transplant center networks, and growth in emergency medical logistics services, according to the organ transport service market report. That growth makes one point very clear. More participants are entering the space, but organ missions still demand specialized coordination standards.
Who does what
The Organ Procurement Organization usually acts as the central coordinator on the donor side. It aligns donor hospital activity, communicates timing, and helps connect the recovery timeline to the transport timeline.
The donor hospital clinical team handles the recovery environment. That includes patient care, operating room access, and support around packaging and release procedures.
The recipient transplant center decides whether the organ can be accepted, confirms recipient readiness, and prepares for immediate receipt and implantation. If the receiving team isn't synchronized with the route plan, transport speed alone won't save the mission.
The transport provider owns movement. That means aircraft or ground asset selection, route planning, dispatch, communications, and contingency management. In a good operation, the transport team also pressure-tests assumptions that others may not see, such as airport operating limitations or ground access bottlenecks.
Why freight experience isn't enough
People sometimes ask whether any urgent logistics company can handle this work. The short answer is no. General cargo knowledge helps, and a primer on fast air freight solutions can be useful for understanding expedited movement principles, but organ transport adds clinical packaging rules, chain of custody, medical accountability, and time windows that are far less forgiving than standard freight.
A hospital case manager also needs practical tools, not just theory. For coordination checklists and transfer planning support, the case worker toolkit for medical transport planning is a useful reference point.
The coordination failure to avoid
The most common breakdown isn't a pilot problem or a weather problem. It's fragmented communication.
Watch for these warning signs:
- Multiple decision-makers with no single point of operational control
- Unclear release authority at the donor hospital loading point
- Loose ETA updates that leave the receiving team guessing
- Assumptions about ground transport instead of confirmed vehicles and drivers
Operational note: The best transport coordinator acts like an air traffic controller for the whole mission, not just the airplane.
That's what families and case managers should expect. Not vague reassurance. Clear ownership.
The Clock is Ticking Clinical and Packaging Requirements
The clinical side of organ recovery transport dictates the logistics, not the other way around. Aircraft availability matters. Couriers matter. Weather matters. But the governing reality is organ viability outside the body. That's why transport teams build plans around cold ischemia time, packaging integrity, and chain-of-custody discipline from the first call.
Why preservation drives the route
Different organs tolerate out-of-body time differently, so not every mission has the same operational flexibility. A kidney shipment may allow more routing options than a heart or lung mission. That single fact changes everything, from airport selection to whether a commercial connection is acceptable.
Here's the practical planning view.
| Organ | Maximum Preservation Time |
|---|---|
| Heart | Short window, requires the fastest and most direct routing |
| Lung | Short window, often demands highly controlled scheduling |
| Liver | Moderate window, but still sensitive to avoidable delay |
| Pancreas | Moderate window, requires strict packaging and tracking |
| Kidney | Longer window than other major organs, but still time-sensitive |
The exact acceptable window is determined by the transplant program and the preservation method in use. Operators should never guess. They should confirm the clinical requirement for that specific mission and build the route around it.
Packaging isn't just a cooler
People outside transplant logistics often picture a cooler and ice. Real organ transport packaging is more controlled than that. Teams use sterile barriers, secure outer containers, labels, documentation packets, and temperature controls appropriate to the organ and preservation method. Every layer exists for a reason: sterility, traceability, impact protection, thermal stability, and handoff confidence.
For readers who want a basic logistics comparison between protective materials and transport supplies, this warehouse shipping and packing materials guide helps explain why the container system matters. Organ transport applies those distinctions under much stricter clinical standards.
A provider also needs the right onboard support equipment when the mission calls for it. Resources on aero medical supplies used in transport operations are relevant because compatibility between aircraft space, securing points, and medical packaging can affect whether a device-based preservation setup can travel safely.
Where advanced preservation changes the decision
Hypothermic machine perfusion (HMP) changes the planning picture for kidney transport. Devices using HMP preserve kidneys by pumping physiologic solutions at 4-8°C, extending viability to 24-36 hours versus 18-24 hours with static cold storage, according to Organ Recovery Systems information on kidney preservation technology. In practice, that can create options that wouldn't exist with static cold storage alone.
That doesn't mean transport teams can relax. It means they can make a smarter mode decision when distance, weather, or operating room timing complicate the mission.
Chain of custody is part of patient care
An organ can be well preserved and still be placed at risk by sloppy documentation. Every handoff should confirm identity, packaging condition, sender, receiver, timing, and destination. There shouldn't be any “I thought they had it” moments in this work.
Use a hard checklist for these points:
- Container verification before departure, during handoff, and at arrival
- Temperature confirmation when applicable to the packaging method
- Document packet control so nothing gets separated from the shipment
- Named receiving contact at the destination hospital, not just a department name
Good packaging protects the organ. Good documentation protects the mission.
Wheels Up Choosing the Right Transport Mode
Mode selection is where experience shows. On paper, ground, commercial air, and dedicated air ambulance can all move an organ. In actual operations, only one may fit the organ's time window, the route's geography, and the mission's risk profile.
The wrong mode usually looks cheaper or simpler right up until it fails.
Ground, commercial, or dedicated aircraft
Ground transport works when distance is short, traffic is predictable, and there's no advantage in adding airport handling. It can be the cleanest option for local or tightly clustered regional transfers. It becomes a poor option when congestion, night closures, or long highway segments introduce uncertainty.
Commercial airline transport can work for some planned routes, especially when schedules line up and airport handling is dependable. The trade-off is loss of control. If the organ misses a connection, waits on a delay, or gets trapped in airport processes that weren't built for transplant urgency, the mission starts absorbing risk quickly.
Dedicated air ambulance or chartered fixed-wing transport becomes the only viable choice when the mission needs direct routing, short-notice launch, airport flexibility, and an operations team that can control the full chain. That's often the deciding factor for longer interstate missions, complex geography, or short clinical windows.
When a dedicated aircraft is the only real option
Dedicated air transport is not about prestige. It's about removing dependencies.
Choose a dedicated aircraft when:
- The organ's viability window is tight and a missed connection isn't acceptable
- The donor and recipient centers are geographically separated by long driving times or inefficient airline paths
- Weather or airport constraints require rapid rerouting authority
- The handoff involves specialized equipment that needs secure placement and monitored handling
Safety standards matter just as much as speed in this context. National standards for organ recovery transport emphasize twin-engine, turbine-powered aircraft with two qualified pilots, a protocol established to mitigate risks highlighted by a tragic 2007 crash, as outlined by UNOS guidance on safer organ recovery transportation. In practice, that standard tells coordinators what kind of aircraft setup belongs on a serious mission.
Fixed-wing decisions are operational decisions
If you're comparing aircraft types more broadly, this overview of fixed-wing vs rotary-wing medical transport is useful. For organ recovery transport, fixed-wing aircraft usually make sense when the route is longer, airport-to-airport transfer is practical, and you need speed with range.
A helicopter can be valuable for short hops or difficult local access. It's rarely the primary answer for cross-state organ movement where distance, weather exposure, and payload considerations favor fixed-wing planning.
A dedicated aircraft earns its keep when the mission can't tolerate someone else's schedule.
What doesn't work
What fails most often is trying to force a borderline mission into a cheaper mode. If the route only works when every connection is perfect, it doesn't really work. If the airport is convenient for the carrier but adds substantial ground time at the destination, it's the wrong airport. If the crew can fly the mission but can't support the packaging or equipment requirements, it's the wrong aircraft.
Transport mode should be chosen by the organ's needs. Not by habit. Not by convenience.
How to Coordinate an Organ Transport Flight
When a case manager or transplant coordinator reaches out for a flight, speed matters, but clarity matters more. The fastest way to lose time is to start the call without the details the dispatch team needs to make real decisions.
A hard lesson from the field is that transport friction is not hypothetical. Between 2014-2019, 170 organs were lost and 370 delayed over 2 hours due to transport issues, according to reporting on organ transport disruption and new hybrid models. That's why the intake process has to be disciplined from the start.
What to have ready before you call
The first conversation should answer operational questions, not create new ones.
Prepare these basics:
Pickup and delivery locations
Give exact hospitals, departments, and access points if known. Large campuses can waste precious time if the crew receives only the hospital name.Organ type and preservation setup
The transport provider needs to know whether this is standard cold storage or a device-supported preservation mission.Ready time and latest acceptable arrival
Dispatch can't choose the right mode without both ends of the window.Handoff contacts
Provide names and direct phone numbers for the sending and receiving personnel.Special constraints
Mention weather concerns, airport preferences, aircraft access limits, or security restrictions early.
Questions to ask the provider
Don't ask only, “How fast can you go?” Ask how the mission will be controlled.
A strong checklist includes:
- Who owns dispatch on this mission?
- Will you coordinate ground transport, or do we need to arrange it separately?
- How do you handle weather reroutes or airport changes?
- How will status updates be communicated during transit?
- Can you accommodate specialized preservation equipment if needed?
Those questions reveal whether the provider is running a full medical logistics operation or offering aircraft time.
Ask this directly: “Who is my single point of contact from launch through final handoff?”
What the coordination flow should look like
After intake, the provider should validate route feasibility, aircraft suitability, crew readiness, and airport access. Ground transfers should be matched to wheels-up and wheels-down times, not booked as a separate afterthought. The receiving side should know who is arriving, from where, and at what handoff point.
This short video gives useful context on how air medical coordination works in practice:
What families and case managers should expect
A seasoned provider should sound calm, specific, and organized. You should hear route logic, contingency planning, and handoff confirmation. You shouldn't hear vague promises.
The right coordination style includes:
- Clear acceptance criteria for the mission
- Direct language about limitations or risks
- Regular status updates at defined points
- Documented handoff planning before the aircraft departs
That's what good organ recovery transport sounds like. Measured. Precise. Controlled.
Frequently Asked Questions About Organ Transport
What happens if weather affects the flight
Weather doesn't automatically cancel the mission, but it can force a reroute, a different departure airport, or a different transport mode. Strong coordinators plan alternates early and decide quickly when the original route becomes unreliable. The goal is to protect viability, not to defend the first plan.
Can commercial flights still play a role
Yes, in selected cases. Hybrid models are emerging, especially when preservation technology and schedule alignment make commercial segments workable. But commercial options are still less controllable than dedicated aircraft, so they fit only the right mission profile.
Who pays for organ transport
Coverage depends on the transplant arrangement, the clinical setting, and the organizations involved in the case. Families usually shouldn't assume they're the direct payer, and they shouldn't guess. The right move is to ask the transplant center or coordinating organization for the funding path tied to that specific mission.
How is the organ tracked in transit
Programs use chain-of-custody procedures, direct communications between teams, and, in some cases, real-time tracking tools associated with the shipment or preservation method. The important question isn't just whether tracking exists. It's who is watching it and who is authorized to act if the mission starts drifting off plan.
Can a family member travel with the organ
Usually, organ transport itself is handled as a controlled medical logistics movement, not a passenger trip. If family travel is needed around the broader transplant process, that has to be arranged separately and should never interfere with the transport plan.
What makes one provider better than another
Look for operational control, medical transport experience, aircraft and crew standards appropriate to the mission, and confidence at the handoff points. Anyone can promise speed. Fewer teams can explain exactly how they'll protect the mission from donor hospital release through recipient center receipt.
Is a dedicated jet always necessary
No. But when the route is long, the timing is tight, the geography is awkward, or the mission can't risk schedule dependency, a dedicated fixed-wing aircraft often becomes the safest practical choice.
If you need help arranging a time-sensitive medical flight, Med Jets by Air Trek coordinates end-to-end air ambulance transport with experienced crews, fixed-wing aircraft, and 24/7 dispatch support. For urgent planning, families, case managers, and assistance teams can contact the program directly through the company website.