Your mother is medically stable enough to leave the hospital, but she can’t get in a car and go home. She needs oxygen. She gets confused in unfamiliar places. The receiving facility wants records before arrival, and the discharging unit is asking when transport will be confirmed. That’s the moment many families and case managers realize they’re not arranging a ride. They’re arranging a clinical handoff.
That distinction matters in medical transport for seniors. A basic ride solves movement from one address to another. Medical transport solves safety, monitoring, transfers, paperwork, timing, and continuity of care. If the patient is frail, recently hospitalized, mobility-limited, or traveling a long distance, choosing the wrong level of transport can create delays, failed discharges, and avoidable stress for everyone involved.
Understanding Your Senior Medical Transport Options
A common call starts the same way. A daughter says her father was hospitalized while visiting family. He’s improved, but he’s weak, using a walker, and the team doesn’t want him flying alone. She’s already looked at rideshares, wheelchair vans, and standard airline tickets. What she really needs to know is simpler and harder at the same time.
When is a simple ride not enough?
The answer starts with clinical continuity. Many public guides focus on how to get a senior to an appointment, but they stop short of the bigger issue. Families and case managers usually need to know what level of medical support is required for a safe transfer, and who manages the handoff between sending and receiving teams, which is the core gap described in this discussion of ride access versus clinical continuity.
The three broad categories
Most senior transfers fall into one of these groups:
| Option | Best fit | Usually not enough when |
|---|---|---|
| Ground medical transport | Local or regional trips for stable patients who need mobility help | The patient needs intensive monitoring or long-distance travel |
| Medical escort on a commercial flight | Stable patients who can tolerate airport and airline logistics with a clinician beside them | The patient needs stretcher transport, continuous higher-acuity support, or rapid transfer |
| Air ambulance | Long-distance, time-sensitive, or medically complex transfers | The patient can safely use lower-acuity transport |
That’s why families often need more than a booking tool. They need coordination across hospitals, transport teams, equipment, and family communication. Even simple administrative support can help keep details straight. If you’re juggling discharge planning, records, and follow-up logistics, this overview of how virtual personal assistants work can help you think through what tasks can be delegated while the clinical team handles transport.
Practical rule: If the patient’s condition, equipment needs, or transfer risk would make you uneasy during an unmonitored delay, you’re no longer choosing a ride. You’re choosing a care setting in motion.
For higher-acuity transfers, a dedicated medical flight may be the right category to evaluate. Families comparing options often start by reviewing emergency medical transport services so they can see what bed-to-bed coordination includes.
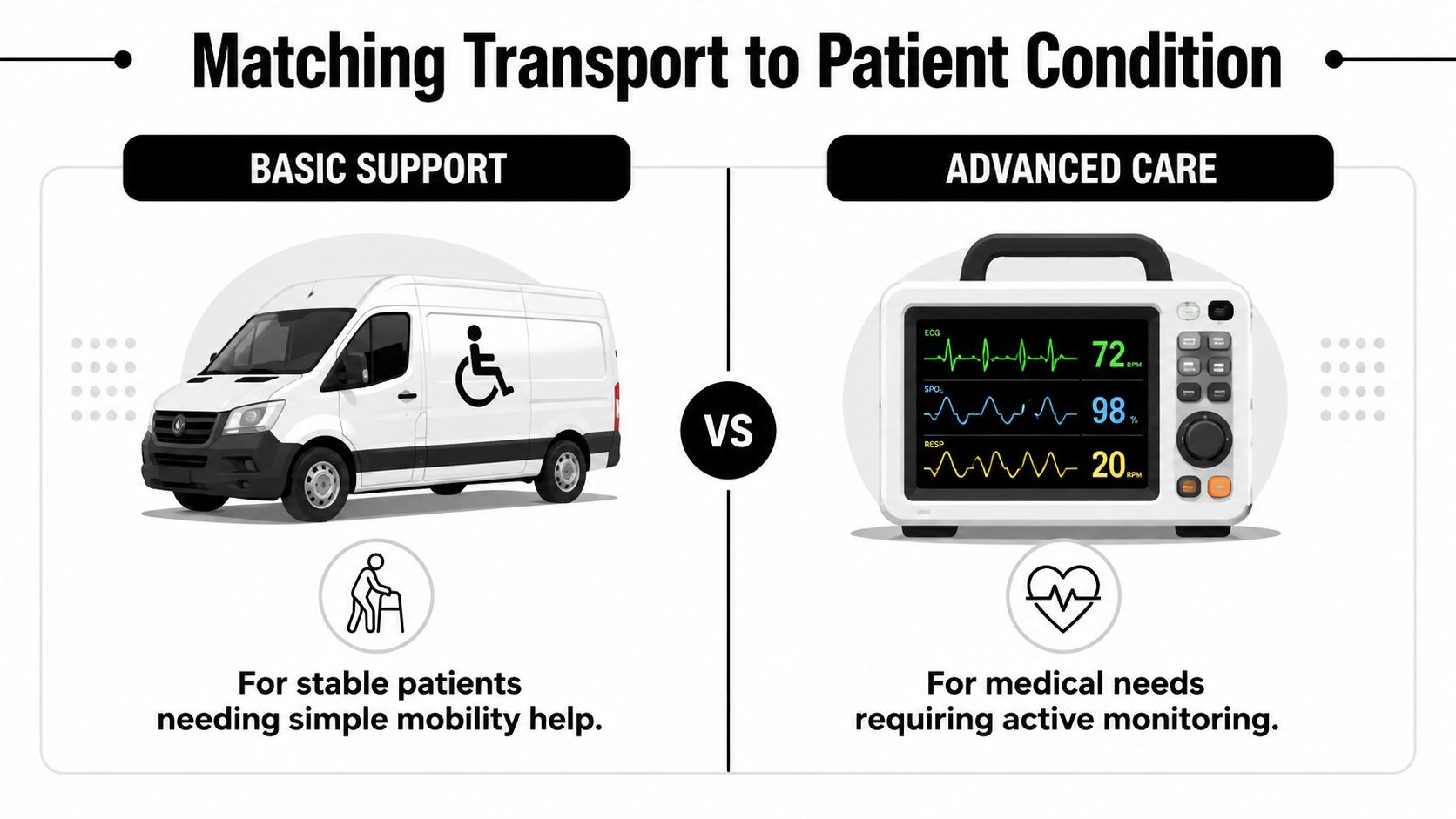
How to Match the Transport to the Patient’s Condition
The safest way to choose transport is to profile the patient first and the vehicle second. Start with the clinical facts. Then work outward to distance, timing, and destination requirements.
A peer-reviewed evaluation found that reliable non-emergency medical transportation was associated with 9.2 additional outpatient visits per person-year (study details). In practice, that reinforces something coordinators see every day. When transport is matched correctly, scheduled care does happen.
Start with these five questions
-
Can the patient sit upright for the full trip?
If yes, you may be looking at ambulatory transport, wheelchair transport, or a medical escort. If no, stretcher-capable transport becomes the starting point. -
Is the patient medically stable without active intervention?
A stable patient may only need supervision, transfer help, and medication timing. A patient needing oxygen titration, continuous observation, suction capability, or higher-level monitoring needs a more clinical environment. -
What happens during transfers?
A senior may tolerate the ride itself but struggle with bed-to-chair moves, bathroom needs, fatigue, or confusion during check-in and boarding. Many failed transports happen during these transition points, not during travel. -
How far is the patient going?
Distance changes everything. A short local move may be manageable by ground. A long interstate or international transfer can turn a stable-looking patient into an exhausted, unstable traveler if the mode is wrong. -
Who must receive the patient at the other end?
Some destinations will accept a basic drop-off. Others need a nurse-to-nurse report, medication list, discharge summary, and confirmed arrival window before they’ll take the patient.
What often changes the decision
The details below frequently push a case from “simple” to “needs medical transport”:
- Cognitive status: A patient with dementia, delirium, or poor safety awareness may need an escort even if they walk.
- Equipment needs: Oxygen, wound support, feeding support, or personal devices all need planning.
- Body size and transfer risk: Bariatric moves require the right vehicle and the right lifting plan.
- Recent hospitalization: Seniors right after surgery, infection, or cardiac events can look better on paper than they perform in transit.
A useful parallel is fall prevention. If you’re evaluating whether a senior can manage standing, turning, and boarding safely, this guide on balance training for seniors offers helpful context on mobility and fall-risk thinking.
The right question isn’t “What transport services are available?” It’s “What could go wrong for this patient between bed A and bed B?”
A quick matching framework
| Patient profile | Likely fit |
|---|---|
| Walks with help, stable, local appointment | Basic senior transport or wheelchair-capable ground service |
| Stable but frail, needs help through airport and flight | Commercial medical escort |
| Needs stretcher, oxygen support, or higher-acuity supervision | Non-emergency ambulance or air ambulance depending on distance |
| Medically fragile, long-distance, coordinated facility transfer | Air ambulance |
What doesn’t work is guessing from labels alone. “Wheelchair transport” tells you how the patient enters the vehicle. It doesn’t tell you whether the service can manage fatigue, confusion, oxygen, or a receiving-facility handoff.
Ground Ambulance, Medical Escorts, and Air Ambulance Explained
Demand for specialized senior transport isn’t a niche issue. It sits inside a larger demographic shift. In the United States, by 2034 seniors are projected to outnumber children, and the need for stretcher-capable vehicles and coordinated hospital transfers is tied to that change, as noted in this overview of senior use of NEMT and demographic demand.
Ground medical transport
Ground transport covers a wide range. At the lower-acuity end, you have wheelchair vans and ambulatory services. At the more clinical end, you have non-emergency ambulances with stretcher capability and trained crews.
Ground is usually the best fit when:
- The distance is local or regional
- The patient can tolerate road time
- The receiving destination doesn’t require a flight-speed transfer
- The main issue is mobility, not in-transit instability
Ground often works well for dialysis, rehab transfers, wound care visits, return trips from hospital to skilled nursing, and other planned moves where the patient’s condition is known and relatively steady.
What fails in ground transport is underestimating the practical burden. A two-hour road move can be hard on a frail senior if they need frequent repositioning, toileting support, or pain control. Even before the wheels move, stairs, narrow hallways, and transfer surfaces can become the primary challenge.
Commercial medical escorts
A medical escort is a clinician who accompanies the patient on a standard commercial flight and manages care needs that can be handled safely in that setting. This option is often overlooked, but it can be an excellent middle ground.
A medical escort is often appropriate when the patient:
- Can sit upright for the trip
- Is stable enough for cabin conditions and airport flow
- Needs medication oversight, supervision, or clinical judgment in transit
- Would not do well traveling alone
For many families, this is the right answer when the parent is weak, anxious, or recently discharged but doesn’t need a full aircraft configured for intensive care. The escort handles coordination, watches for decline, and helps bridge the gap between ordinary travel and true medical transport.
If that sounds close to your situation, reviewing dedicated medical escort services can clarify what support is included before, during, and after the flight.
Air ambulance
Air ambulance is the right choice when the patient needs a higher-acuity clinical environment in transit, or when distance and timing make lower-acuity options unsafe or unrealistic.
Air ambulance becomes the likely fit when:
- The patient needs stretcher transport over a long distance
- Ongoing monitoring is necessary
- The transfer is hospital-to-hospital or facility-to-facility
- Delays, layovers, and multiple handoffs would create risk
One-time labels like “stable” can be misleading. A patient may be stable in a monitored bed with immediate help nearby, but not stable for airport lines, layovers, cabin transfers, and prolonged sitting.
Decision shortcut: If a patient would need medical supervision during every phase of the trip, the transport mode should provide that supervision from start to finish.
One practical example is Med Jets by Air Trek, which coordinates air ambulance, medical escort, and ground transport depending on the patient profile. That kind of multi-modal coordination matters because the safest solution isn’t always the most dramatic one. It’s the one that preserves the patient’s clinical continuity all the way through transfer.
The Process for Insurance Authorization and Private Pay
Payment questions usually arrive right after the clinical decision. The family asks whether insurance will cover it. The case manager asks what documentation is needed. Both are asking the same thing in different language. Can we prove medical necessity, and if not, what’s the private-pay path?
Transportation barriers carry real system costs. One healthcare transportation source says over 3.6 million Americans miss appointments annually because of transportation barriers, and it also describes NEMT as often less than 1% of total healthcare spending while supporting better outcomes and lower costs (healthcare transportation management overview).
Insurance authorization
Insurance review usually turns on one issue. Why is this level of transport medically necessary for this patient on this date?
That means the request has to connect the patient’s condition to the transport mode. Strong authorization packets usually include:
- Physician documentation: Why lower-acuity transport isn’t appropriate
- Current clinical status: Mobility limits, oxygen needs, cognitive concerns, recent events
- Origin and destination details: Why the receiving facility is appropriate and prepared
- Transfer requirements: Stretcher, monitoring, escort, special equipment, or bariatric handling
Case managers often improve approval odds by being precise. “Needs transport” is weak. “Cannot tolerate commercial travel due to stretcher requirement and supervised interfacility transfer needs” is clearer and easier for a reviewer to evaluate.
For families sorting through Medicare questions, this guide on whether Medicare covers air ambulance is a practical starting point.
Documentation tip: The insurer doesn’t authorize stress. It authorizes documented medical need.
Private pay
Private pay becomes the path when coverage is excluded, authorization is delayed, or the family chooses speed and control over a long review cycle. That’s common in cross-country moves, repatriation, non-covered destinations, or situations where everyone agrees the transfer should happen quickly.
When reviewing a private-pay quote, look for these details:
| What to confirm | Why it matters |
|---|---|
| Bed-to-bed scope | Tells you whether ground segments and handoffs are included |
| Clinical crew level | Confirms whether the staff matches the patient’s needs |
| Equipment included | Prevents surprises around oxygen, stretcher, or special support |
| Cancellation terms | Important when discharge timing changes |
| Who coordinates records | Reduces last-minute failures |
What doesn’t work is comparing quotes as if they were airline tickets. A lower number may reflect fewer services, fewer transfer points covered, or less clinical support than the patient needs.
Your Pre-Transfer Checklist for Patients and Families
Once transport is booked, anxiety usually shifts from “what should we choose?” to “what do we need ready?” A smooth transfer depends on preparation that is both clinical and practical.
What to gather before the day of travel
Use one folder, digital or paper, and keep the latest version of everything in it.
- Medical records: Discharge summary, medication list, recent physician notes, and current orders
- Identity and insurance items: Photo ID, insurance cards, and facility contact sheet
- Destination contacts: Unit number, receiving clinician contact, admissions desk, and after-hours line
- Personal essentials: Glasses, hearing aids, chargers, dentures, labeled belongings, comfort item
If the patient uses personal medical equipment, confirm battery status and charger access. Don’t assume the sending unit packed those items.
What families should confirm with the coordinator
Call and verify the details that are easiest to misunderstand:
- Pickup window: Not just the date, but the realistic handoff time
- Mobility plan: Can the patient bear weight, pivot, or only transfer with full assistance?
- Escort policy: Who can travel with the patient, if anyone
- Medication timing: Which doses should be given before departure
- Arrival procedure: Who signs, who receives report, and what happens if the bed isn’t ready
One family spokesperson helps more than is typically expected. When three relatives call separately, details drift.
Here’s a quick visual reminder of the kinds of practical details that matter on transfer day:
Day-of-transfer checklist
Bring less than you think, but bring the items the patient cannot safely do without for a delayed day.
- Dress for access: Loose clothing, layers, non-slip footwear if the patient will stand at all
- Label medications and devices: Especially if items may be handed between teams
- Manage expectations: Travel days often involve waiting, reassessment, and timing changes
- Protect the handoff: Make sure the receiving facility knows the estimated arrival time and patient status
What works best is simple. One bag. One document packet. One main family contact. One transport coordinator who can answer the question, “What happens next?”
Ensuring Continuity of Care Upon Arrival
Arrival is where families often relax too early. The trip isn’t finished when the vehicle or aircraft stops. It’s finished when the patient is accepted, report is given, and the receiving team has what it needs to continue care without guesswork.
That final handoff is why medical transport for seniors should be viewed as bed-to-bed coordination, not just door-to-door movement.
What a good arrival looks like
The receiving team should get a concise clinical report details the patient’s condition during transport, medications or support provided in transit, current status on arrival, and any changes the crew observed. Families don’t need a dramatic presentation. They need a clean transfer of responsibility.
If the patient has cognitive impairment, handoff quality matters even more. Staff need to know what calms the patient, what triggers agitation, how they communicate discomfort, and whether a family member should stay briefly during transition. For caregivers dealing with that side of the move, this guide on managing dementia patient behavior offers practical communication ideas.
Why this last step matters
In the U.S., 4.5% of adults age 65 and older reported lacking reliable transportation in the previous year, according to the CDC’s data brief on transportation barriers. For frail seniors, even environmental barriers like broken sidewalks can interfere with getting to care. Coordinated medical transport addresses more than movement. It protects access, timing, and safety.
A transport plan is complete only when the receiving team can continue care without having to reconstruct what happened on the way.
The families and case managers who manage this well usually follow the same pattern. They assess the patient objectively, choose the transport mode based on clinical continuity, prepare thoroughly, and protect the final handoff. That’s careful coordination, but it’s also advocacy. For a senior who is vulnerable, tired, or far from home, it can make the difference between a difficult trip and a safe one.