When a hospital tells you a loved one needs to move today, often, the focus is on the destination. Which facility? How fast? Ground or air? Those questions matter, but they miss the harder one.
Who is responsible for the patient during the move?
That's where patient transport training starts. Safe transport isn't just loading someone onto a stretcher and driving or flying to another building. It's a clinical handoff in motion. The crew has to manage the patient, the equipment, the communication, and the risks that change minute by minute once the room and the bedside team are gone.
Families often ask a version of the same thing. “Will they monitor him the whole way?” “What if her oxygen drops?” “Who makes sure the receiving hospital gets the full report?” Those are the right questions. The safest transport teams think about transfer as active care, not movement.
What Is Patient Transport Training
Patient transport training is the preparation crews need to move a patient safely while protecting the basics of care. That includes assessment before departure, securing lines and devices, monitoring during the trip, communicating with sending and receiving teams, and knowing exactly what to do if the patient worsens en route.
In older models, transport was often treated as a technical task. Move the patient. Avoid a fall. Get there. Modern practice is much more serious because the risks are real. The Anesthesia Patient Safety Foundation notes that intrahospital adverse events during transport or within 24 hours can approach 80% in some studies, and 4% to 9% of transported patients have required medical intervention because of transport-related adverse events, according to the APSF discussion of intrahospital patient transport risks and checklists.
Why transport is a care event
A patient leaving a unit loses some of the protection of that unit. The bedside nurse isn't right there. Respiratory therapy may not be right there. The room oxygen source is gone. Wall suction is gone. Extra hands are gone.
That's why good patient transport training covers more than lifting mechanics:
- Pre-transport assessment that checks airway, breathing, circulation, stability, medications, and device needs
- Role clarity so every crew member knows who leads, who watches monitors, who manages the airway, and who handles documentation
- Emergency escalation so deterioration triggers a practiced response, not confusion
- Repeated competency checks because transport skills decay if crews don't rehearse them
Practical rule: If a provider talks only about vehicles and response times, and not about monitoring, handoff, and escalation, you're hearing a logistics pitch, not a clinical transport plan.
What families should listen for
A strong program won't describe transport as “just getting them there.” It will describe a sequence:
- Assessment before movement
- Stabilization before departure
- Monitoring throughout transport
- Structured report on arrival
That language matters. It tells you the team sees transport the way experienced clinicians do. As a vulnerable period where small misses become major problems.
Core Competencies of Elite Transport Teams
The safest crews are built on four connected pillars, much like building a house. If the foundation is weak, the walls won't matter. If the wiring is poor, the lights fail even if the frame looks good. Elite transport teams work the same way. Clinical skill alone isn't enough.
A useful visual summary is below.
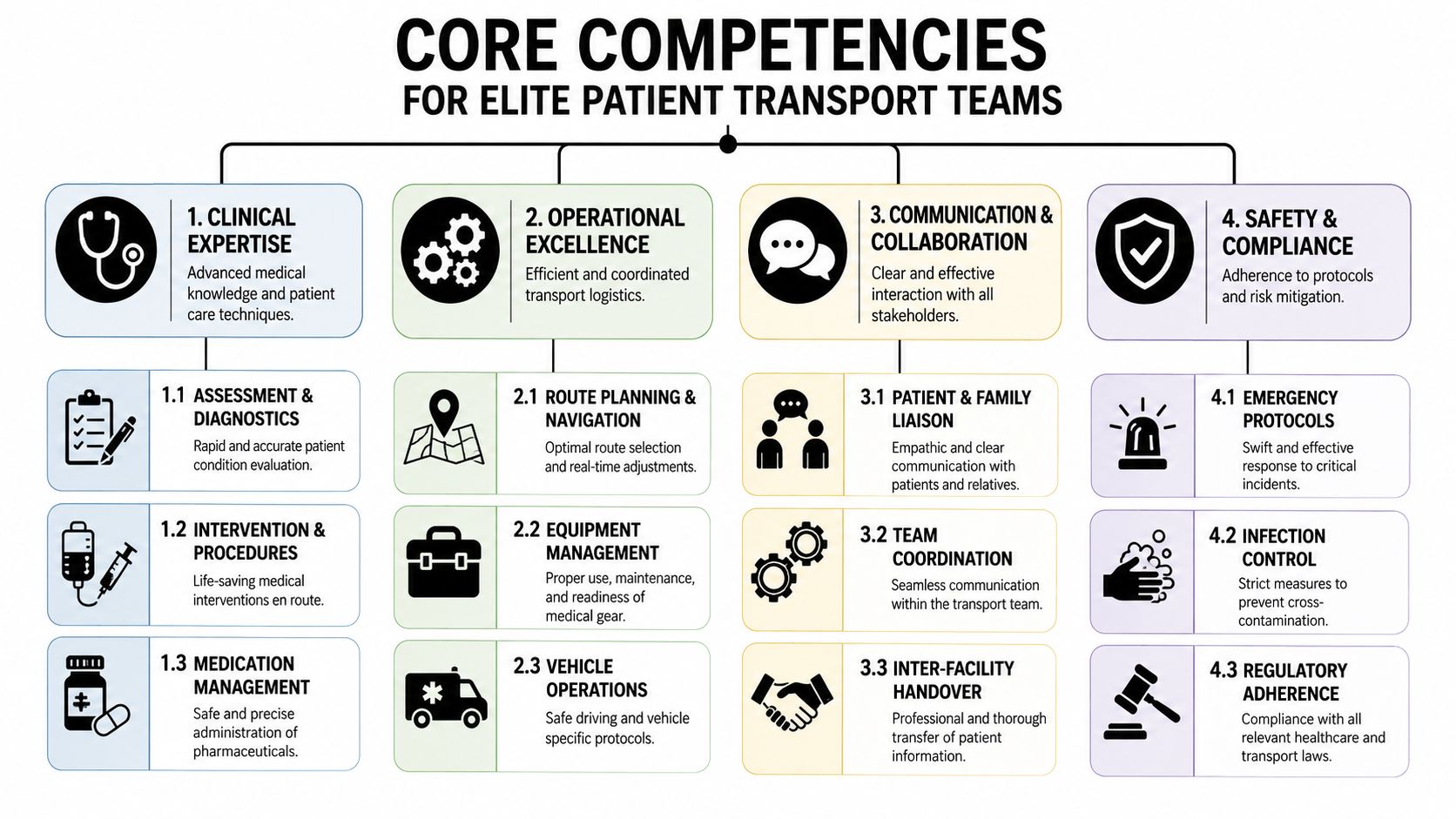
Clinical proficiency
This is the foundation. Crews need to recognize what the patient looks like now, what could go wrong next, and what interventions may be needed before arrival.
That means more than reading vitals off a screen. It means noticing a tiring respiratory pattern before oxygen saturation falls. It means deciding whether pain, agitation, bleeding, secretions, or pressure issues are likely to create trouble in transit. It also means understanding how medications, ventilators, oxygen devices, and infusions behave outside the hospital room.
Safety and risk management
Transport teams have to think ahead. Every move is a chain of hazards. Tubing can snag. A stretcher can shift. A patient can decompensate during a transfer between bed, cot, aircraft, and receiving bed.
Public descriptions of transfer training often stop at movement techniques, but safer transfers require identity checks, airway, breathing, and circulation assessment, line and monitor management, and a risk-benefit decision before each inter-facility transfer, as described in the American Medical Compliance overview of patient transfer training.
What doesn't work is generic “be careful” training. What does work is specific preparation for predictable failure points.
Equipment mastery
A crew can't be slow with equipment. They need to know it well enough to use it under pressure, in a cramped space, with noise, vibration, or poor lighting.
That includes transport monitors, suction, oxygen systems, infusion pumps, stretchers, and specialty gear. It also includes knowing whether the right gear was loaded at all. A family may never see that side of patient transport training, but case managers should ask about it.
If a program coordinates complex flights or escorts, the quality of aeromedical supplies and transport equipment planning tells you a lot about how seriously it treats the mission.
A short look at transport teamwork in action helps here.
Communication and handoffs
At this juncture, many transports succeed or fail. Often, the primary danger isn't the lift. It's the missed detail.
A blood pressure trend isn't passed along. A drain gets mentioned casually instead of clearly assigned. A receiving team isn't told that the patient needed more oxygen during loading. Good crews close those gaps. They give concise, structured reports. They confirm names, medications, current status, and what changed during transport.
The handoff isn't paperwork at the end. It's part of patient care from first contact to arrival.
If you want one dividing line between basic and elite teams, it's this. Basic teams move patients. Elite teams manage transitions.
Understanding Transport Certifications and Standards
The letters after a clinician's name matter, but only if you know what they mean. Families and case managers see credentials like CFRN, CTRN, CNPT, or FP-C and often assume they're just professional shorthand. In transport medicine, they signal a crew member has trained and tested for a harder environment than routine bedside care.
What the certifications tell you
These credentials don't guarantee perfection. They do tell you the provider has pursued transport-specific knowledge rather than relying only on a base license.
Global Trauma Quality standards set a high bar for critical care transport teams. They state that providers should have at least 3,700 hours of critical care patient contact or 5 years of critical care experience, and that at least one provider should hold a specialty certification such as CFRN, CTRN, CNPT, or FP-C. The same standards tie competency progression to 150 critical care transports. You can review those benchmarks in the Global Trauma Quality critical care transport standards.
That matters because transport medicine is a different discipline. A clinician may be excellent in an ICU and still need additional training to function well in a moving vehicle, in a confined cabin, or during a cross-country transfer.
What to ask instead of “Are you certified”
Ask questions that make the answer concrete:
- Which transport certifications does the clinical crew hold
- How much critical care experience do your transport clinicians have
- How are new crew members cleared for independent transport
- How many supervised critical care transports are required before full release
Those questions are much more useful than a vague promise that the team is “highly trained.”
Standards also cover equipment and mode-specific safety
One detail experienced teams pay attention to is that standards become more specific as patient complexity rises. In air transport, for example, airway management has to account for changes in pressure and altitude. The Global Trauma Quality standards specify an endotracheal cuff pressure manometer for air transport modes, which is the kind of detail that separates transport medicine from ordinary transfer work.
Case managers who need to verify transport readiness often look beyond the clinical side and check operational qualifications too, especially when flight crews and pilots are part of the mission. That's where a provider's approach to pilot medical certification requirements can help complete the picture.
Credentials are useful when they map to real exposure, real supervision, and a clear standard for release to practice.
How Medical Transport Crews Are Tested
The best testing doesn't happen when everything is calm. It happens in drills designed to make teams uncomfortable on purpose.
A strong transport program puts crews into scenarios where something changes halfway through the move. The monitor alarms during loading. Oxygen delivery becomes unreliable. A patient who looked stable starts working harder to breathe. The point isn't to “trick” the crew. The point is to see whether they can think, communicate, and act without losing control of the scene.
What simulation should look like
Good simulation is specific. It doesn't ask, “Can you move a patient?” It asks whether the team can move this patient with this equipment, using this staffing pattern, while following the same safety rules they'd be held to in the field.
Formal standards from the Association of Surgical Technologists include concrete transport protocols. A conscious, mobile patient requires at least two team members, while a nonmobile, conscious or unconscious patient requires at least four to reduce injury risk. The same standards also require securement of lines, drains, and monitors, along with side rails, safety straps, and transfer devices for nonmobile patients, as laid out in the AST standard for patient transportation.
That gives educators something testable. Not “Did the transfer seem fine?” but “Did the crew use the correct number of people, secure the devices, and protect the patient throughout the move?”
What gets evaluated beyond procedures
A realistic drill tests several layers at once:
- Scene organization so the team doesn't crowd itself or lose track of responsibilities
- Closed-loop communication so verbal orders are heard and confirmed
- Mechanical safety so lines, catheters, drains, and monitors stay controlled
- Clinical judgment so teams know when not to proceed until a problem is fixed
I've always trusted crews more when they train to stop a transport as confidently as they train to start one. A rushed departure is one of the easiest ways to create a problem that follows the patient the rest of the day.
What families and planners can ask
You don't need technical language to get a useful answer. Ask:
| Training area | Question to ask | Good sign |
|---|---|---|
| Simulation | How do you rehearse emergencies during transport? | They describe realistic scenarios, team roles, and debriefing |
| Staffing safety | How do you train crews for bed-to-stretcher or stretcher-to-aircraft transfers? | They mention staffing, device securement, and patient-specific plans |
| Competency review | How do you know a clinician is still ready for this level of transport? | They describe recurrent testing, observation, and sign-off |
A provider that answers with specifics usually has a real training culture. A provider that answers in slogans usually doesn't.
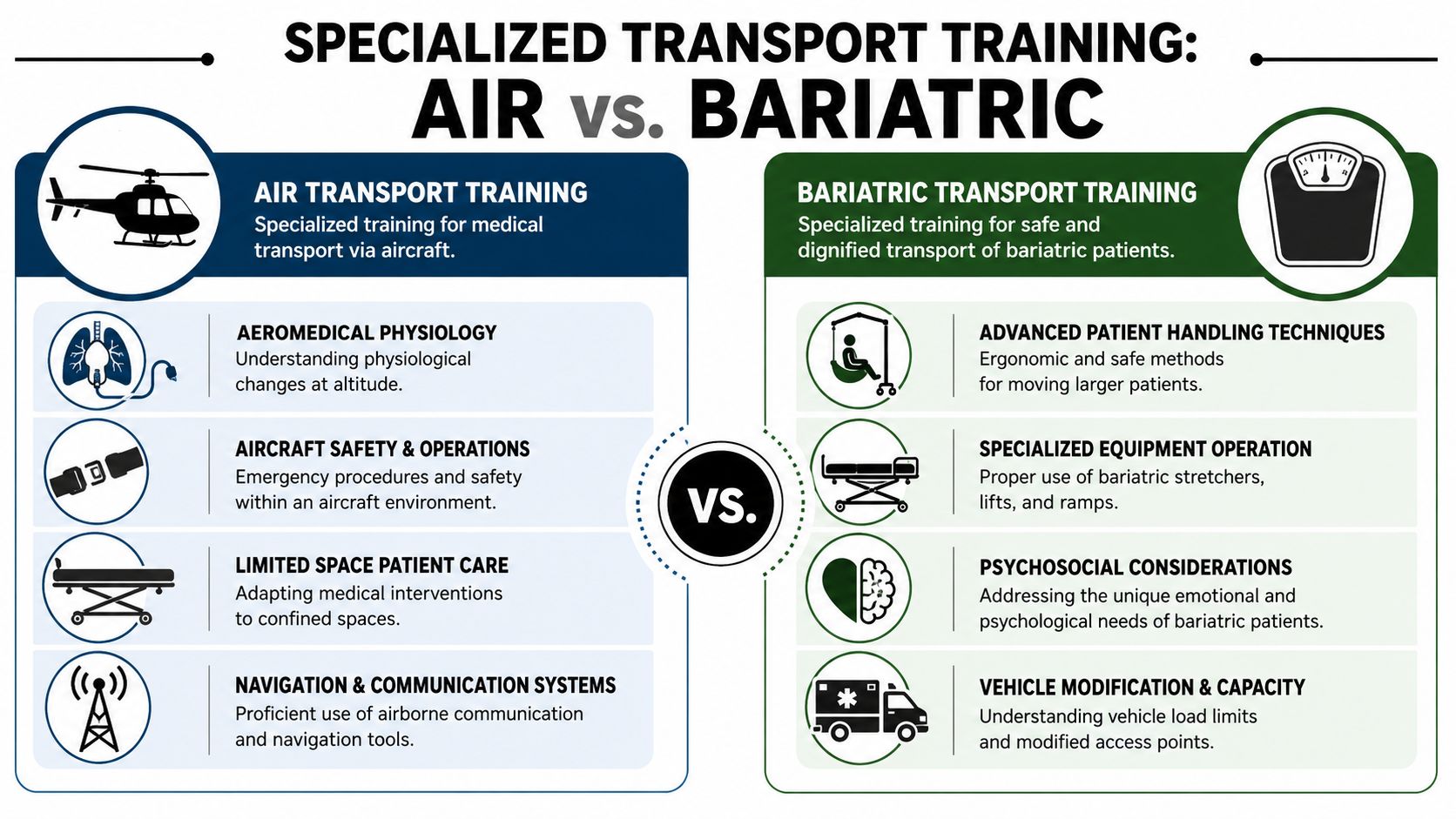
Specialized Training for Air and Bariatric Transport
Not every patient needs the same transport plan. A stable medical escort on a commercial airline isn't the same mission as an ICU-level jet transport. A standard stretcher transfer isn't the same as a bariatric move through narrow hallways and aircraft doors. Patient transport training has to match the actual job.
The comparison below helps show why one-size-fits-all training breaks down fast.
Why specialization matters more now
Transport volume is not a niche issue. One study reports that one in twenty hospital admissions results in an interhospital transfer, equal to approximately 1.7 million patients transferred annually, and the patient transport services market was valued at USD 49.02 billion in 2026 and projected to reach USD 75.49 billion by 2030, as cited in the PMC article on interhospital transfer volume and market growth. More transfers and more service types mean more need for crews who know the differences, not just the basics.
Air transport training
Air medical crews work in a space where medicine and aviation constantly interact. The cabin is tighter. Noise is higher. Access to the patient can be worse. Loading and unloading are more technical. Some interventions become harder because there's less room to move.
Training for these missions usually centers on:
- Aeromedical physiology so crews understand how flight conditions affect the patient and equipment
- Aircraft safety procedures including loading zones, restraint rules, and emergency coordination with pilots
- Confined-space care because reaching the airway, pump, or monitor may require a different setup than in a ground unit
- Aviation communication so clinical and flight teams stay coordinated during departure, changes, and arrival
Programs may also use different staffing models depending on the mission. Some transfers need a dedicated flight team. Others may be appropriate for pediatric flight nurse and specialty escort support when the patient profile calls for that level of training.
Bariatric transport training
Bariatric transport isn't just “use bigger equipment.” That's one part of it. The primary task is preserving safety and dignity while reducing strain on the patient and the crew.
Strong training covers:
- Patient handling strategy before movement begins, including path planning and transition points
- Specialty equipment use such as reinforced stretchers, ramps, transfer aids, and loading systems
- Positioning and respiratory awareness because larger body habitus can change tolerance for lying flat, moving, or being secured
- Team coordination so everyone knows the sequence before the first lift or slide
This is also one of the few areas where a family can often feel the quality difference immediately. Prepared teams move deliberately. Unprepared teams improvise, reposition repeatedly, and create anxiety.
A specialized mission needs a specialized crew. If the transport plan sounds generic, the training probably is too.
A Checklist for Evaluating Transport Providers
When you're comparing providers, don't ask only, “Can you do the trip?” Most services can answer yes. Ask how they do it, who does it, and how they handle the moments where transfers usually go wrong.
The checklist below is the kind of tool I'd want in a family member's hand before they agreed to a move.
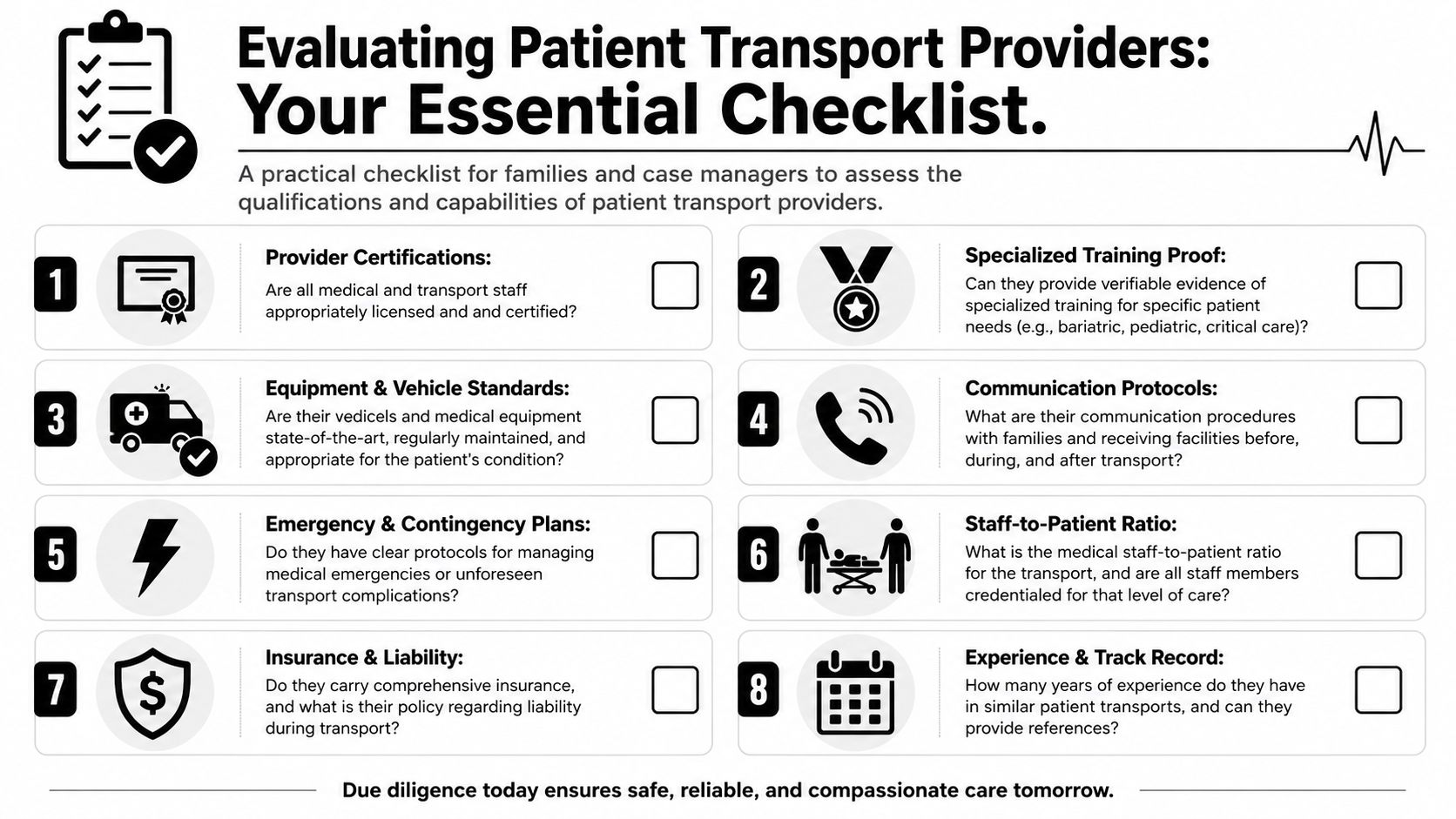
Questions worth asking on the first call
Start with the clinical side.
Crew qualifications
Ask who will be physically with the patient. Nurse, paramedic, physician, respiratory support, or escort staff. Then ask what transport-specific training they hold.Patient-specific planning
Ask how they adapt for oxygen, ventilators, infusions, obesity, infection precautions, pediatrics, or behavioral concerns.Handoff process
Ask how they receive report from the sending team and how they deliver report on arrival.
Then move into operational discipline.
Equipment readiness
Ask what monitor, oxygen, suction, stretcher, and backup systems travel with the patient.Escalation plan
Ask what happens if the patient gets worse before departure, during loading, or en route.Documentation flow
Ask who handles medical records, physician certification paperwork, and communication with the receiving facility.
What a strong answer sounds like
A good provider usually answers in sequence, not in marketing language. They describe assessment, acceptance, equipment matching, staffing, communication, transfer execution, and arrival handoff.
Here's a practical table to use.
| Category | Question to Ask | What a Good Answer Sounds Like |
|---|---|---|
| Clinical crew | Who will care for the patient during transport? | Clear roles, credentials, and why that crew matches the patient |
| Training | How is your patient transport training maintained? | Specific mention of recurrent drills, competency review, and supervised progression |
| Handoff | How do you manage report and transfer of care? | Structured communication with sending and receiving teams |
| Equipment | What equipment travels with the patient? | Patient-specific list, plus backup capability |
| Special needs | How do you handle bariatric or air medical cases? | Distinct protocols, not generic reassurance |
| Escalation | What if the patient deteriorates? | Defined response steps and authority to delay or change the mission |
| Family communication | Who updates the family during the process? | Named point of contact and clear timing expectations |
One more signal people miss
Listen for whether the provider treats the trip as a system, not a vehicle booking. That's usually the difference between a mature operation and an improvised one.
For example, Med Jets by Air Trek coordinates air ambulance transport, medical escorts, and ground segments as one transfer process rather than separate tasks. That kind of end-to-end model can be useful when a patient needs continuity across multiple legs of transport. It's one option among several, but it illustrates what integrated planning looks like.
If a provider can't explain responsibility from bedside pickup to bedside arrival, keep asking questions.
Frequently Asked Questions About Medical Transport
What's the main training difference between ground and air medical crews
Ground crews train around roadway movement, ambulance operations, loading mechanics, and patient care in a mobile but more familiar environment. Air crews still need those clinical fundamentals, but they also train for aircraft safety, tighter spaces, louder environments, flight physiology, and more complex coordination with pilots and dispatch. The patient may be the same. The care environment isn't.
Is patient transport training only about moving the patient safely
No. Safe movement is part of it, but not the whole job. Good patient transport training covers assessment, device management, monitoring, medication continuity, communication, and clinical handoff. The actual move is only one phase of a larger care process.
How can a family tell if a provider understands handoffs, not just transport
Ask them to walk you through the transfer from first report to arrival report. If they talk about identity verification, current condition, lines and drains, monitoring, and what they communicate to the receiving team, they're probably treating it as a clinical handoff. If they only talk about pickup times and vehicles, they're probably not.
Do all stable patients need the same level of transport crew
No. “Stable” can mean many different things. Some patients are stable but fragile. They may need oxygen, careful positioning, device management, or a crew that can recognize subtle deterioration. The right crew depends on the patient's condition, the distance, the mode of transport, and what could reasonably change during the trip.
How is training usually verified
Providers should be able to describe licenses, transport certifications, onboarding requirements, supervised progression, and recurrent competency checks. For more complex programs, they should also be able to explain how they document those standards internally and how they prepare crews for patient-specific missions.
Is specialized training important for bariatric patients even if the trip is short
Yes. Distance doesn't remove the handling risk. Bariatric transport often depends on route planning, transfer surfaces, loading equipment, positioning, and respiratory awareness. Short trips can still go badly if the crew improvises.
What should case managers ask that families often forget
Ask who owns the handoff. Not just who drives or flies. Who receives report, who confirms acceptance, who manages the patient's devices, who gives the arrival report, and who documents changes in condition during transport. Those questions get to the heart of transport quality.
What's a warning sign that a provider may not be the right fit
Vague answers. If the provider can't explain staffing, equipment, communication steps, or escalation plans in plain language, that's a problem. Strong teams usually make complicated work sound organized, not mysterious.
Patient transport looks simple from the hallway. It rarely is. The safest crews combine clinical judgment, disciplined communication, equipment fluency, and repeated practice under pressure. That's what makes a transport team reliable when the patient leaves the protection of the bedside and care has to keep moving.