A doctor has just said your loved one may need to move to another hospital. You're trying to listen, take notes, answer texts, and make sense of terms you didn't expect to hear today. At the same time, practical questions start piling up. Why transfer at all? Who accepts the patient? How does transport get arranged? What does insurance need? Can someone ride along?
A hospital to hospital transfer can feel chaotic from the outside, but the process is manageable when you break it into the right decisions in the right order. Families need plain language. Case managers need a working checklist. Both need the same thing most of all, which is a clear picture of what happens next.
The safest transfers usually have three things in common. The reason for transfer is well defined. The sending and receiving teams agree on the plan. One person keeps the moving parts aligned so no step gets missed.
Determining if a Hospital Transfer Is Appropriate
The first question isn't how to move the patient. It's why a transfer is being considered at all. That answer shapes everything after it, including urgency, destination, transport mode, and insurance review.
The three common reasons for transfer
Most hospital to hospital transfer decisions fall into one of these categories:
- Higher level of care: The current hospital has stabilized the patient, but the patient needs services the facility can't provide around the clock. That may mean a larger ICU, advanced cardiac support, trauma capability, transplant services, or a more specialized nursing environment.
- Access to a specific specialist or treatment: Sometimes the issue isn't the hospital overall. It's one procedure, one team, or one type of equipment not available locally. Families often hear this when a physician says, “We can continue supportive care here, but definitive treatment is at another center.”
- Repatriation or closer-to-home care: This is a planned move after the patient is stable enough to continue recovery nearer to family, a home physician, or a preferred health system. This is still a hospital to hospital transfer, but the timeline and transport decision are usually less urgent.
Those reasons are not equal in urgency. A transfer for medical necessity often has to move quickly, sometimes as soon as the receiving hospital confirms a bed and physician acceptance. A transfer for repatriation may be carefully scheduled around staffing, bed availability, and transport logistics.
Questions to ask before anyone books transport
When families feel rushed, they often skip the questions that matter most. Ask them anyway. A good medical team will expect them.
- What is the exact reason for transfer? Ask for the plain-language version, not only the diagnosis.
- Is this urgent or planned? The answer affects how much time you have to review destination options.
- What can the receiving hospital do that this hospital can't? That question often clarifies medical necessity.
- Is the patient stable enough to move right now? Stability for treatment is not always the same as stability for transport.
- What level of monitoring or life support will be needed during transport? This helps determine ground versus air and crew type.
- Has a receiving physician accepted the patient? A preferred hospital is not the same as an accepting hospital.
- Is there an available bed, and what unit will the patient go to? ICU, step-down, telemetry, and med-surg are very different transfer targets.
- If we wait, what risks increase? Families need to understand whether delay is inconvenient or dangerous.
A transfer should solve a defined care problem. If no one can explain what changes at the receiving hospital, stop and ask again.
What works and what doesn't
What works is a transfer request built around a specific clinical objective. “The patient needs neuro-interventional care not available here” is strong. “The family wants another hospital” may still be valid, but it usually requires more logistics and may not move as quickly.
What doesn't work is starting with destination preference before confirming clinical fit. Families sometimes call multiple hospitals at once, hoping one will say yes. That can create crossed records, mixed messages, and delays. In most cases, it's better to identify the most appropriate receiving facility first, then push that path forward cleanly.
For case managers, the key early task is separating urgent transfer need from desired transfer location. For families, the key is understanding that asking for clarity isn't being difficult. It's how safe transfers get organized.
Choosing Your Transport Method Ground vs Air Ambulance
Once the destination is identified and the transfer is medically appropriate, the next decision is how the patient should travel. Families often focus on speed alone at this point. In practice, the right choice depends on three things: distance, urgency, and patient acuity.
How ground and air really compare
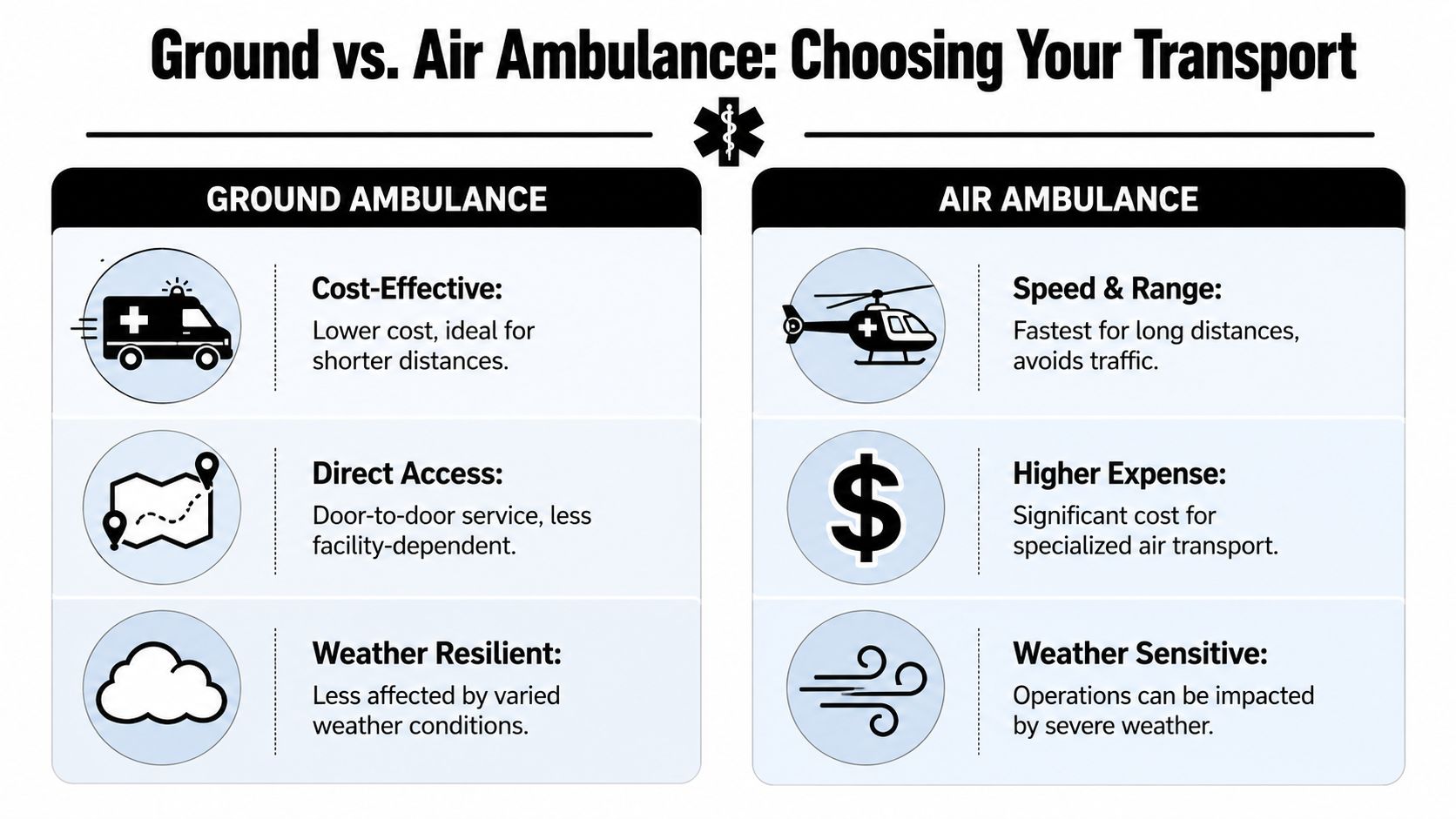
Ground ambulance is often the practical choice when the receiving hospital is close enough that road travel won't create harmful delay, and when the patient's needs can be safely managed in that vehicle. Air ambulance becomes more relevant when distance is longer, the patient needs rapid movement between facilities, or the transport team must maintain a higher level of critical care throughout the trip.
Here's the side-by-side view families and case managers usually need:
| Factor | Ground ambulance | Air ambulance |
|---|---|---|
| Best fit | Shorter regional transfers | Longer transfers or higher-acuity cases |
| Speed | Slower over distance, subject to road conditions | Faster over long distance, avoids highway delays |
| Access | Direct hospital-to-hospital by road | Usually includes ground legs on one or both ends |
| Weather impact | Usually less weather-sensitive | More likely to be delayed or adjusted for weather |
| Clinical setup | Appropriate for many monitored transfers | Strong option for ICU-level continuity in transit |
| Cost profile | Generally lower | Generally higher because of aircraft, crew, and coordination |
The clinical side of the decision
Transport isn't just a ride. It's a moving care environment.
A ground critical care unit may be appropriate for a patient on oxygen, cardiac monitoring, IV medications, or ventilator support when the route and travel time are reasonable. An air ambulance is often chosen when time matters more, when fatigue and delay from a long road trip would add risk, or when the patient needs intensive oversight during a longer move.
Families often ask what they're paying for with an air ambulance. The answer usually includes a medically configured aircraft, specialized crew, monitoring equipment, medication capability, oxygen management, and end-to-end logistics. For a simple overview of aircraft types, this guide to fixed-wing vs rotary-wing transport helps explain why jets and helicopters are used in different situations.
Rule of thumb: If the patient is stable and the trip is relatively short, ground is often the sensible choice. If the distance is substantial, urgency is higher, or the patient needs critical care continuity over a longer route, air usually deserves serious consideration.
What people often get wrong
One common mistake is assuming air is always faster door to door. It isn't always. Air transport includes dispatch, airport coordination, loading, and usually ground transport on both ends. For some regional transfers, ground may still be more efficient overall.
Another mistake is choosing based only on price or only on stress. A family may want the fastest option because the situation feels frightening, or may avoid air because it sounds expensive. Those reactions are understandable, but the right decision comes from matching the patient's condition to the transport environment.
A third mistake is ignoring comfort and access issues. Bariatric patients, patients with complex ventilator setups, and patients who decompensate with movement may require a transport team that can handle more than standard loading and monitoring. Those cases should be screened early, not after a trip is booked.
Navigating Documentation and Insurance Approvals
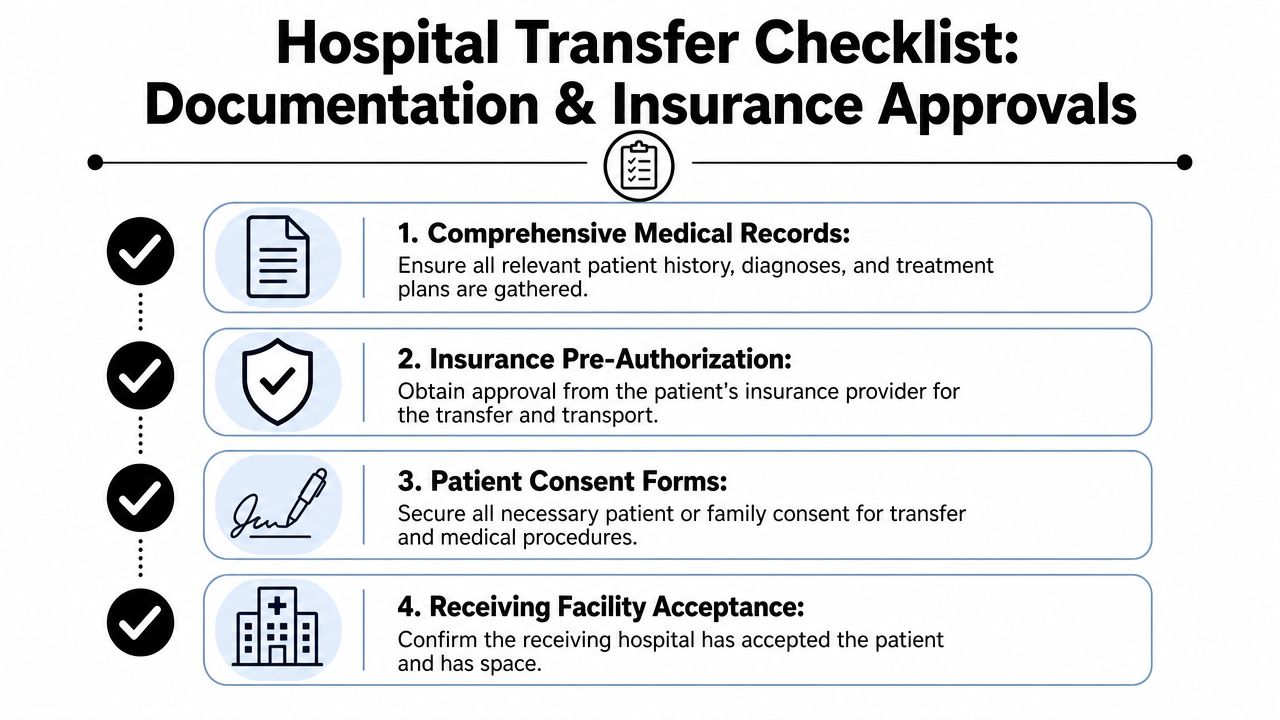
The paperwork side of a hospital to hospital transfer is where many delays begin. Most of them are preventable. The easiest way to manage the process is to sort it into three buckets: medical orders, insurance authorization, and facility agreements.
Medical orders and clinical packet
The transfer cannot move safely without a complete clinical handoff. A transport provider needs more than a diagnosis line and room number.
Gather or confirm these items first:
- Physician transfer order: The sending physician documents the need for transfer and the level of transport required.
- Current face sheet: This usually includes patient identifiers, contact details, and insurance information.
- Recent clinical summary: Diagnosis, reason for admission, current status, active problems, and why the receiving facility is needed.
- Medication list and infusions: Include anything running now, especially time-sensitive drips.
- Vital trends and nursing notes: The transport team needs to know the patient's trajectory, not just a snapshot.
- Test results and imaging access: Labs, radiology reports, and actual images if the receiving team requests them.
- Code status and consent forms: These should be clear before the patient leaves the floor.
If the patient is on a ventilator, has drains, has isolation precautions, or requires specialty devices, that information needs to be stated plainly. Don't assume it will be obvious from the chart.
Insurance approval and preauthorization
Insurance review usually turns on medical necessity, destination appropriateness, and transport mode. Families often hear “the hospital is handling it,” but it still helps to know what to ask.
Use this checklist with the case manager and insurer:
- Ask whether prior authorization is required: Some transfers move under urgent clinical review, while others need formal approval before transport can be scheduled. This overview of medical transport prior authorization is a useful starting point.
- Confirm what part of the transfer is covered: Hospital stay, transport, and ground legs may be handled differently.
- Ask if bed-to-bed coverage is included: Families often assume the policy covers the whole journey when it may only cover one segment.
- Clarify in-network and out-of-network issues: The receiving hospital may be covered differently from the sending hospital.
- Find out who submits the clinical justification: It may be the sending hospital, receiving hospital, transport provider, or a combination.
- Request the authorization reference and reviewer contact: If anything stalls, that information matters.
When approval is delayed, the usual cause isn't “insurance being impossible.” It's that the clinical reason, accepting physician, destination, or transport level hasn't been documented clearly enough.
Facility acceptance and transfer agreements
A hospital to hospital transfer doesn't happen just because a family wants one or a doctor suggests one. The receiving facility must formally accept the patient.
That generally means:
- An accepting physician agrees to take over care
- A bed or unit placement is identified
- The sending hospital forwards the required records
- Both sides agree on timing and transport readiness
You may also hear EMTALA mentioned. In simple terms, EMTALA is the federal framework that requires emergency evaluation and stabilizing treatment and guides appropriate emergency transfers. For families, the practical takeaway is this: hospitals cannot treat transfer as a casual discharge. There must be a medically appropriate handoff.
What works here is one person tracking each approval point in real time. What doesn't work is assuming the chart “has everything” while three different departments are waiting on one unsigned form.
The Coordination Workflow from Start to Finish
On transfer day, the smoothest cases don't look dramatic. They look organized. Phone calls are shorter because the right information is already in place. The bedside nurse knows what time the crew is coming. The receiving unit is expecting the patient. The family knows where to go and who to call.
What a typical transfer day looks like
The day usually starts with a transfer request from the sending hospital, case manager, insurer, or family. A coordinator gathers the patient's current condition, destination request, and urgency. That's the moment when the process either becomes orderly or fragmented.
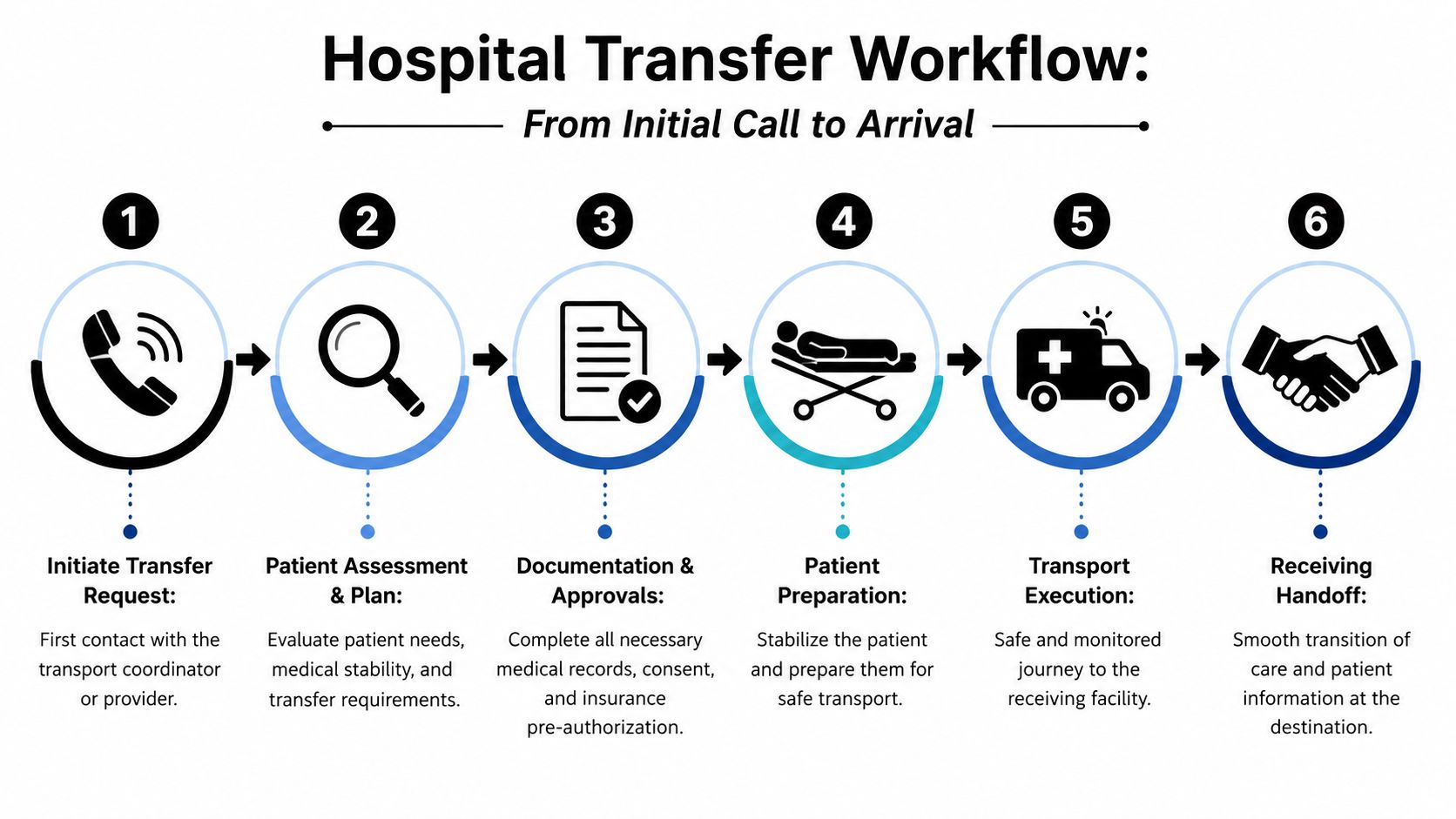
Once the basics are confirmed, the coordinator lines up the clinical review, transport plan, and communications chain. In many programs, the flight or transport coordinator becomes the single point of contact. That matters more than families realize. Without one lead person, updates can split across nursing, dispatch, admissions, and insurance calls.
Teams that want a more formal process map often borrow ideas from incident management tools. For example, Resgrid workflow features show how structured workflows help teams assign steps, track approvals, and avoid missed handoffs. The same principle applies in medical transport, even if hospitals use a different platform.
The handoffs that matter most
There are several points where a transfer can go wrong if communication is weak:
- Sending physician to receiving physician: This confirms the clinical reason for transfer and acceptance.
- Case manager to insurer and transport coordinator: This keeps approvals and timing aligned.
- Bedside nurse to transport crew: This is where current status, drips, lines, recent changes, and special precautions are clarified.
- Transport crew to receiving team: This final report closes the loop and protects continuity of care.
A provider handling the full transport chain, including air and ground coordination, can reduce these handoff gaps. One example is Med Jets by Air Trek, which coordinates hospital departure, aircraft transport, and receiving-side logistics as part of a bed-to-bed transfer workflow.
Here's a useful overview of why that continuity matters in patient continuity of care during transport.
The safest transfer is the one where everyone knows who owns the next step.
What the family should expect during movement
A family often sees only the loading part, but several clinical checks happen around it. The transport team reviews the chart, confirms equipment compatibility, checks oxygen and medication needs, and reassesses the patient before leaving the room. If the patient isn't stable enough at that moment, the departure time may change. That's frustrating, but it's often the right call.
This short video gives a basic visual sense of medical flight operations.
During the trip, the crew manages monitoring, medication administration within protocol, airway support if applicable, and communication with destination contacts. On arrival, the handoff should happen at bedside or as close to bedside as the receiving facility allows. The receiving team needs the transport summary, not just the sending hospital chart, because the patient's status may have changed in transit.
What works is predictability. What doesn't work is assuming silence means nothing is happening. Much of the actual coordination occurs before the wheels move.
Special Considerations for Complex Patient Transfers
Some patients fit standard transfer pathways. Others don't. Complex transfers require different equipment, different staffing, and sometimes a different aircraft or routing plan. If a case involves bariatric needs, neonatal or pediatric care, or international movement, the details matter early.
Bariatric transfers
Bariatric hospital to hospital transfer planning goes far beyond asking for a larger stretcher. The team may need reinforced loading systems, wider access points, additional personnel for safe movement, and an aircraft cabin configuration that can physically accommodate the patient and medical equipment.
The transport decision also involves weight and balance planning, which affects aircraft selection and onboard layout. That's why the right question isn't “Can you take a bariatric patient?” It's “What exact equipment and aircraft setup will you use for this patient's size, mobility, and medical condition?”
Key screening points include:
- Room-to-vehicle movement: Can the sending hospital safely move the patient to the transport stretcher?
- Doorway and elevator access: Problems often start before the patient reaches the ambulance.
- Pressure injury protection: Longer movement times increase skin and positioning concerns.
- Crew lifting limits and transfer aids: This should be planned, not improvised.
Pediatric and neonatal transfers
Children are not small adults, and neonatal transfers are their own specialty. A premature infant, a child with congenital heart disease, or a pediatric respiratory patient may need a team with neonatal or pediatric-specific training, rather than a general critical care crew.
The equipment differs too. Depending on the case, transport may require an isolette, pediatric ventilator settings, age-appropriate airway tools, medication dosing support, and a neonatal nurse or respiratory therapist. For families, one of the most important questions is simple: Who exactly will be on the team, and do they routinely transport patients in this age group?
A specialized patient needs a specialized transport plan. General capability isn't always enough.
What works in pediatric transfers is narrowing the plan to the child's actual condition. A baby needing thermal control and respiratory support has a very different transport profile from a school-age child moving for orthopedic care.
International transfers
International transfers add a layer of nonclinical coordination that families often underestimate. Even when the patient is medically stable enough to travel, the case may still hinge on passport issues, customs procedures, airport permissions, language barriers, receiving-country admissions, and timing with foreign medical teams.
The transport coordinator may need to align:
- Medical records across systems and languages
- Customs and immigration paperwork
- Airport handling and ground ambulance at both ends
- Medication and equipment compliance for cross-border travel
- Communication with consulates, assistance companies, or travel insurers
International cases also demand realistic timing. Families sometimes expect them to move like domestic transfers. They usually don't. Even when the aircraft is available, bedside readiness and border coordination still have to line up. The safest international transfers are deliberate, not rushed.
Frequently Asked Questions About Patient Transfers
Can a family member travel with the patient?
Often, yes, but it depends on the patient's condition, the aircraft or vehicle configuration, safety limits, and crew judgment on the day of transport.
If the patient requires intensive intervention space, the crew may need every inch around the stretcher. In more stable cases, one family member may be allowed to accompany the patient. Ask this early, but understand that final approval can change if the clinical situation changes.
What personal items can the patient bring?
Keep it minimal. Bring essentials only.
Good choices usually include identification, insurance cards, eyeglasses, hearing aids, dentures, a phone and charger, and a small bag of necessary comfort items. Leave valuables, bulky luggage, and anything fragile with family if possible. Transport crews need a clean, safe treatment area, and loose items can create problems during loading and unloading.
Who arranges the ground ambulance on each end?
Usually the transport coordinator or arranging provider handles it, but you should never assume. Ask directly, “Who is booking the sending-side ground leg and the receiving-side ground leg?”
In air transfers especially, the patient may need ambulance movement from hospital to airport and then airport to receiving hospital. If nobody owns those segments clearly, you can end up with an aircraft waiting on one side and no ambulance on the other.
What happens if the weather is bad on the day of the flight?
Weather can delay or alter air transport plans. Safety decisions are made by the flight operation, not by scheduling pressure.
That may mean a later departure, a different airport, a switch in routing, or in some cases a recommendation to use ground transport instead. Families often worry that a delay means the case has been forgotten. Usually it means the team is protecting the patient and crew from an avoidable risk.
Bad weather doesn't automatically cancel a transfer. It changes the plan until the plan is safe.
How is medical care managed during the flight or ride?
The transport team provides ongoing monitoring and care appropriate to the patient's condition and the service level booked. That can include oxygen therapy, cardiac monitoring, suction, medication administration within protocol, ventilator support, and reassessment throughout the trip.
The key point is that the patient is not “just being moved.” The crew is maintaining continuity of care during a vulnerable transition. If the patient's status changes, the transport team responds and updates the receiving facility as needed.
Can the patient be transferred for a second opinion?
Yes, in some cases, but a second opinion and a transfer are not the same thing. A hospital can often send records for outside review without physically moving the patient.
A full hospital to hospital transfer usually makes more sense when the outside team recommends treatment that the current hospital can't provide, or when the patient needs to be under the care of that receiving team directly. Families should ask whether records review alone is enough or whether the treatment plan requires relocation.
What if the receiving hospital says yes, but there's no bed yet?
Then the transfer is not ready to move. Physician acceptance is only one part of receiving-side readiness.
The patient also needs placement in an appropriate unit. Sometimes a transfer can be approved clinically but delayed operationally because the destination is still arranging ICU, telemetry, or specialty bed space. That's frustrating, but it's common and it's better than arriving without a safe handoff location.
Can we choose any hospital we want?
Not always. Preference matters, but clinical appropriateness, physician acceptance, service availability, and insurance constraints all affect the final destination.
If your preferred hospital cannot provide something the patient needs, can't accept the patient, or has no bed, the team may need to choose a different facility. When there's flexibility, families should still ask whether the destination aligns with the patient's likely next phase of care, not just today's emergency.
How long does a hospital to hospital transfer take?
There's no universal answer because several steps have to line up. The timeline depends on patient stability, physician acceptance, bed availability, records transfer, insurance review if required, and transport readiness.
Some urgent transfers move quickly once the medical need is clear. Others take longer because one missing approval or one unavailable bed holds the entire chain. The best question isn't “How long does it usually take?” It's “Which step are we waiting on right now?”
What should families do while the team is arranging the transfer?
Focus on the few actions that help.
- Choose one main family contact: That prevents repeated calls to the nursing station.
- Keep your phone available: Coordinators and case managers often need quick answers.
- Write down names and roles: Sending physician, case manager, receiving hospital contact, and transport coordinator.
- Ask for the current status in one sentence: For example, “We are waiting for bed assignment,” or “Insurance review is pending.”
- Prepare a small essentials bag: Not a suitcase.
- Clarify where you should go: Some families need to travel separately and meet at the receiving hospital.
What doesn't help is having several relatives each call different departments for updates. That creates confusion at exactly the wrong time.
What if the patient gets worse before departure?
Then the plan may change. The team may delay departure for stabilization, upgrade the transport level, change from ground to air, or in some cases change the destination to the nearest appropriate higher-acuity center.
That isn't a failure of the process. It's the process doing what it should do, which is adjusting to the patient rather than forcing the patient into a plan that no longer fits.
Is a hospital to hospital transfer ever optional?
Sometimes yes, sometimes no. A repatriation transfer closer to home may be elective in timing. A transfer for stroke intervention, specialized cardiac care, burn treatment, neonatal support, or advanced ICU management may be medically necessary and time-sensitive.
If you're unsure which kind of transfer you're dealing with, ask the attending physician this exact question: “If we don't transfer today, what care will the patient not receive here?” That usually gets you the clearest answer in the room.
A well-run hospital to hospital transfer doesn't depend on luck. It depends on clear medical reasoning, complete documentation, confirmed acceptance, and tight coordination from bed to bed. Families don't need to know every clinical detail, but they do need to know what question to ask next. Case managers don't need a sales pitch. They need a process that holds together under pressure.
If you're arranging a transfer now, slow the situation down just enough to identify the primary reason for the move, the right destination, and the person managing the chain. Once those are clear, the rest of the process becomes much easier to handle.
If you need help evaluating air medical transport options, coordinating documents, or understanding what a bed-to-bed transfer involves, Med Jets by Air Trek can be reached through the Med Jets website.