A hospital calls and says your loved one needs to move today. The receiving facility is ready. The medical records are in order. Then the transfer stalls on a detail most families never expect to hear: the patient is too large for a standard air ambulance setup.
That moment is frightening because it sounds personal, but it isn't. It's usually a problem of aircraft dimensions, loading systems, stretcher limits, and safe handoff planning. A bariatric air ambulance isn't just a regular medical flight with extra room. It's a transport built around different operational limits from the first phone call to the final bedside handoff.
Families and case managers often start with the wrong question. They ask, “Who can fly the patient?” The better question is, “Who can move this patient safely through every step of the mission without a failed transfer, last-minute refusal, or avoidable delay?” That means asking about door width, stretcher compatibility, ground ambulance capability, powered loading, crew handling plans, and what happens if the patient's condition changes during transport.
The Urgent Need for Specialized Air Medical Transport
A common scenario looks like this. A discharge planner has finally secured an accepting hospital. The patient needs ongoing care, can't tolerate a routine travel option, and needs a medical flight. Then someone asks for weight, body width, and mobility status, and the room goes quiet because no one gathered those details early.
That's when coordination either gets sharper or starts breaking down.
A bariatric transfer becomes urgent because the patient still needs clinical care on the same timeline as anyone else. What changes is the transport method. The wrong aircraft can create a failed loading attempt. The wrong ground team can turn a smooth hospital exit into a dangerous lift. The wrong assumptions can cost hours.
Why this is showing up more often
The need for specialized air transport sits inside a larger growth trend in medical aviation. The global air ambulance services market is projected to grow from US$17.76 billion in 2022 to US$50.43 billion by 2032, with a projected compound annual growth rate of 11%, according to Fact.MR's air ambulance services market analysis. That broader expansion matters because bariatric transports depend on the same specialized aircraft access, crew coordination, and clinical infrastructure.
In real life, that means more families, hospitals, insurers, and assistance companies are trying to solve complex transports quickly, often across long distances and with little margin for error.
Time pressure changes every transport decision. For a bariatric patient, speed still matters, but the safe answer is the one that works from bedside to bedside.
If the transfer is clinically time-sensitive, the concept of the medical golden hour in patient transport becomes more than a phrase. It reminds families and case managers that delays don't just happen in the air. They happen during acceptance, loading, airport handling, and arrival planning.
The emotional part families feel first
Families usually hear “special equipment required” and think the case has become impossible or unaffordable. That isn't necessarily true. It does mean the mission needs more exact screening at the start.
Ask early. Be direct. If the provider sounds vague about dimensions, loading equipment, or ground arrangements, keep asking until the answer is concrete.
What Makes an Air Ambulance Bariatric-Capable
The easiest way to understand this is to compare it to moving heavy medical equipment through a house. If the equipment fits the room but not the doorway, the move fails before it starts. A bariatric air ambulance works the same way. Clinical need may justify the flight, but the mission still has to pass through doors, ramps, stretchers, mounts, and cabin space.
It starts with the aircraft, not the marketing
A provider can advertise bariatric capability, but what matters is the actual setup assigned to your case. The aircraft must physically accept the patient, the stretcher system, the medical team, and any required devices without compromising safe loading or in-flight care.
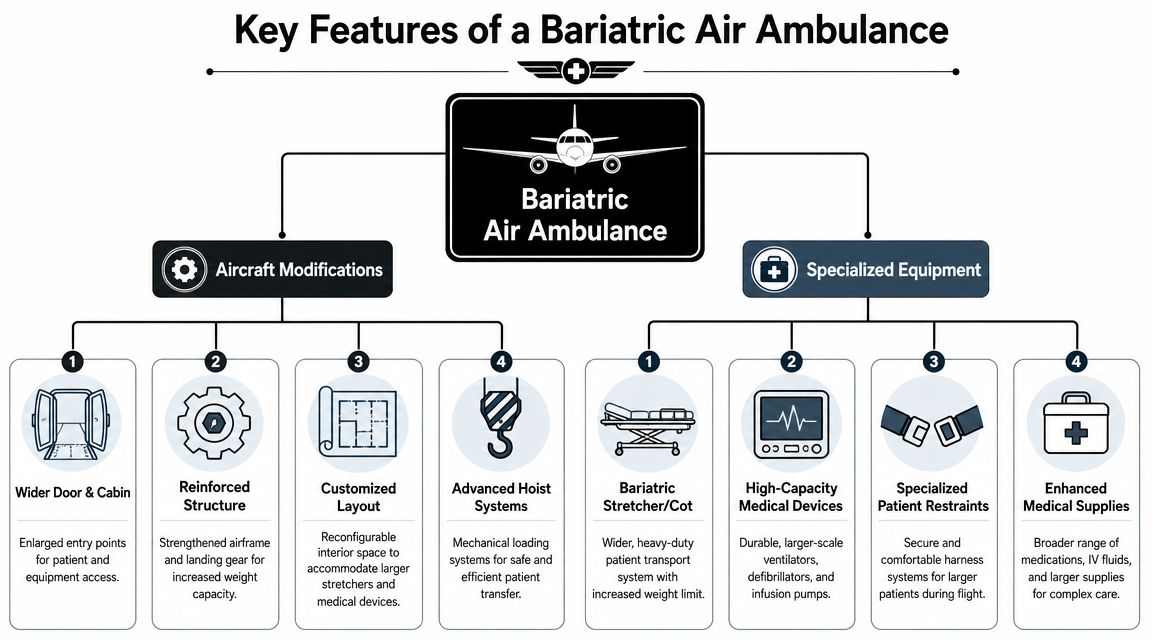
Key elements usually include:
- Wider access points so the patient and stretcher can enter without unsafe repositioning
- A cabin layout that can accommodate a larger patient footprint while preserving clinician access
- A stretcher and restraint system designed for bariatric use rather than a standard cot pushed to its limit
- A loading method that reduces manual lifting, especially at the aircraft threshold
- Ground segments that match the flight setup, because the transfer often fails before takeoff, not after
Equipment compatibility matters more than labels
The phrase “bariatric capable” should trigger follow-up questions, not relief. Ask whether the stretcher mounts are fixed and compatible with the aircraft interior. Ask whether powered loading equipment is available. Ask whether the patient can remain on one system from hospital departure through airport transfer, or whether a switch is required.
That last point matters. Every extra transfer point adds friction, time, and handling risk.
Practical rule: If a provider can't explain exactly how the patient gets from hospital bed to aircraft stretcher to receiving facility, they haven't solved the mission yet.
What families often miss
Families tend to focus on flight comfort. Case managers often focus on hospital acceptance. Coordinators focus on the whole chain. That's the right lens.
Questions people often ask include:
- Does a bigger patient always need a helicopter? No. The answer depends on distance, loading conditions, dimensions, and the available aircraft.
- Can a standard air ambulance just add extra staff? More staff doesn't solve a door-width or stretcher-mount problem.
- If the patient is medically stable, can equipment limits be relaxed? No. Physical limits stay physical limits.
- Does “bariatric” only refer to weight? No. Width, girth, mobility, transfer tolerance, and pressure-point management all affect planning.
A bariatric air ambulance is really a systems question. Aircraft, stretcher, crew, loading, and ground support all have to work together. If one piece doesn't fit, the mission doesn't fit.
Core Clinical and Operational Requirements
Clinical suitability gets most of the attention, but physics often decides feasibility first. That's why experienced coordinators ask for exact measurements before discussing schedules.

According to REVA's bariatric patient transport guidance, many fixed-wing air ambulances have a door opening of about 27 inches and can transport patients weighing 350 to 400 pounds. The same guidance notes that bariatric missions may require aircraft with larger doors and higher capacities, sometimes up to 700 pounds, along with dedicated ground support and powered loading equipment. Those aren't preferences. They're operational boundaries.
The measurements that decide everything
A safe booking usually depends on getting these details right the first time:
- Patient weight
- Patient width and girth at the widest point
- Ability to self-assist with turns or transfers
- Need for oxygen, monitoring, infusion support, or ventilation
- Pressure injury risk and positioning tolerance
- Whether the patient can tolerate a flat, semi-Fowler's, or other transport position
If any of those are guessed, the mission can unravel late.
Why crew skill changes the outcome
Bariatric transport isn't just about having extra hands. The crew has to know how to move a patient without creating shear injury, line dislodgement, respiratory compromise, or panic during loading. The medical team also needs enough cabin access to assess airway, circulation, comfort, monitoring, and device function throughout the flight.
That's one reason many case managers ask detailed questions about onboard supplies and device readiness before confirming the mission. The provider's aero medical supplies and transport equipment should align with the patient's actual needs, not a generic critical care checklist.
A patient can be medically appropriate for air transfer and still be operationally unsafe for a specific aircraft.
The real trade-offs
Sometimes a helicopter solves an access problem but not a range problem. Sometimes a fixed-wing aircraft can handle the route but not the cabin entry. Sometimes the aircraft works, but the sending facility can't support a safe extraction from the room to the ambulance bay.
That's why a sound plan answers all three questions at once:
- Can the patient be loaded safely?
- Can the patient be cared for continuously in flight?
- Can the patient be transferred again on arrival without improvisation?
If any answer is uncertain, the case needs more planning before wheels up.
Arranging a Bariatric Air Ambulance Step by Step
A bariatric transfer can look ready at 10:00 a.m. and still stall at 2:00 p.m. because one person never confirmed door width, stretcher limits, or who is responsible for the ground segment. The family hears “the flight is arranged.” The coordinator knows the case is only arranged when every handoff has been tested on paper first.
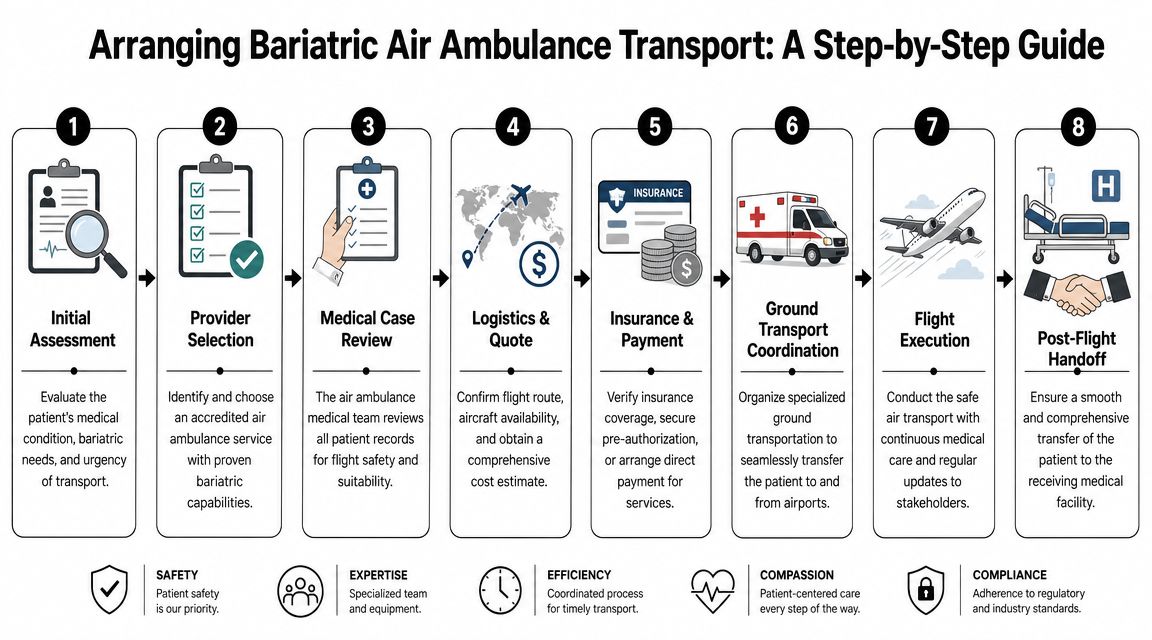
Step 1 through Step 3
Start with a complete intake
The first call should cover the sending facility, receiving facility, diagnosis, current condition, mobility status, respiratory support, active devices, and exact patient measurements. Ask for what is known now, and identify what still needs to be verified. Weight alone does not clear a case. Width, girth, transfer tolerance, and positioning limits often decide whether the plan will work.
Confirm acceptance at the destination
Get the name of the accepting physician or service, the level of care arranged on arrival, and whether the bed is assigned. Families and case managers should ask one practical question early: if the aircraft lands tonight, can the receiving team take the patient tonight?
Have the records reviewed by the transport team
The medical review needs current notes, medication lists, recent vital trends, oxygen needs, wound concerns, and anything that affects loading or in-flight care. “Stable” is too broad to build a mission around. The transport physician or clinical lead needs to know whether the patient can tolerate movement, supine positioning if required, altitude changes, and the time needed for each transfer segment.
Step 4 through Step 6
Match the transport platform to the actual case
Aircraft selection comes after case review, not before it. Ask which aircraft are being screened and why they are suitable for this patient's size, clinical needs, route, and loading method. A useful question here is, “What is the limiting factor on this case?” Sometimes it is cabin access. Sometimes it is range. Sometimes it is the ground interface at one end.
Build the ground plan on both sides
Confirm whether bariatric-capable ground ambulances are required at departure, arrival, or both. Then confirm who is booking them, what stretcher system they use, whether it matches the air segment, and whether extra personnel or powered loading equipment are required. A case can be airworthy and still fail because the airport transfer vehicle cannot complete the handoff safely.
Map the bedside path before launch
This is the step families and new case managers often miss. Ask the sending unit how the patient gets from the room to the ambulance. Ask about hallway clearance, elevator size, turns, ramps, bed height, and whether there are any points where the patient must be transferred to a different surface. Do the same at the receiving end.
Strong coordination starts with the route inside the building, not just the route in the air.
Step 7 and Step 8
- Lock down payment, authorization, and scope
Before wheels up, confirm who is financially responsible, whether insurance authorization is in place, and what the quote includes. Ask directly whether the price covers the air segment only or the full chain of care, including both ground transports, extra staffing, and airport handling if needed. Unclear wording often results in last-minute delays.
Prepare the family and both hospital teams
Set expectations for timing, updates, and what can change on the day of transport. Sending staff should know which records, medications, images, and bedside reports must travel with the patient. Receiving staff should have the ETA, current clinical status, and any special handling instructions before the aircraft departs.
Questions to ask during the first call
Use these questions to find weak points early:
- What exact measurements do you need to confirm fit and loading safety?
- Who is reviewing the chart for medical clearance and transport risk?
- Which part of this case is still unconfirmed right now?
- Will the patient need bariatric-capable ground transport on one end or both?
- How many surface transfers are planned from bedside to bedside?
- Do you have powered loading equipment available for this mission?
- What could stop this case after we think it is booked?
- Who is responsible for coordinating each handoff point?
One practical note about provider selection
Some operators and programs offer bariatric-specific capability within a broader air ambulance service. Med Jets' bariatric patient air ambulance service is one example. The point to verify is not branding. It is whether one team is managing the case from bedside pickup through arrival, with clear ownership of the air plan, the ground plan, and the clinical review.
Well-run bariatric transports feel disciplined before the patient ever leaves the room. Disorganized ones usually reveal themselves in the first few phone calls.
Navigating Costs and Insurance Coverage
The first cost question families ask is usually, “How much is this going to be?” The more useful question is, “What exactly is included, and what extra services does this patient require?”
Bariatric air ambulance pricing isn't driven by one factor. It's built from the route, aircraft selection, crew needs, ground coordination, timing, and handling complexity. A quote can look reasonable until someone realizes it doesn't include the specialized ground ambulances or airport transfer support.
What usually shapes the total price
Here are the main cost drivers to ask about:
- Aircraft type because not every aircraft that can do a medical flight can do this specific one
- Distance and routing because repositioning, airport choice, and range affect logistics
- Clinical level of care if the patient needs monitoring, oxygen, or more advanced support
- Ground transport on both ends especially if bariatric-capable vehicles are required
- Loading complexity when powered systems, extra coordination, or special access planning are needed
- Timing if the mission must launch on short notice or after-hours coordination is involved
How insurance usually enters the process
Coverage decisions often turn on medical necessity and plan language. That means the family or case manager should never assume that “air ambulance” automatically means “covered,” or that approval for a transfer means approval for the exact aircraft and equipment the patient needs.
Ask the insurer these questions directly:
- Is the transport covered as medically necessary?
- Does the plan distinguish emergency transfer from repatriation or non-emergency transfer?
- Is pre-authorization required?
- Are the ground ambulances included?
- Is the patient's bariatric requirement treated as part of the medically necessary transport setup?
If the insurer won't answer quickly, keep documenting every conversation. Names, times, and reference numbers matter.
A clear quote should identify the air segment, both ground segments, medical crew level, and any known operational add-ons.
How to avoid expensive surprises
The best quotes are specific. If a provider uses general language such as “special handling may apply,” ask them to translate that into a line-item explanation before you commit.
A good financial checklist includes:
- Who pays if the aircraft is booked but the patient is refused at loading?
- What happens if ground transport arrives and can't complete the handoff?
- Are airport fees, positioning, and coordination already included?
- Will the family receive one invoice or several from different vendors?
If you're paying privately, ask whether the provider offers direct coordination with hospitals and insurers to reduce administrative delays. Even when coverage is uncertain, a tightly managed authorization process often prevents costly last-minute scrambling.
Evaluating Provider Safety and Asking the Right Questions
A bariatric mission is not the time to shop by headline claims. You're trusting a provider to manage patient safety through aircraft selection, clinical care, loading, documentation, and handoff. That requires due diligence.
One of the clearest standards-based questions comes from GAMA Aviation's guidance on transporting bariatric patients by air ambulance. It notes that EURAMI standards require providers to define weight and dimensional limits beyond which a bariatric patient will be refused, and that case managers should request the aircraft's maximum patient weight, door opening dimensions, and stretcher compatibility before booking. That single point separates serious planning from sales talk.
What to ask before you authorize anything
Look for precise answers, not reassurance.
| Question to Ask | Why It Matters |
|---|---|
| What is the maximum patient weight for the aircraft assigned to this case? | It confirms the mission is being matched to a real airframe, not a generic fleet claim. |
| What door opening dimensions apply to this specific aircraft? | A patient can be clinically stable and still physically unable to enter safely. |
| What stretcher system will you use, and is it compatible from ground to air? | Mismatched systems create extra transfers and risk. |
| What patient dimensions would cause you to refuse the case? | Reputable providers define refusal thresholds in advance. |
| Is powered loading equipment available? | It reduces manual handling and lowers the chance of an unsafe lift. |
| Who is responsible for the ground ambulance on each end? | Split responsibility often creates handoff failures. |
| What training does the clinical crew have for bariatric handling? | Technique matters as much as staffing numbers. |
| What happens if the patient's status or measurements differ at bedside? | You need to know whether the provider has a contingency plan or will cancel. |
Accreditation and operational maturity
Accreditation matters because it signals that a provider has submitted its systems to outside review. Families also benefit from asking whether the provider operates the aircraft directly or brokers the case to others. That doesn't automatically make one model unsafe, but it changes who controls quality, communication, and accountability.
If you're reviewing operational risk more broadly, it can help to understand the kind of pilot safety features used in aviation systems that support disciplined flight operations. Clinical safety and flight safety are connected. A weak operation on one side often shows up on the other.
Ask the provider to describe the failure points they plan around. The answer tells you more than a polished brochure ever will.
Why Trust Med Jets by Air Trek for Your Transport
At the point of booking, families usually focus on availability and price. The safer question is who will still be in control when the case gets complicated at bedside, on the ramp, or during a delayed handoff after landing.
That is the practical reason to look closely at Med Jets by Air Trek. The program has been operating since 1978 and handles coordination, flight operations, medical staffing, and ground planning under one chain of communication. In bariatric transport, that matters because the case can fail in small gaps. A stretcher clearance missed by an inch, a ground unit that arrives without the right loading system, or a receiving facility that is not ready can stop a transfer fast.
Its fleet includes Cessna Citation II, III, and V aircraft configured for patient transport and family accompaniment. For a bariatric case, the aircraft type is only part of the answer. The better question is whether the assigned aircraft, loading process, clinical crew, and ground segments have all been confirmed for this specific patient before the launch decision is made.
I tell families and case managers to listen for clear operational answers. Who takes responsibility for verifying dimensions and weight. What happens if bedside measurements differ from the referral. Whether the provider is arranging both ground legs or handing that off. How the crew plans the transfer if the patient cannot tolerate extra repositioning. A provider that can answer those points without vague language is usually showing you how it runs the mission.
Med Jets by Air Trek provides a direct overview of its bariatric patient air ambulance service and can be reached 24/7 at 1-800-MED-JETS.
Trust in this setting is not about branding. It comes from disciplined planning, clear limits, and one team owning the case from the first call to the final handoff. If you are arranging transport now, have the patient's current height, weight, body width, medical summary, facility contacts, and insurance details ready before you call. That usually prevents the first round of delays.