A hospital room far from home changes the timeline fast. One person is talking to the nurse, another is calling siblings, and someone is asking whether a flight can be arranged today. At the same time, the essential questions are more specific. Is the patient stable enough to travel? Who signs off on that? Which receiving facility is expecting them? Can a spouse ride along, and what happens to the medications, luggage, wheelchair, or the dog that still needs a plan at home?
People searching for fly u home are usually dealing with an active discharge problem, not doing casual research. They need clear answers, a realistic transport plan, and someone who can coordinate with the hospital case manager, the sending physician, the receiving team, and the ground crews on both ends.
Bedside-to-bedside sounds straightforward, but families often learn too late that the phrase can mean very different levels of help. In practice, it should cover more than the aircraft. It should include the medical review, records collection, fit-to-fly decision, airport logistics, ambulance transfers if needed, and a clean handoff after landing. It should also account for the people around the patient. Family escorts, mobility limits, personal items, and pets are not small details when a household is trying to regroup.
The process gets easier once the right pieces are lined up. The hard part is knowing which details affect safety, timing, and cost before the first booking is made.
Your Guide to Bringing a Loved One Home
A common version of this call starts the same way. A daughter is standing in a hallway outside a nursing station. Her father had a medical event while traveling. The hospital has stabilized him, but his doctors are far away, the family is exhausted, and everyone is asking the same question in different words. How do we fly him home safely?
That's the right question.
The answer usually isn't “book the first plane.” It's “match the transport to the patient, then build the move around the medicine.” A good fly u home plan starts with medical stability, not urgency alone. Families often feel pressure to act immediately, but the safest moves come from a clear sequence.
What families need most at the start
Three things are needed right away:
- A clinical answer: Is the patient stable for non-emergent transport, or do they need a higher level of care in the air?
- A logistics answer: Which hospital will accept the patient, and who is coordinating ground transport on both ends?
- A human answer: Can family go along, and what happens to personal items, medications, and pets?
Practical rule: The best first call is the one that combines medical review with transport planning, not just flight booking.
Programs built around hospital-to-hospital repatriation have made this process more standardized over time. For example, AirMedCare Network's Fly-U-Home program describes bedside-to-bedside transport for members hospitalized more than 150 nautical miles from home, with coordination through a dedicated logistics center and coverage extending across the contiguous United States, Alaska, Hawaii, and internationally in 250 cities across 150 countries through its broader program offerings, according to the Fly-U-Home program overview.
That matters because it gives families a useful benchmark for what organized repatriation should look like. One call should trigger physician review, transport planning, bed confirmation, and movement from sending bedside to receiving bedside. If you're not getting that level of coordination, expect delays, confusion, or both.
First Decision Air Ambulance or Commercial Escort
A daughter gets the call everyone dreads. Her father is ready to leave the hospital out of state, but "ready to travel" does not answer the question she needs answered. Can he get through an airport, sit upright for hours, tolerate delays, and still arrive in good shape? Or does he need a medical aircraft with a crew prepared to treat changes in condition in the air?
That first decision is clinical, and it drives everything that follows.
If the patient needs continuous monitoring, stretcher transport, oxygen that must be managed closely, suction, medication support, or a cabin arranged around medical equipment, an air ambulance is usually the safer choice. If the patient is stable, can tolerate the physical demands of a commercial trip, and only needs a qualified medical professional to accompany them, a commercial medical escort may be enough. The wrong call can lead to airline denials at the airport, discharge delays, or a rushed rebooking after the patient has already been moved.
Air Ambulance vs. Commercial Medical Escort
| Feature | Air Ambulance (e.g., Med Jets by Air Trek) | Commercial Medical Escort |
|---|---|---|
| Clinical capability | High-acuity environment with medical equipment and dedicated clinical crew | Limited to what can be managed safely on a commercial flight |
| Patient stability needed | For patients who may need monitoring, oxygen, stretcher setup, or advanced support | For stable patients who can tolerate airport movement and airline conditions |
| Departure flexibility | Scheduled around the patient and receiving facility | Dependent on airline schedules, airport processes, and seat availability |
| Airport exposure | Minimal for the patient because transfers are tightly coordinated | More exposure to terminals, delays, security, and public spaces |
| Family accommodation | May allow family depending on aircraft configuration and safety limits | Usually easier for accompanying relatives to book separate seats |
| Best fit | Hospital-to-hospital transfer for medically fragile patients | Lower-acuity travel when the patient can handle commercial transport |
Families often get tripped up by the word "stable." A bedside team may mean the patient is no longer in immediate crisis. A flight coordinator has to answer a narrower question. Stable for which transport method.
A patient may be stable in a hospital bed and still be a poor candidate for commercial travel. The trouble points are rarely abstract. Can the patient sit up for boarding and taxi. Can they make it through security without distress. Are they at risk if a flight is delayed on the tarmac. Will pain, confusion, weakness, or oxygen needs get worse during connections and terminal transfers. Those details decide the mode of transport more than the diagnosis name alone.
When an air ambulance is the safer choice
A private medical aircraft makes sense when the transfer itself requires clinical control. This often applies to patients coming from ICU or step-down units, patients who cannot stay seated for the trip, and patients whose oxygen, medication, airway, positioning, or monitoring needs could change en route.
It also solves logistical problems that families do not always see at first. Hospital discharge may be timed around a receiving facility's admission window. Ground ambulances may be needed on both ends. A spouse may want to ride along. A service animal or family pet may need separate planning. Bedside-to-bedside service sounds simple, but in practice it means one team is coordinating the sending floor, ground pickup, aircraft loading, receiving bed, and final handoff so the patient is not left waiting in the wrong place at the wrong time.
Aircraft type can matter too. The difference between helicopter and jet transport affects range, airport access, and how the hospital transfer is set up. This guide to fixed-wing vs. rotary-wing medical transport helps explain why a case manager may recommend a fixed-wing aircraft for a longer repatriation.
When a commercial escort can work
A commercial medical escort can be a good fit for the right patient. The patient needs to be medically steady enough for a public travel environment and physically able to tolerate check-in, boarding, possible delays, cabin pressure changes, and the lack of privacy and flexibility that come with airline travel.
There are trade-offs. Commercial escort trips can cost less, and some families prefer the familiarity of a scheduled airline. But the schedule belongs to the airline, not the patient. If the hospital discharge runs late, weather shifts, or the patient declines at the airport, the plan can unravel fast.
One question helps cut through a lot of confusion. Ask the treating team and the transport coordinator, "Is this patient safe for commercial airline travel, or only safe with a medical aircraft and clinical crew?" That wording usually gets a clearer answer than asking whether the patient is stable enough to travel.
Gathering Critical Information Before You Call
A call often comes in while a family is standing in a hospital hallway, trying to answer questions from a nurse, a sibling, and a receiving facility at the same time. The call goes better when one person can quickly confirm where the patient is, what the doctors are saying today, and who at the bedside can speak for the medical team.
What to have in front of you
Start with the details a coordinator will ask for first:
- Current location: Hospital name, city, state, unit, and room number.
- Destination plan: The preferred receiving hospital, rehab center, or home city, if discharge planning is still being finalized.
- Bedside contacts: Name and direct line for the nurse, case manager, or discharge planner.
- Medical summary: Diagnosis, current condition, oxygen needs, mobility limits, and any infection-control precautions.
- Key timing facts: Admission date, expected discharge timing, and whether the receiving facility has accepted the patient.
- Insurance and membership details: Policy cards, membership documents, and any prior authorization instructions.
- Family point person: One person who can answer questions and approve changes.
That last item prevents a lot of avoidable confusion. If updates are coming from several relatives at once, the transport team can lose time sorting out which version is current.
What the coordinator actually needs to know
Families often worry that they do not have the right medical terms. Plain language is fine. A good coordinator is trying to answer practical questions: Can the patient sit up or do they need a stretcher? Are they on oxygen, and at what flow? Do they need suction, isolation precautions, or help with pain control during the trip?
The bedside team fills in the rest.
This is also where families often misunderstand what bedside-to-bedside means. It does not just mean a plane is available. It means the transport company can coordinate the sending hospital, ground ambulance if needed, airport handling, flight crew, receiving facility, and final handoff so the patient is not stranded in a lobby, held on a ramp, or discharged before the next step is ready. If a spouse is traveling along, or if the family is trying to bring a small pet home too, say that early. Those details affect ground vehicles, seating, documentation, and timing.
Questions worth asking the hospital before you call
Ask the sending team these questions before you pick up the phone:
- Has the attending physician approved transfer?
- What level of transport does the patient need during the trip?
- Is there a confirmed receiving physician, facility, or home care plan?
- What records, imaging, medication list, and discharge paperwork will be ready to travel with the patient?
- Who should the flight coordinator call first at the bedside?
A short, direct handoff from the nurse or case manager can save hours. When those contacts know a coordinator may call soon, records move faster, physician questions get answered sooner, and the family gets a clearer plan.
Navigating Insurance Costs and Clearances
Money is often the most stressful part of a fly u home decision because families are balancing medical urgency with uncertainty about what will be covered. The right approach is to separate three things that often get blurred together: transport cost, medical necessity, and plan eligibility.
What usually drives the bill
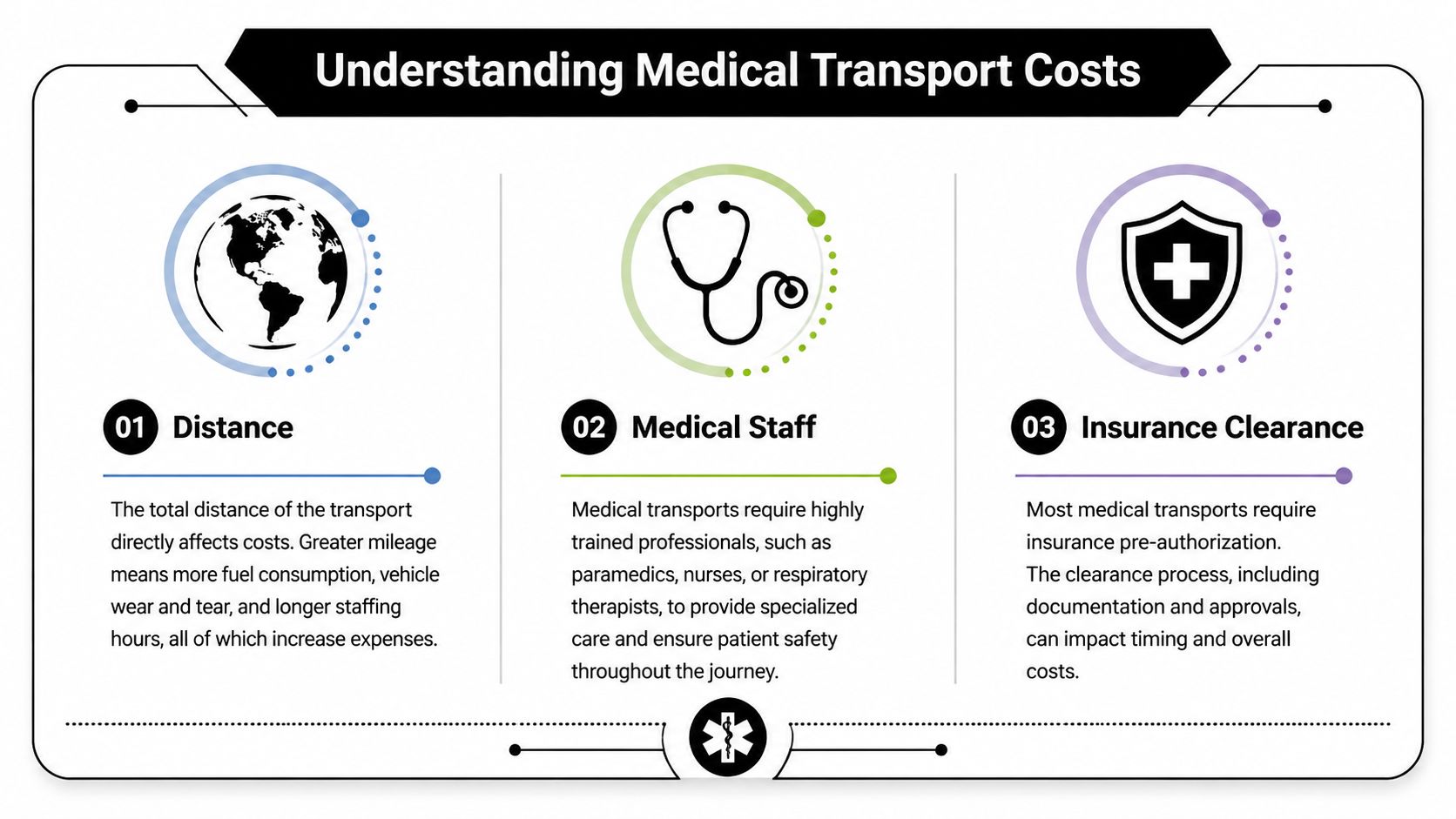
Even when a family doesn't get an exact number on the first call, the price is shaped by a familiar set of factors:
- Distance: Longer flights usually mean more aircraft time, fuel planning, and crew scheduling.
- Medical staffing: A patient who needs a higher-acuity crew changes the mission profile.
- Aircraft setup: Cabin configuration, stretcher needs, oxygen, and other onboard support affect operations.
- Ground coordination: Bedside-to-bedside transport often includes ambulances at both ends.
- Clearances and timing: Hospital acceptance, physician paperwork, and payer review can all influence timing and routing.
None of that means you should wait to call until the paperwork is perfect. It means you should expect the quote and approval process to depend on more than mileage alone.
Membership plans and the gaps families miss
Membership programs can be valuable, but families should read the exclusions carefully. Some Fly-U-Home memberships explicitly exclude residents of Alaska, Hawaii, West Virginia, and North Dakota, and missing that detail can lead to major out-of-pocket exposure. The same source notes that hospital case managers can overlook these exclusions and that costs can exceed $50,000 per flight, according to the Fly-U-Home eligibility overview.
That's the kind of detail people discover too late if they assume “membership” always means “covered.”
How prior authorization fits in
Private insurance may require clinical documentation before approving non-emergent transport. The bedside team usually helps assemble that packet, and a strong case manager is often the difference between a smooth review and a stalled one. If your family hasn't dealt with this before, this guide to managing healthcare prior authorizations gives a useful plain-English overview of how the approval process works.
For families asking about Medicare, expectations need to stay grounded. Coverage rules are narrower than many people assume, especially outside true emergency scenarios. This explanation of whether Medicare covers air ambulance transport is a helpful starting point before anyone counts on federal coverage.
Ask the payer a direct question: “What documentation do you need to review hospital-to-hospital air transport for this patient today?”
Documents that usually move things forward
A coordinator or case manager will often need some version of the following:
- Physician certification or medical necessity statement
- Current clinical notes
- Receiving facility acceptance
- Insurance information and authorization contacts
- Medication and equipment requirements for transport
When those pieces are assembled early, the family gets answers faster and with fewer surprises.
Coordinating the Bedside-to-Bedside Transfer
At 8 a.m., a case manager may be waiting on discharge timing, the sending nurse is asking what travels with the patient, the receiving hospital wants an ETA, and the family is trying to answer one question. Who is in charge of today? Bedside-to-bedside transport works best when one coordinator owns that chain from the hospital room at departure to the room at arrival.
“Bedside-to-bedside” does not mean only the flight. It includes the release from the sending floor, the ground ambulance to the airport, the in-flight medical care, the ambulance on arrival, and the handoff into the receiving facility. If one piece slips, the patient can end up waiting in a hallway, on an airport ramp, or in an ambulance longer than planned.
What transport day actually involves
The coordinator confirms more than a departure time. The sending unit needs to know when the patient should be ready, what records and medications must travel, and which devices stay with the patient. The receiving side needs a realistic arrival window, not a rough guess. Ground crews need the correct entrance, unit number, and contact names at both facilities.
Then the day usually runs in this order:
- Hospital pickup at the sending facility: The ground ambulance checks in, confirms paperwork, and receives report from the bedside team.
- Transfer to the airport: The patient moves with the monitoring, oxygen, stretcher setup, and support equipment approved for the trip.
- Aircraft transfer: The flight crew assumes care, secures equipment, and verifies the clinical plan before takeoff.
- Care in flight: The crew monitors the patient, manages comfort and medications, and documents any change in condition.
- Arrival ground transfer: A receiving ambulance meets the aircraft and continues to the accepting hospital or rehab facility.
- Bedside handoff at destination: The transport team gives report to the new clinical team and transfers the patient into facility care.
Families often ask for a plane. What they need is a managed medical handoff at every step.
Where delays usually happen
The common problems are rarely dramatic. A floor nurse may not know the patient is leaving from a side entrance. A medication list may be outdated by a few hours. The family may assume they can ride along without asking early enough to reserve space. I have also seen transfers stall because the receiving room was assigned, but the unit had not been told the patient was close.
Those are preventable issues. Good coordination means calling the unit, confirming the bed, checking ambulance timing, and making sure the bedside staff know exactly what is happening.
Family members and pets
This part matters more than many guides admit. Families want to know whether a spouse can stay close, whether an adult child can ride with a parent, and whether a pet can come too. Those questions affect the patient's comfort and the family's ability to cope with a hard day.
Med Jets by Air Trek plans for those details directly. Dedicated medical aircraft can often accommodate family members, and the team can discuss pet-friendly options during trip planning. The answer depends on the patient's condition, the amount of medical equipment required, the crew configuration, and aircraft limits. Ask early. If having a family member or pet nearby will make the trip easier on the patient, say that on the first call so the mission can be set up correctly.
If relatives need to travel separately and meet the patient at the destination, practical local planning still matters. A guide to stress-free airport car service to SeaTac is one example of the kind of advance ground planning that can cut down confusion on arrival day.
What the crew is doing while the family waits
The flight time is active care time. The medical team is reassessing the patient, checking comfort, watching for changes related to altitude and movement, updating documentation, and preparing the report for the receiving team. Families may not see that work, but it is a large part of what makes a bedside-to-bedside transfer safe.
For a closer look at how these missions are set up, Med Jets by Air Trek outlines its emergency medical transport services and the operational steps behind a coordinated transfer.
When this process is run well, the family is not calling three vendors for updates. They know who to contact, what happens next, and where their loved one is in the chain of care.
Arrival Handoff and Continuity of Care
The aircraft is down, the ambulance doors open, and families often expect the hard part to be over. In practice, arrival is another handoff point, and it needs the same attention as departure.
The flight crew gives the receiving team a direct clinical report at the bedside. That report covers the patient's status before takeoff, treatment provided in flight, current medications, oxygen or ventilator needs, pain control, and any change the crew saw en route. The goal is simple. The receiving nurses, physicians, or rehab staff should know exactly what they are inheriting before the transport team steps away.
What bedside-to-bedside means at the destination
This term gets used loosely, so it helps to be specific. It does not just mean an airplane ride followed by a drop-off at the front door. It means the patient is physically transferred into the care of the receiving facility, with report, paperwork, and equipment transition completed by the appropriate medical teams.
That final hour can feel slower than families expect. The patient may be moved to a hospital bed, monitors may be changed over, IV lines checked, orders confirmed, and admission questions handled. If the destination is a rehab center or long-term care facility, staff may also review mobility limits, feeding plans, skin protection, and medication timing before the transport crew leaves.
This is also where good coordination shows. If the receiving room is not ready, if the nurse taking report is tied up, or if a medication order needs clarification, the family needs one clear update and a realistic timeline, not guesswork.
What families and case managers should have ready
A short checklist prevents avoidable delays on arrival:
- Photo ID and insurance information: The receiving facility may ask for them again, even after pre-admission.
- A current medication list: Do not assume every record transferred cleanly.
- Advance directives or power of attorney documents: Keep copies in hand, not packed in checked luggage or a suitcase with ground transport.
- One decision-maker on point: Staff need to know who can answer questions and sign paperwork.
- Patient basics that affect immediate care: Glasses, hearing aids, dentures, chargers, and a phone for family contact.
If a spouse, adult child, or case manager is meeting the patient at the destination, arrive early enough to handle admissions without rushing. If a pet is part of the reunion plan, confirm facility rules before arrival. Families are often focused on getting everyone back together, but many facilities have strict limits on where animals can go, even when the flight itself allowed that arrangement.
A smooth handoff is usually quiet. That is a good sign. It means the report was clear, the room was ready, and the next team could pick up care without gaps.
Frequently Asked Questions About Medical Flights
People usually ask the most important questions after the major decisions are made. That's normal. Once the patient is accepted and the transport is taking shape, the practical worries come into focus.
Why do some families prefer a family-operated provider
Consistency. In a family-operated program, families often value speaking with the people managing the transport rather than being passed between unrelated departments. That can matter when plans change quickly, when the sending hospital calls with an update, or when the family needs a straight answer about timing, companions, or paperwork.
It also tends to make communication feel more accountable. The handoffs are fewer. The tone is clearer.
Can a patient on a ventilator be transported
Yes, if the patient is appropriate for that level of air medical care and the aircraft is configured for it. Ventilator transport is part of what medical aircraft and critical care crews are built to handle. The key question isn't whether ventilator transport exists. It's whether the transport team has reviewed the patient's current settings, stability, and in-flight needs.
That decision belongs to the medical team overseeing the mission.
What happens if weather turns bad
The flight waits.
That answer can frustrate families who are desperate to get moving, but it's the right one. Pilots and operational teams monitor weather, route conditions, and airport limitations continuously. If conditions aren't safe, the mission is delayed or rescheduled. Good coordinators will tell you that plainly and keep updating you until a safe window opens.
Safety decisions should sound firm, not negotiable.
How much luggage can a family member bring
Usually less than people hope. Medical aircraft carry equipment, supplies, and weight-sensitive loads, so personal baggage is limited. Soft-sided bags are often easier to accommodate than hard suitcases. The coordinator should give exact guidance before departure.
The safest approach is to pack only what the patient or companion will need for the transfer and the first part of admission.
Can a family member ride with the patient
Sometimes yes. Sometimes no. It depends on the aircraft setup, the patient's condition, and how much space the medical crew and equipment require. This should be discussed early because it affects not only comfort but also family travel planning.
Can pets travel too
Some operators can accommodate pets, but policies differ and safety rules still apply. If the pet is part of the plan, bring it up immediately. Don't assume it can be added later.
What's the single biggest mistake families make
Waiting too long to line up the receiving side.
Families often focus on the aircraft first because that feels urgent and visible. But transfer delays often come from the hospital side. If the receiving physician hasn't accepted the patient, or the bed hasn't been confirmed, the aircraft can't solve that by itself.
If you need help arranging a fly u home transfer, Med Jets by Air Trek provides family-operated air ambulance and medical transport coordination, including bedside-to-bedside planning, family-friendly jet configurations, and 24/7 support for hospitals, case managers, and families.