A hospital says your mother is ready for discharge, but home is several states away. Your father can't lift her. She needs help transferring, regular medications, and a safe place to lie flat for most of the trip. Everyone is asking a different question at once. Can she fly? Will insurance help? Who talks to the receiving facility? What happens if she needs oxygen on the road?
That's the moment when many families discover long distance medical ground transportation.
For some patients, this service turns a stressful, complicated move into a structured transfer with a medical crew, a vehicle set up for patient care, and a plan that follows the patient from pickup to arrival. For case managers, it fills the gap between a standard discharge and a high-acuity emergency transport. For families, it often means a loved one can travel safely without being squeezed into a car ride that's too long, too painful, or too medically risky.
The need is real. Transportation barriers keep people from care at every level of the system. A U.S. Agency for Healthcare Research and Quality analysis found that 6.2% of U.S. civilian noninstitutionalized adults reported that lack of reliable transportation had kept them from medical appointments, meetings, work, or daily necessities in the prior year, with the rate rising to 20.4% among adults with Medicaid and 9.1% among adults with at least three listed health conditions. A separate peer-reviewed review found transportation barriers may cause foregone or delayed care in up to 3.6 million people annually and account for 25% or more of missed clinic appointments (AHRQ transportation access analysis).
When Your Loved One Needs to Travel a Long Distance
The call often comes fast. A rehab stay is ending. A skilled nursing bed opens near family. A patient needs to return home after treatment in another state. On paper, it sounds simple: get from one facility to another. In real life, it rarely feels simple.
Families usually aren't just arranging a ride. They're trying to protect someone who is weak, confused, in pain, on oxygen, or unable to sit upright for hours. Case managers are balancing discharge timing, physician orders, facility communication, and a family that's scared of making the wrong call.
A common example looks like this. An older adult has been hospitalized far from home after a fall or illness. The patient is stable enough to leave the hospital, but not stable enough for a family car. The family wants door-to-door support, help with transfers, and a crew that can monitor the patient along the way. That's where long distance medical ground transportation often becomes the practical answer.
You don't need to solve the whole transfer at once. You need to turn it into decisions: Is the patient medically stable for ground? What level of crew is needed? Who is receiving the patient? What does the quote include?
This kind of transport sits between everyday travel and emergency response. It's designed for planned, non-emergency movement over significant distance, often when the patient needs more support than a wheelchair van, rideshare, or family vehicle can provide. It can also be less overwhelming than families expect once they understand the workflow.
If you're arranging travel for an older adult, the broader topic of medical transport for seniors can help you understand where long-distance ground service fits among other care options.
The key shift is mental. Instead of thinking, “How will we ever get them there?” start thinking, “What level of transport matches the patient's condition, and what information does the provider need to build the trip safely?”
Defining Medical Ground Transportation
A good working definition helps families make better decisions. Long distance medical ground transportation is a planned, non-emergency road transfer for a patient who cannot safely make a long trip in a private car, on commercial travel, or in a basic wheelchair van. The goal is to move the patient from one setting to another while keeping the trip medically appropriate, organized, and tolerable.
What this service is and what it isn't
The easiest way to understand it is to place it between two familiar options.
On one side is emergency ambulance service. That service is built for urgent response and rapid transport to the nearest appropriate hospital. On the other side is ordinary travel, such as a family car, rideshare, or wheelchair van, where the rider can usually sit up, transfer with little help, and go without ongoing medical attention.
Long distance medical ground transportation sits in the middle. It works like a care-focused road transfer. The patient may need to lie flat, use oxygen, be repositioned, receive help with medications, or be watched closely over many hours. The trip is scheduled in advance, and the route, crew, and timing are built around the patient's condition rather than convenience alone.
That distinction matters because families often ask the wrong first question. Instead of asking, “How far is the trip?” it helps to ask, “What support does the patient need for the entire ride?”
Who usually needs it
This service often fits patients in situations like these:
- Hospital to home in another state when discharge is appropriate but the patient is not safe in a private vehicle
- Facility-to-facility transfer for rehab, skilled nursing, long-term care, or specialty follow-up
- Post-discharge transport for someone who needs oxygen, monitoring, careful positioning, or assistance with transfers
- Travel for ongoing treatment when the patient is medically fragile but does not need emergency air transport
In practical terms, transportation is part of access to care. A missed transfer can delay rehab, complicate discharge plans, or leave a family trying to piece together help one phone call at a time.
How the trip is structured
Many families picture a city ambulance racing across highways. Long-distance ground transport is usually more methodical than that.
A typical trip is prearranged, with a sending location, a receiving location, a medical summary, and a transport plan. Providers often use custom-configured vehicles with room for a stretcher, medical equipment, supplies, and sometimes one family rider. The crew commonly includes two certified drivers and an onboard nurse or medic, depending on the patient's needs and the company's model.
The road schedule is built around tolerance, not speed. That means planned stops, position changes when needed, medication timing, and a realistic daily mileage range rather than a nonstop push.
One useful comparison is this. A private car trip asks the patient to adapt to the ride. Medical ground transport sets up the ride around the patient.
Some companies define "long distance" differently. One provider may start that category at 100 miles, another at 200 or 300. The exact threshold matters less than the care plan, the crew level, and whether the patient can travel safely by road. If you are comparing providers, details like vehicle standards and driver medical requirements may come up, and resources such as a 2026 DOT medical card guide can help explain part of that regulatory background.
Practical rule: If the patient is stable enough for scheduled transport but needs more support than ordinary travel can provide, long-distance ground transport is often the first option to evaluate.
Inside the Vehicle Medical Crew and Equipment
Once families understand the category, the next worry is usually very concrete. What does the vehicle look like, and who is going with my loved one?

What the vehicle is built to do
Most long-distance units are customized vans rather than city-style emergency ambulances. Providers often use vehicles similar to Mercedes Sprinters because they allow enough interior space for patient care, equipment storage, and a smoother long-haul setup.
A standard long-distance ground crew consists of two certified drivers and an onboard nurse or medic. Vehicles are typically customized vans equipped with hospital-grade monitoring, oxygen, and multiple beds to accommodate family. This setup is designed for trips of 500 to 700 miles per day, with planned stops for patient comfort.
In plain terms, the vehicle is built for a different mission than a 911 truck. It needs to support a full day of careful travel, safe loading and unloading, medication handling, and comfort over many hours.
What equipment may be onboard
Equipment varies by provider and by the patient's needs, but families commonly ask about a few basics:
- Oxygen support when the patient has a respiratory need or physician order
- Suction capability for patients who need airway support
- Vital sign monitoring during transport
- Hospital-grade stretcher systems for safe positioning and transfers
- Space for bags, medications, and care items so the trip doesn't feel improvised
Some long-distance vehicles also have bariatric capability. That usually means the provider can plan for higher weight capacity, different stretcher systems, and loading methods that are safer for both the patient and crew.
Who does what on the crew
The crew structure matters more than many people realize. One part of the team is responsible for the road, route, and safe operation of the vehicle. The medical professional focuses on the patient.
That split is important. A patient who needs medication timing, symptom observation, oxygen management, or regular repositioning should not be riding in a vehicle where the only person present is also driving. Long-distance services are designed to avoid that kind of conflict.
If you're evaluating how transport companies handle driver qualifications and safety requirements, a general 2026 DOT medical card guide can help you understand the broader framework around medically qualified commercial drivers.
Understanding care levels
Families often hear terms like BLS, ALS, or CCT and assume they need to memorize them. You don't. What matters is matching the patient's actual condition to the right staffing level.
Here's a simple way to understand it:
| Transport level | Usually fits patients who | Common focus during trip |
|---|---|---|
| BLS | Are stable but need assistance, monitoring, positioning, or stretcher transport | Comfort, observation, basic support |
| ALS | Need more advanced monitoring or interventions during the ride | Higher clinical oversight |
| CCT | Have complex medical needs that require intensive management in transit | Ongoing treatment continuity |
The exact staffing model varies by provider and physician orders. The important question isn't “Which acronym sounds safest?” It's “What does the patient need during the hours between pickup and arrival?”
Ask the provider to explain the planned crew in plain language. A good answer sounds like patient care, not jargon.
Ground vs Air Deciding the Right Transport Method
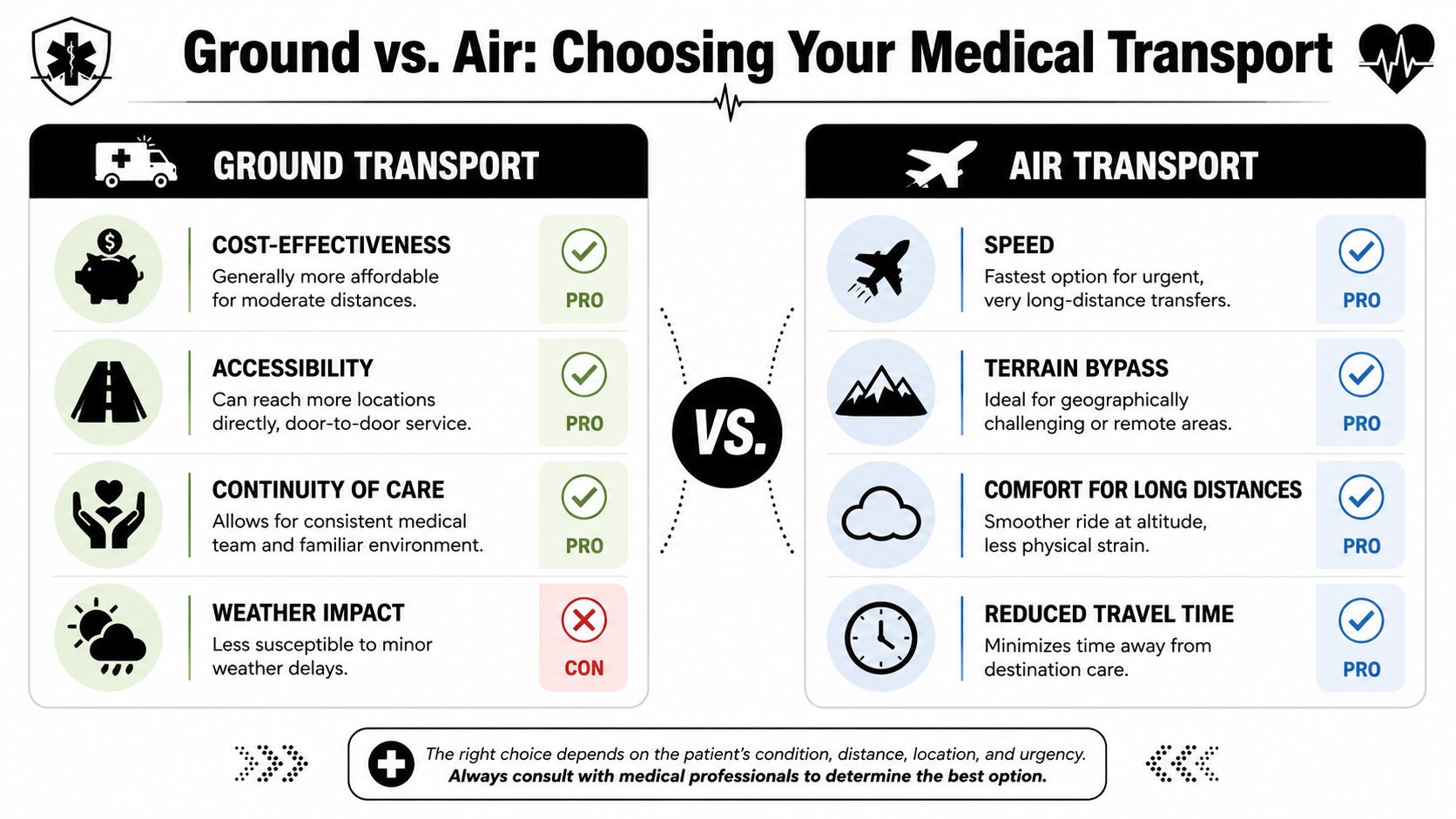
This is the decision families wrestle with most. Ground sounds slower. Air sounds faster. But the safest option isn't always the fastest one, and the fastest option isn't always the most practical.
Choosing between ground and air transport is a major decision point where cost, stability, and comfort often conflict. One industry source notes that air ambulances can cost $10,000 to $20,000, while ground transport is often in the $3,500+ range for comparable distances, and argues that the primary question is: what is safest and most appropriate for this specific patient? (guide to long-distance medical transport options)
A simple decision table
| Factor | Ground transport | Air ambulance | Commercial medical escort |
|---|---|---|---|
| Best fit | Stable patient who needs stretcher support, monitoring, or door-to-door transfer | Patient whose condition or distance makes speed medically important | Stable patient who can tolerate commercial travel with professional accompaniment |
| Door-to-door workflow | Strong fit | Usually involves ground segments on one or both ends | Usually involves multiple handoffs |
| Environment | More continuous and controlled over the whole trip | Fast, but includes airport logistics and transfer points | Least private, most dependent on airport processes |
| Family accommodation | Often easier to arrange | May be limited by aircraft setup | Depends on airline rules and booking structure |
| Positioning and comfort | Good for lying flat, planned stops, and gradual pacing | Faster overall for very long distances | Better for sitting travelers than stretcher patients |
| Typical use case | Discharge, interfacility transfer, relocation closer to family | Urgent long-range transfer | Stable traveler who needs supervision, not full vehicle-based medical transport |
When ground is often the better clinical fit
Ground tends to work well when the patient is medically stable but not travel-independent. That includes people who need to remain on a stretcher, need oxygen or symptom monitoring, or can't tolerate the repeated transfers involved in airports and aircraft loading.
Door-to-door continuity matters more than people think. A patient with pain, confusion, weakness, or pressure injury risk may do better with one carefully managed loading event, one crew, one route, and planned comfort stops. For some families, the ability to ride with the patient is also a major factor.
Ground can also be the more humane option when the patient is anxious or cognitively impaired. A quieter environment, fewer transitions, and a more predictable rhythm can reduce distress.
When air may be the better answer
Air transport usually enters the picture when distance, urgency, or clinical fragility make extended road travel less appropriate. A patient who needs to reach specialty care quickly, or who cannot safely spend many hours on the road, may be better served by an air ambulance.
This doesn't mean ground is unsafe. It means the transport choice should reflect the patient's medical tolerance and the receiving timeline. Some patients need speed more than they need road-based continuity.
Med Jets by Air Trek is one example of a provider that coordinates air, ground, and medical escort services, which can be useful when a case manager wants one company or coordinator to help compare multiple transport modes instead of treating each option separately.
Where commercial medical escort fits
Commercial medical escort is often misunderstood. It's not a substitute for every long-distance medical transfer. It can be appropriate for patients who are stable enough for commercial flight, can tolerate airport handling, and need professional supervision rather than a full air ambulance or ground stretcher setup.
It's less suitable when the patient needs to lie flat, requires complex onboard equipment, or is likely to struggle with check-in, security, boarding, and in-terminal movement.
Questions that help families decide
Instead of asking only, “Which one is cheaper?” ask these:
- Can the patient tolerate the total trip, not just the headline travel time?
- Will the patient need to lie flat, be repositioned, or receive care during the journey?
- How many handoffs are involved from bedside to destination bed?
- Does the receiving facility need the patient by a specific time or condition window?
- Can a family member travel with the patient, and does that matter clinically or emotionally?
A transfer isn't just miles between two points. It's every lift, handoff, delay, and care task between the sending bed and the receiving bed.
For borderline cases, ask both the treating physician and the transport provider the same question: “If this were your family member, what mode would you choose based on this exact medical picture?” The quality of that answer often tells you a lot.
Navigating Costs and Insurance
Money is usually the next source of stress. The problem isn't only the price itself. It's that families often don't know what drives the quote, what insurance might ask for, or which costs appear later if nobody clarified them up front.
What shapes the quote
Long-distance ground transport pricing is usually built around the actual conditions of the trip, not a consumer ride app model. Providers look at distance, crew time, the level of medical support needed, equipment, routing, and whether the patient has special needs such as bariatric transport or complex loading requirements.
Verified cost data helps frame the big picture. A 2024 MASA Assist report using U.S. claims data found that the average medical ground transport cost was about $1,740 per service in 2022, while air medical transport averaged approximately $51,300 in the same period (MASA Assist emergency medical transport cost report).
Independent industry guidance in that same report notes that long-distance stretcher transport is often priced at $5 to $16 per mile, with typical trip totals ranging from about $450 to more than $3,700 depending on distance and care level. It also states that stretcher ground transport can cost 75% to 95% less than an air ambulance on comparable routes.
What families should ask for in writing
A clean quote should answer practical questions, not just list a total. Ask for:
- What level of crew is included
- Whether oxygen or other medical equipment changes the cost
- If the quote is one-way or includes return positioning
- Whether the provider expects overnight logistics on a very long trip
- How pickup timing interacts with hospital discharge timing
If the quote feels vague, ask the provider to walk you through it line by line.
Insurance expectations
Coverage for non-emergency transport can be confusing because medical necessity, policy wording, and authorization rules all matter. Some families assume a doctor's order guarantees payment. It usually doesn't.
In many cases, families need to ask whether the transport is considered medically necessary, whether pre-authorization is required, and whether ground is being treated as the most appropriate transport mode for that patient at that time. If you need a refresher on the basics, this plain-English guide to how health insurance works can make those insurer conversations easier.
For readers specifically trying to sort out policy language around transport, Med Jets also has a helpful tag page on medical transport insurance coverage.
A calm way to handle the financial side
Use this sequence:
- Get the medical recommendation first. Cost matters, but the patient's condition comes first.
- Request a detailed written quote. Verbal estimates are hard to compare.
- Call insurance with the quote and medical summary in hand. Ask about authorization and reimbursement rules.
- Clarify what you may owe out of pocket before booking.
Families feel better once the cost conversation becomes a checklist instead of a guessing game.
Arranging the Transfer Your Step-by-Step Guide
This is the part families and case managers usually need most. Not the definition. Not the theory. The actual workflow.
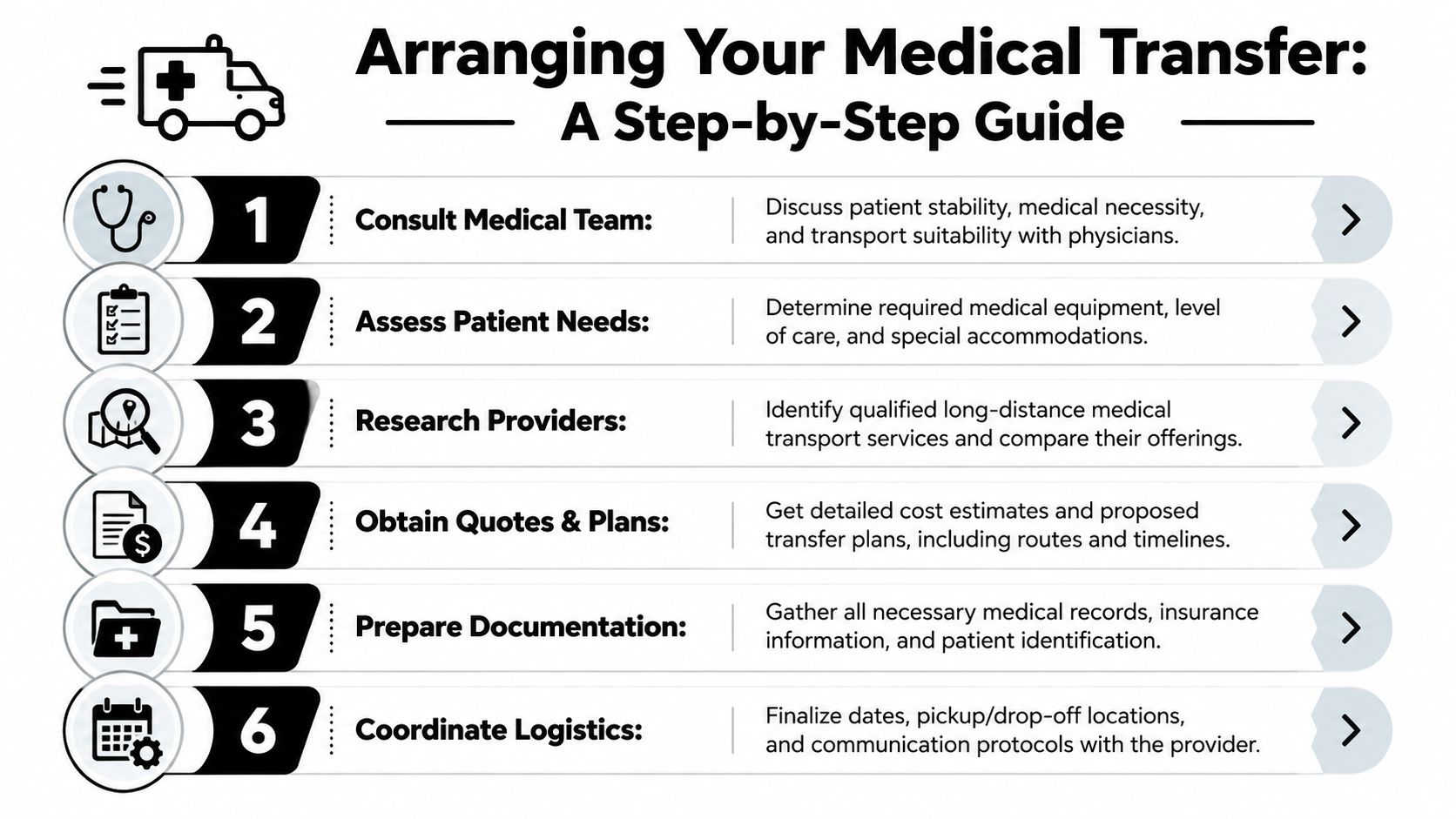
The arrangement process is often more complex than simple guides admit. It usually requires coordination between the hospital, transport provider, and receiving facility, and key details can include nurse escort arrangements, bariatric capability planning, and handoffs across state lines (long-distance medical transportation challenges and workflow).
Step 1 Get the medical picture clear
Before calling providers, gather a concise patient summary.
You want the practical version, not the entire chart. Can the patient sit up? Do they need a stretcher? Are they on oxygen? Do they have wound care needs, pressure injury risk, confusion, feeding needs, or medication timing issues? What assistance is needed for transferring in and out of bed?
A provider can't build a safe plan from “my dad is weak.” They need a real transport profile.
Step 2 Confirm the sending and receiving details
A transfer only works if both ends are ready.
Make sure you have:
- Sending facility contact information
- Receiving facility name and acceptance confirmation
- Target discharge date
- Any destination restrictions, such as admission hours or paperwork cutoffs
Case managers save families from painful delays. A patient can be clinically ready and still not be logistically ready.
Step 3 Contact transport providers with the same core facts
When you call for quotes, give each provider the same information so you can compare responses fairly.
Include:
- Pickup location and destination
- Patient diagnosis in practical terms
- Mobility status
- Required equipment or monitoring
- Whether a family member hopes to ride along
- Any bariatric or special handling concerns
Some families also look at broader service coordinators. If you want a starting point for the category, Med Jets offers information on private medical transport services, which can help clarify what different providers may include.
Step 4 Review the transport plan, not just the price
A good plan should tell you more than “we can do it.”
Ask:
- Who will be on the crew
- What equipment will be onboard
- How the patient will be loaded and unloaded
- Whether the route includes planned comfort stops
- How updates will be shared during transport
If a patient has obesity-related transfer challenges, limited mobility, or complex medication timing, the planning conversation should reflect that. If it doesn't, keep asking questions.
The best transport plans feel specific before the trip starts. Vagueness now usually becomes stress later.
Step 5 Gather documents early
The paperwork usually includes some combination of medical orders, discharge paperwork, medication information, identification, insurance information, and receiving facility documents.
Don't wait until the day of travel. Missing paperwork can delay departure, create confusion at arrival, or force the crew to stop and verify details mid-process.
Step 6 Lock in handoff communication
Families often focus on the vehicle and forget the handoffs. Handoffs are where errors happen.
Make sure everyone knows:
- Who releases the patient at pickup
- Who receives the patient at destination
- Which phone numbers are active that day
- What the crew should do if timing changes
This matters even more on state-to-state trips. The farther the move, the more important clear contact chains become.
Step 7 Prepare the patient and family
By the time the booking is confirmed, the patient should know what to expect in simple language. So should the family.
Tell them:
- What time the crew may arrive
- How long loading may take
- What personal items can go
- Whether medications should travel with the patient
- Who will receive progress updates
A calm patient usually comes from a calm handoff.
Real-World Examples and Final Preparations
The process becomes easier to understand when you attach it to real situations.
A daughter bringing her father closer to home
A daughter needs to move her father from a rehab facility to a care setting near family in another state. He's stable, but he can't sit comfortably for a full-day car ride and needs help with transfers. The family first worries they need an air ambulance because the distance feels intimidating.
After speaking with the treating team and a transport coordinator, they learn he's stable for road transport with a stretcher setup and onboard clinical support. The deciding factor isn't speed alone. It's that he can travel safely by ground, avoid extra airport handoffs, and arrive directly at the receiving facility.
A case manager handling a complex discharge
A hospital case manager is arranging a transfer for a patient with significant mobility limitations and specialized positioning needs. The challenge isn't just finding a vehicle. It's making sure the provider can handle the loading plan, communicate with the receiving team, and manage the comfort issues that could become safety issues on a long trip.
In that kind of case, the strongest provider usually isn't the one with the fastest sales response. It's the one that asks detailed questions, verifies equipment needs, and coordinates the bedside-to-bedside workflow.
A family choosing against commercial travel
Another family starts by assuming a medical escort on a commercial flight will be simpler. But their loved one is confused in unfamiliar environments and becomes distressed during repeated transitions. The airport process itself becomes the problem.
Ground transport makes more sense because it reduces those transitions. One pickup. One crew. One care environment. One destination handoff.
If the patient is likely to struggle with repeated transfers, confusion, or prolonged sitting, convenience on paper may not be convenience in practice.
Day-of-transfer checklist
The day of travel goes better when the basics are packed and confirmed.
Bring or verify these items:
- Identification and paperwork. Keep photo ID, insurance cards, discharge papers, and destination details together in one folder.
- Current medications. Send them in original containers if possible, and make sure the crew knows what the patient has already taken.
- Comfort items. Glasses, hearing aids, dentures, phone charger, blanket, and a familiar pillow can make a long ride easier.
- Change supplies. Include incontinence supplies, wipes, and a spare set of clothing if relevant.
- Contact list. Have the sending facility, receiving facility, primary family contact, and transport company numbers in one place.
Before departure, ask the crew three practical questions:
- Who should I call for updates during the trip?
- What is the expected arrival window?
- What would cause a change in plan on the road?
Long distance medical ground transportation works best when no one treats it like “just a ride.” It's a coordinated care move. When families and case managers understand the process, the transfer becomes far less intimidating and much more manageable.
If you're comparing transport options for a medically fragile patient, build your plan around the patient's actual tolerance, the number of handoffs involved, and the destination's requirements. That approach leads to better decisions than choosing by price or speed alone.