In the United States, 42,887 organ transplants were performed in 2022, setting a new annual record and rising 3.7% over 2021, according to HRSA's transplant update. That number changes how people should think about medical organ transport. This isn't a rare side function tucked behind transplant medicine. It's a nonstop logistics system that has to work at clinical speed, with aviation discipline and hospital-grade documentation.
Families usually see the miracle. Coordinators see the clock.
The job is never just “get the organ there fast.” The primary objective is to move a time-sensitive organ through a chain of handoffs without breaking temperature control, losing traceability, missing a runway slot, delaying the recipient OR, or creating uncertainty about package integrity. Every weak link matters.
That's why experienced teams treat medical organ transport as a coordinated clinical mission, not a courier run. The route, the packaging method, the custody trail, the flight choice, the backup plan, and the final hospital delivery all have to align. When they do, transplant teams can accept organs from farther away, make better use of preservation technology, and reduce avoidable risk. When they don't, even a fast trip can become the wrong trip.
The Unseen Race How Organ Transport Makes Miracles Possible
In 2022, the United States performed 42,887 organ transplants, including 25,498 kidney, 9,528 liver, 4,111 heart, and 2,692 lung transplants, with 6,466 living organ donors, according to HRSA's annual record report. Numbers at that scale only happen when a transport system can move with clinical precision under real operational pressure.
From the outside, organ transport can look like a fast airport transfer. In practice, it is a chain of time-dependent decisions made by people who have very little margin for error. The organ has to stay within preservation parameters, the custody trail has to remain clear, and the recipient hospital has to be ready when wheels touch down. If any one of those pieces slips, speed alone does not save the case.
Why the logistics matter so much
Every trip is shaped by constraints that families rarely see. Traffic around the donor hospital. TSA or airport access procedures. Weather cells on the route. Crew availability. Aircraft range. Commercial schedule limits. Recipient operating room timing can also change with almost no notice.
Experienced coordinators build the plan in layers, because one good answer is never enough.
- Clinical fit: The packaging and preservation method must match the organ, distance, and expected transit time.
- Transport control: The route should reduce handoffs, protect chain of custody, and limit exposure to avoidable delays.
- Hospital timing: Arrival has to line up with the recipient center's OR, staffing, and final readiness checks.
- Backup planning: If the first aircraft diverts or a connection fails, the recovery team needs a second path immediately.
I have seen cases where the fastest option on a screen was not the safest option in the field. A direct charter with tighter custody control may beat a commercial itinerary with multiple handoffs. In other situations, a well-timed commercial segment works perfectly and avoids unnecessary cost. Good coordination means choosing the method that fits the case, not forcing every case into the same playbook.
That is also why teams involved in organ recovery transport coordination focus as much on handoffs and contingency planning as they do on departure time.
What families and case managers often miss
The highest-stakes decisions usually happen before the organ leaves the hospital. Provider selection, aircraft choice, courier handoff points, packaging verification, and communication protocols all affect risk. Case managers and families who understand those trade-offs ask better questions and spot weak plans earlier.
A reliable transport operation does more than move an organ quickly. It creates control under pressure. That is what gives transplant teams the confidence to accept an organ, commit OR resources, and proceed without adding avoidable uncertainty.
The Organ Journey From Donor to Recipient
A donated organ begins its trip long before anyone books an aircraft. The process starts inside a hospital, where donor identification and consent set the entire chain in motion. From there, the timeline compresses quickly. Recovery teams, coordinators, labs, transport teams, and recipient hospitals all work in parallel.
This visual captures the full path at a high level.
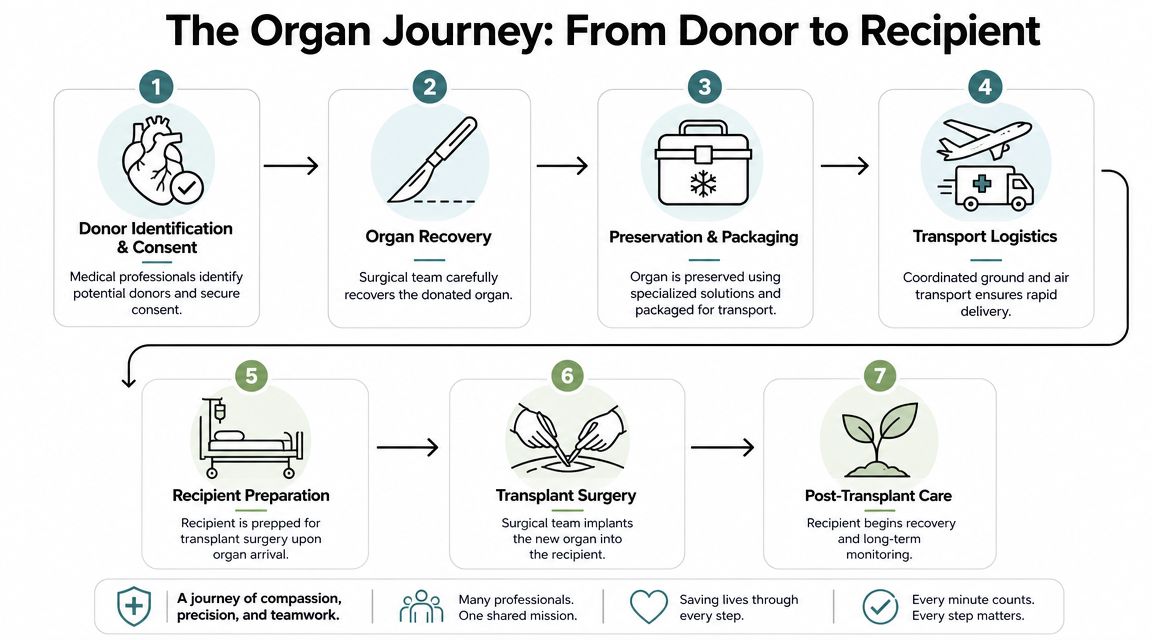
What happens first
Once a donor is identified and the donation pathway is active, the recovery process is coordinated around clinical suitability and timing. The recovery surgical team evaluates the organ, prepares for procurement, and works to protect organ quality from the start.
Packaging isn't an afterthought. The preservation approach, labeling, and handoff details are set before the organ leaves the recovery hospital. Teams involved in organ recovery transport operations know that the clean handoff from OR staff to transport personnel is one of the most sensitive points in the chain.
The handoff that can't be sloppy
Strong systems are exemplified when the organ is packaged, documented, and transferred to a dedicated transport path. Depending on distance and urgency, that may involve ground movement only, a commercial flight segment, or a chartered aircraft with direct airport-to-hospital coordination.
At this stage, a good coordinator is tracking more than mileage:
- Release timing: When exactly did the organ leave the recovery site?
- Custody record: Who signed for it, and where?
- Environmental control: Is temperature being maintained and monitored?
- Receiving readiness: Is the recipient center prepared for immediate transfer on arrival?
A successful trip feels smooth because the friction was removed before transport began.
Arrival is not the end of transport
The final leg is often the most underestimated. A flight can land on time and still fail operationally if the receiving hospital isn't synchronized. Ground pickup, security access, elevator routing, and OR timing all matter.
The organ is delivered to the recipient center, verified, and brought into the transplant workflow. Only then has transport done its job.
That's the core truth families and case managers should know: medical organ transport is one continuous chain. It isn't recovery, then transport, then surgery as separate worlds. It's one tightly connected process, and every transition has to hold.
Preservation Methods and The Critical Time Window
The clock in medical organ transport is biological, not just logistical. Once an organ is removed from normal blood supply, injury risk rises as cold ischemia time, often shortened to CIT, gets longer. That's why transport planning starts with preservation. The route is built around the organ's condition and support method, not the other way around.
This comparison helps explain the difference between traditional and modern approaches.
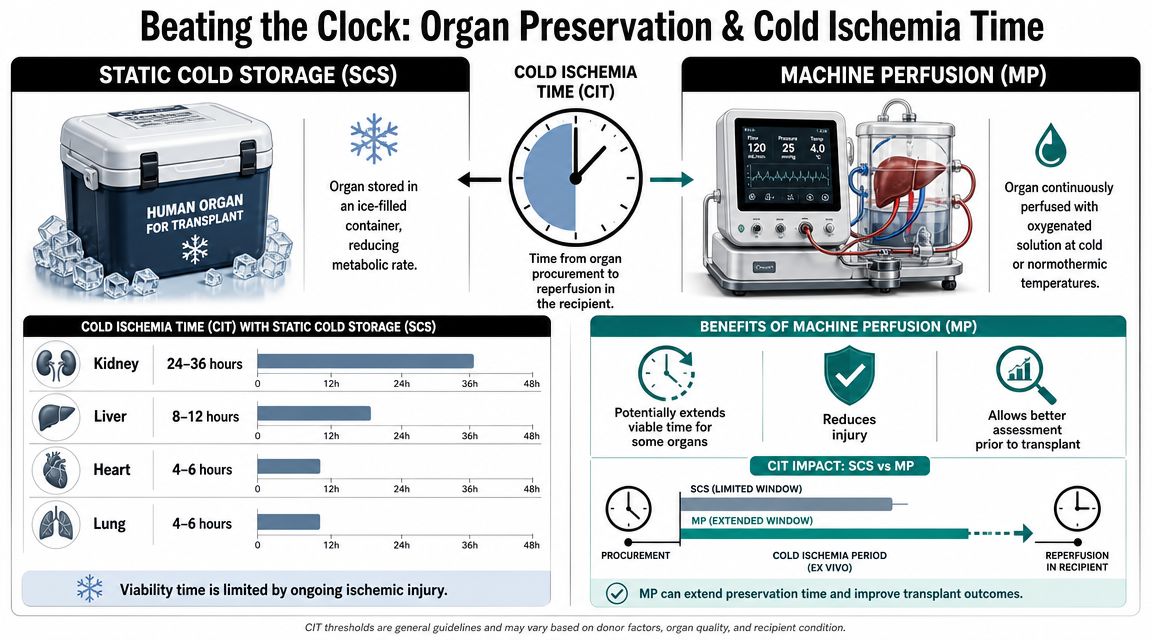
Think of preservation as a biological hourglass
Static cold storage is the most recognized method. The organ is cooled to slow metabolism and packaged for transport. It's simple, established, and still widely used.
But modern transplant programs don't rely on one method for every mission. According to UChicago Medicine's report on donor organ transport technology, some lung transport systems maintain donor lungs at 4 to 8°C without ice, while other systems use warm perfusion to keep lungs oxygenated and perfused with blood during transit. Operationally, that matters because it can extend viable transport windows and expand the donor radius.
What works in practice
The preservation method should match the trip profile.
- Shorter, simpler movements: Static cold storage may be appropriate when the route is direct and handoffs are limited.
- Longer or more complex transports: Active preservation can provide more stability when distance, timing uncertainty, or recipient urgency makes the window tighter.
- High-sensitivity organs: Teams may prefer a system that supports the organ during transit rather than only cooling it.
The practical lesson is straightforward. Preservation technology doesn't replace logistics discipline. It gives logistics more room to succeed.
A short explainer is useful here because the transport decision often starts with the preservation decision.
Cold storage versus perfusion
| Method | What it does | Best fit | Main trade-off |
|---|---|---|---|
| Static cold storage | Lowers metabolic demand through cooling | Direct routes with fewer variables | Less flexibility if delays occur |
| Cold perfusion systems | Maintains controlled cold conditions with more active support | Longer-distance or higher-risk routing | More equipment and coordination |
| Warm perfusion systems | Supports the organ while oxygenated and perfused in transit | Time-sensitive cases where assessment and support matter | More complex transport planning |
The route should serve the preservation method. If the organ needs tighter control, don't build a plan around multiple uncertain handoffs.
Questions coordinators should ask early
Before transport is locked in, ask:
- What preservation system is being used?
- Does the container require special handling in ground or air transit?
- Can the selected flight path support that system without risky delays?
- Is the receiving center comfortable with the projected arrival window under that preservation method?
That's where strong medical organ transport teams earn their keep. They don't treat preservation as packaging. They treat it as the operating condition for the whole trip.
The Team Behind the Transport Roles and Responsibilities
Medical organ transport only looks simple from a distance. Up close, it's a relay among people with very different jobs, authority, and timelines. Confusion usually starts when families or newer coordinators assume one team “handles everything.” In reality, each group owns a separate piece of the mission.
This role map makes the handoffs easier to understand.
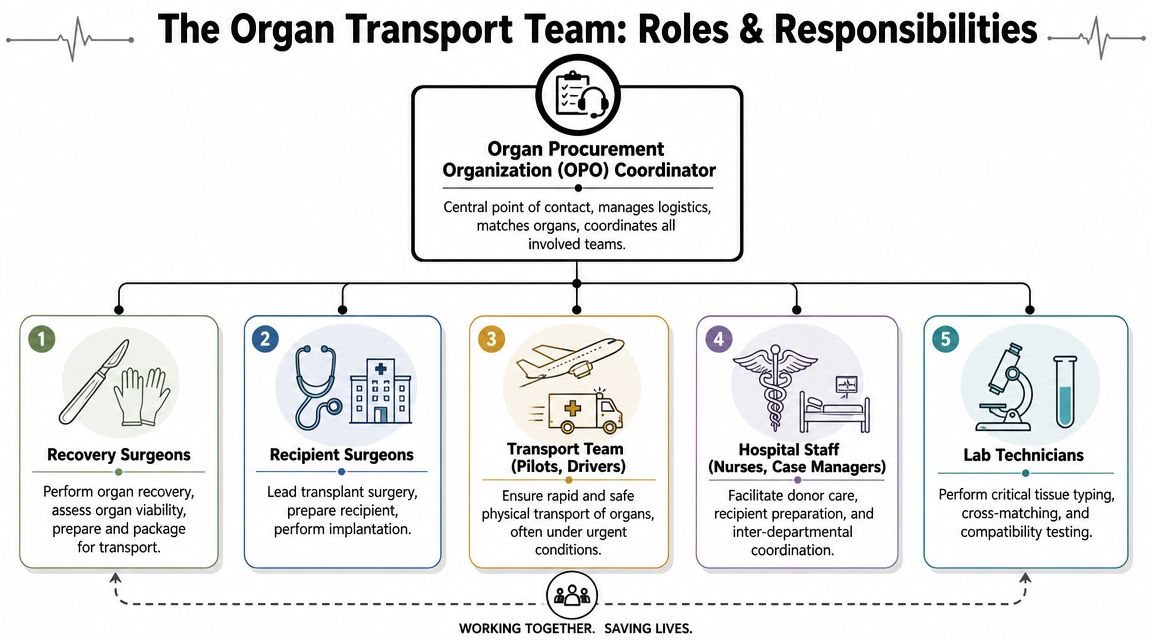
Who runs point
The central coordinator is usually the Organ Procurement Organization contact. That person aligns recovery timing, recipient coordination, documentation flow, and transport communication. If nobody is clearly running that board, the risk of avoidable error goes up.
Recovery surgeons are responsible for organ recovery, condition assessment, and immediate preparation for transfer. Recipient surgeons prepare for implantation and need accurate, real-time updates on estimated arrival and organ status.
Hospital staff, including nurses and case managers, keep both ends of the operation moving. Lab teams handle compatibility-related work. Transport personnel execute the physical movement, but they also protect chain-of-custody and report status throughout the trip.
Where mistakes usually happen
The weak spots aren't usually dramatic. They're ordinary failures of coordination.
- Assumed ownership: One team thinks another team confirmed the final handoff details.
- Partial documentation: Critical information exists, but not in the package moving with the organ.
- Timing drift: OR preparation and transport arrival slowly move out of sync.
- Equipment mismatch: The vehicle or aircraft isn't planned around the preservation system's needs.
Engineers who work on regulated healthcare hardware often think the same way transport coordinators do. The product has to perform under real constraints, not just in ideal conditions. That's why Sheridan Technologies' medical device guide is relevant here. It's useful background on how medical systems are designed around usability, reliability, and compliance under pressure.
What a strong transport carrier actually owns
A specialized carrier doesn't replace the clinical teams. It fills the logistics role that hospitals and OPO staff can't safely improvise in real time.
That includes:
- Route execution: Ground and air planning based on timing, custody, and environmental control
- Continuous updates: Dispatch-level communication to the sending and receiving sides
- Transfer discipline: Clean sign-out and sign-in at each handoff
- Support equipment awareness: Knowing what the preservation container or escort team needs
For teams coordinating broader clinical movement and supplies, aero medical supply logistics can be just as important as the aircraft itself. The mission only works when the transport setup matches the medical payload.
The best-organized transports usually have one clear coordinator, one current timeline, and no ambiguity about who owns the next step.
Choosing the Right Transport Method
This is the decision point that case managers and transplant coordinators wrestle with most. Should the organ move by dedicated ground unit, on a commercial airline, or by private charter? There isn't one right answer for every case. The right answer is the option that protects the organ, keeps custody clear, fits the preservation method, and matches the clinical timeline.
According to FAA guidance on organ transport, organs may travel on commercial flights under FAA, TSA, and HRSA frameworks, either in the cabin or as cargo, with standard securement and screening requirements. The same guidance also makes the larger point that matters most operationally: the safest route is the one that minimizes handoffs, preserves temperature stability, and keeps the organ continuously tracked.
Side-by-side comparison
| Factor | Ground Ambulance | Commercial Airline | Private Charter Jet |
|---|---|---|---|
| Speed over short distance | Strong when airports add complexity | Variable, depends on schedule and airport flow | Usually strong when direct routing is available |
| Chain-of-custody control | High if it stays one crew door-to-door | More vulnerable to handoffs and airport transitions | High, especially with dedicated mission planning |
| Geographic reach | Limited by distance and traffic | Broad network if schedules align | Broad, with more direct control |
| Delay exposure | Traffic, road closures, local conditions | Schedule changes, missed connections, airport delays | Weather and airspace still matter, but schedule control is stronger |
| Team accommodation | Limited | Limited and dependent on airline rules | Better suited when personnel or specialized equipment must travel together |
| Best use case | Short direct transfers | When scheduled service is practical and custody can be protected | Time-sensitive or complex transports needing tighter control |
Ground transport when simpler is better
For shorter routes, ground can be the cleanest option. No airport transfer. No screening delay. No reloading from vehicle to terminal to aircraft and back again.
Ground also works well when the sending and receiving hospitals are within a manageable radius and the preservation plan doesn't require air movement. In those cases, simplicity is a safety feature.
Commercial airline when the network helps more than it hurts
Commercial airline organ transport is real, and it's growing in relevance. It can be workable when flights are available, airport access is smooth, and the custody plan is tightly controlled. It becomes less attractive when the route requires multiple handoffs or a missed connection would create serious clinical pressure.
Paragonix has publicly described a courier model with NORA that included a donor lung moved on a publicly accessible flight using advanced preservation technology, as noted in its announcement on a commercial-flight transport initiative. That doesn't mean commercial is always preferable. It means commercial can be operationally sound when the preservation method, courier process, and route design are all aligned.
A related perspective comes from other temperature-sensitive transport fields. Cryonos GmbH's cryogenic transport overview is about biological sample shipping rather than organ transplantation, but it's a useful reminder that environmental control and handling discipline often matter as much as raw transit time.
Private charter when control matters most
Private charter is often the strongest fit when teams need direct routing, reduced handoffs, or flexibility around exact departure time. It also helps when the preservation system, courier team, or airport geography makes scheduled service awkward.
For transport planners weighing aircraft choices, fixed-wing versus rotary-wing medical flight considerations can help frame when direct range and cabin profile matter more than vertical access.
Med Jets by Air Trek is one option hospitals and families may encounter for coordinated air medical transportation. In a broader medical transport context, the company handles fixed-wing patient transfers and hospital-to-hospital coordination, which is relevant when teams need an aviation partner familiar with clinical movement rather than standard charter logistics.
If the route needs too many handoffs to save money, it may stop being the lower-risk option.
Questions to ask before choosing
- How many custody transfers will this route require?
- What happens if the first leg is delayed?
- Can the preservation system travel safely on the selected mode?
- Does the route match the recipient hospital's OR readiness?
- Will a courier stay with the organ the entire time?
Those answers matter more than a generic promise of speed.
Risk Mitigation and Navigating Complications
Organ transport plans fail in familiar ways. Weather shifts. A runway closes. A driver gets trapped in hospital congestion. A document packet is incomplete. The recipient room turns slower than expected. None of those problems are unusual. What matters is whether the transport plan expected them.
That's why proactive risk mitigation is more important than chasing headline speed. Public discussion in the field has emphasized a broader challenge: providers must balance rising transport costs, access outside major hubs, organ viability, clinical team coordination, and total system cost, not just flight time, as reflected in the Organ Donation Alliance discussion on transportation logistical challenges.
The complications that deserve real planning
Experienced teams prepare for the ordinary disruptions first.
- Weather risk: Build alternatives before departure, not after a diversion.
- Documentation risk: Verify the packet at pickup, not at the airport curb.
- Access risk: Confirm hospital receiving instructions and after-hours entry points.
- Timing risk: Keep the recipient center updated so OR preparation doesn't drift.
What good contingency planning looks like
A credible medical organ transport provider should be able to answer practical questions without hesitation.
- If the primary route breaks, what is the backup?
- Who has authority to reroute in real time?
- How is the organ tracked during every handoff?
- How are the sending and receiving teams updated if timing changes?
If those answers are vague, the plan is weak.
The backup plan shouldn't start with “we'll see what flights are available.” It should already exist before departure.
Cost pressure changes decisions
Cost pressure is changing how some teams think about routing. That doesn't mean lower cost should outweigh organ safety. It means the old habit of defaulting to the most expensive path without evaluating alternatives isn't enough either.
The stronger approach is operationally balanced:
- Use direct ground when ground is cleaner.
- Use commercial air only when chain-of-custody and timing can be defended.
- Use charter when control, flexibility, or escort requirements justify it.
Outside major hubs, access can be uneven. Aircraft availability, airport proximity, weather, and specialized ground support all shape what's realistic. Good coordinators don't promise perfect conditions. They build plans that can survive imperfect ones.
Practical Checklists for Coordination and Documentation
Families need clarity. Case managers need a tool they can use under pressure. A checklist helps because organ transport depends on details that are easy to assume and dangerous to miss.
This visual lays out the two operating viewpoints clearly.
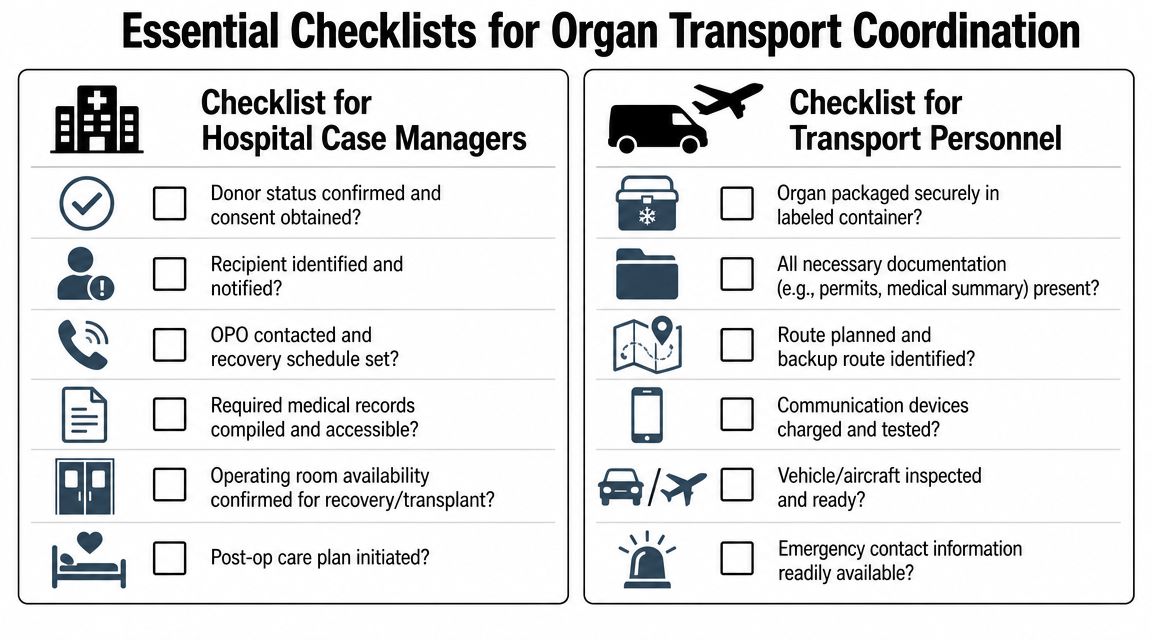
Checklist for hospital case managers
Before confirming the transport plan, verify these points:
- Clinical readiness: Donor status and consent are confirmed, and the recipient pathway is active.
- OR synchronization: Recovery timing and recipient preparation are aligned closely enough that the transport plan still makes sense.
- Transport mode logic: The selected route matches the preservation method and doesn't create unnecessary handoffs.
- Named contacts: One person at the sending side, carrier side, and receiving side is accountable and reachable.
- Contingency agreement: Everyone knows what happens if departure or arrival time changes.
Checklist for transport personnel
The transport side should verify the package and the path, not just the pickup time.
- Container integrity: The organ is packaged, labeled, and ready for the planned mode of movement.
- Chain-of-custody paperwork: Every handoff has a sign-out and sign-in process.
- Medical details present: Donor ID, organ type, blood type information, and temperature logs are traveling with the organ when required by protocol.
- Route backup: Alternate routing has been reviewed if the primary leg fails.
- Hospital access details: Pickup and delivery instructions are confirmed down to building entrance and receiving contact.
Checklist for families
Families often ask what they should do when they're not handling the logistics directly. Focus on understanding, not controlling, the transport mission.
- Ask who is coordinating: Get the name and role of the primary hospital or transplant coordinator.
- Ask about timing in broad terms: Exact times can change. Ask what milestone the team is waiting on next.
- Ask how updates will be shared: One communication channel is better than many mixed messages.
- Ask what's already arranged: Transport, OR planning, and recipient preparation are often moving at once.
The best checklist is the one people use. Short, specific, and tied to named responsibility.
Frequently Asked Questions about Medical Organ Transport
As of September 2024, over 100,000 people in the U.S. were on the waiting list for an organ transplant, including 89,792 waiting for a kidney and 3,456 waiting for a heart, according to the federal organ donation statistics summary. That demand is one reason medical organ transport has to be both fast and disciplined.
Can an organ really travel on a regular commercial flight
Yes, in some situations. Commercial-airline transport is allowed under the applicable federal framework, but it only works well when custody, screening, handling, and timing are all tightly managed. A scheduled flight isn't automatically the safer choice just because it's available.
Who actually carries the organ during transport
That depends on the transport model. A certified courier or designated transport professional may accompany it, or the organ may move through a controlled cargo process depending on the route and provider setup. The important question isn't the job title alone. It's whether custody remains documented and continuous.
What should families ask if they're worried about delays
Ask three direct questions:
- What is the current transport plan?
- What is the backup if that plan changes?
- Who will update us if timing shifts?
Those questions usually reveal whether the operation is tightly managed or still too loose.
Is the fastest route always the best route
No. The best route is the one that protects the organ's condition while keeping the transport chain stable. A route with extra handoffs, uncertain transfers, or poor temperature control can be riskier than a slightly longer but cleaner route.
What documentation matters most
The exact packet can vary by protocol, but teams commonly need the identifiers and logs that prove the organ is what it's supposed to be, preserved the way it's supposed to be, and handed off the way it's supposed to be. Missing paperwork can create the same kind of delay as a transportation problem.
Medical organ transport works when people respect a simple truth: speed matters, but controlled speed matters more. Families don't need to know every aviation detail. They do deserve to know that the team has a real plan, a backup plan, and clear accountability.
If you're evaluating air medical logistics options for a hospital transfer or a time-critical coordination need, contact Med Jets by Air Trek to discuss transport planning, routing, and hospital-to-hospital continuity.