
A domestic medical plane flight usually costs $20,000 to over $100,000, and that price is typically all-inclusive, covering the aircraft, medical crew, onboard equipment, and the ground transport needed to move the patient safely at both ends. For many families, that number lands at the worst possible moment, right when a hospital is saying a loved one needs to move now or when someone far from home can’t return on a regular airline.
That’s usually when core questions start. Why does the quote vary so much? What’s included? Will insurance help? And what happens if the patient is larger, medically fragile, traveling internationally, or needs more than a standard stretcher setup?
I’ve found that people don’t need vague reassurance in this moment. They need a clear explanation of how medical plane cost is built, what changes the quote, and which questions prevent expensive surprises.
What to Expect When You Need a Medical Flight
A common call sounds like this: a daughter is at a hospital several states away, her father has been stabilized after surgery, and the discharge planner says he can’t travel on a standard commercial flight. The family is trying to make decisions fast, but the first quote they hear feels impossible.
That reaction is normal. Air medical transport is highly specialized, and the price trend has moved in the wrong direction for families. From 2008 to 2017, the average price of a fixed-wing air ambulance trip rose by 166%, from $15,684 to $41,674. By 2020, the base charge alone had increased another 27.6% according to Health Care Cost Institute reporting on air ambulance trends.
The part that helps people breathe again is understanding what they’re paying for. This isn’t just a plane ride. It’s a clinical handoff, flight planning, bedside coordination, airport handling, medical staffing, and receiving-hospital timing all wrapped into one mission. That’s why a medical plane quote looks nothing like a last-minute airline ticket.
Practical rule: If a quote looks unusually low, ask what is not included before you compare it to anything else.
A proper transfer usually starts with the sending facility, moves through medical review, confirms the patient’s condition and equipment needs, and only then locks in aircraft and crew. If you’re trying to understand what service is being arranged, this overview of what an air ambulance really does and why it matters more than people think is a useful place to start.
The first questions families usually ask
- Can they fly safely right now? That depends on stability, oxygen needs, monitoring, and whether the patient can tolerate cabin conditions and transport time.
- Is the quote for bedside-to-bedside service? It should include ground segments, not just the aircraft.
- Can someone ride along? Sometimes yes, but it depends on the aircraft layout, patient condition, and crew requirements.
- Will insurance cover it? Sometimes, but coverage turns on medical necessity and plan rules.
Understanding Air Ambulance Services
An air ambulance isn’t just “a private plane with a stretcher.” It’s a bedside-to-bedside medical transport system. The patient leaves one level of care and stays under organized supervision until arrival at the next one.
What bedside-to-bedside really means
A true medical flight usually includes several moving parts:
- Clinical review before launch so the flight team knows the diagnosis, current status, medications, oxygen needs, and equipment requirements.
- Ground ambulance on the departure side to move the patient from hospital bed to airport safely.
- In-flight medical care with the appropriate clinicians and equipment for the patient’s condition.
- Ground ambulance on arrival to complete the handoff to the receiving hospital, rehab center, or home setting when appropriate.
Families often focus on the airplane because that’s the visible part. Operationally, the handoffs matter just as much. A transfer goes badly when those handoffs are rushed, incomplete, or arranged by different parties who aren’t communicating.
Fixed-wing planes and helicopters serve different jobs
Think of a fixed-wing medical jet as the right tool for longer hospital-to-hospital moves, interstate transfers, and many international transports. A helicopter fits shorter-range work, scene calls, or places where runway access is limited.
That difference also explains why people can’t compare every air ambulance quote as if it were the same service. A helicopter may be the only clinically realistic option in one situation, while a fixed-wing aircraft is the efficient option in another.
A useful reminder comes from a PubMed-listed 1998 study on helicopter air medical systems. It found helicopter systems could be more cost-effective per patient than ground ambulances in certain critical cases, at $2,811 per transported patient versus $4,475 for ground, measured in 1991 dollars. The lesson isn’t that helicopters are always cheaper. It’s that the right transport mode depends on the patient and mission, not assumptions.
The cheapest-looking transport option can become the most expensive one if it delays care or can’t safely manage the patient during transfer.
What a medical flight is not
It’s not the same as:
| Service | What it does | When it fits |
|---|---|---|
| Dedicated air ambulance | Full medical aircraft with crew and equipment | Patients who need continuous medical oversight |
| Commercial medical escort | Clinician accompanies a patient on a scheduled flight | Stable patients who can tolerate airline travel |
| Standard non-medical charter | Private flight without air ambulance setup | Not appropriate for patients needing active care |
That distinction matters because many pricing misunderstandings come from comparing a full air ambulance mission to a simpler escort arrangement that serves a different patient profile.
The Anatomy of Your Medical Plane Cost
The fastest way to understand medical plane cost is to separate the quote into four buckets: aircraft operations, medical staffing, logistics, and patient-specific complexity.
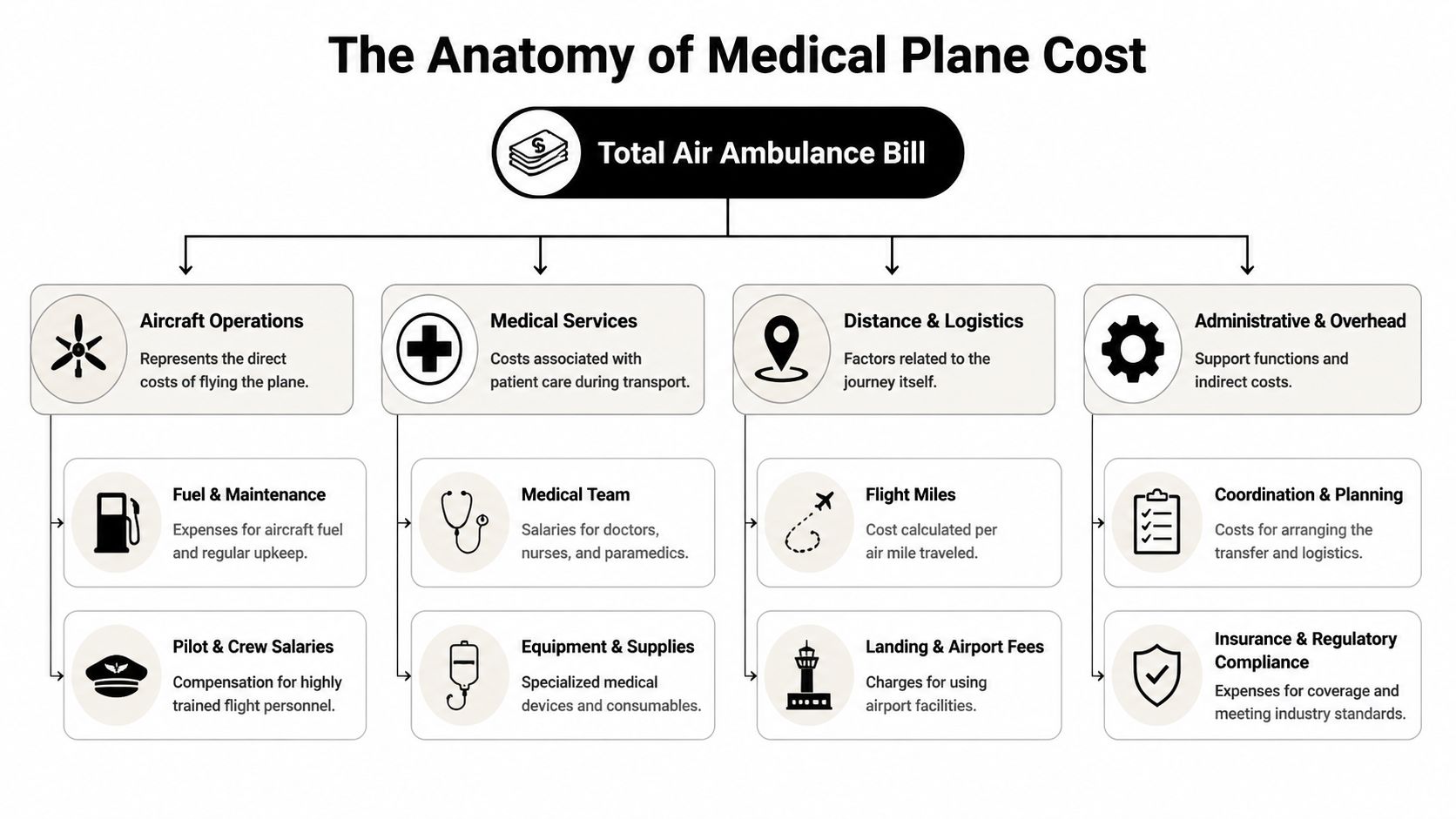
Aircraft and flight operations
A medical jet is expensive to run before a patient ever boards. Jets commonly used in this space, including aircraft comparable to the Cessna Citation family, carry operating costs tied to fuel, pilots, maintenance planning, and compliance. According to Paraflight’s discussion of medical charter flight costs, these aircraft can burn 150 to 250 gallons per hour at $5 to $7 per gallon, and a domestic 4 to 6 hour flight can cost $60,000 to $120,000 once dual-pilot crews and 2 to 4 clinicians are included.
That’s why distance changes a quote so sharply. It’s not just mileage on paper. Longer flights use more fuel, increase crew duty time, and can trigger additional planning around routing and airport handling.
If you want a plain-language comparison of aircraft choices, this breakdown of fixed-wing vs rotary-wing medical transport is helpful.
Medical team and onboard care
Not every patient needs the same crew. One patient may only need monitoring, oxygen, and routine medication support. Another may need a higher-acuity setup with more intensive intervention capability.
That changes the quote in several ways:
- Crew mix matters because a higher-acuity patient may require more specialized clinicians.
- Equipment load matters because ventilators, monitors, suction, medication pumps, and other devices have to be available and secured for flight.
- Cabin setup matters because space is limited and must be configured around the patient’s needs first.
A family member sometimes asks, “Why does an escort-level patient cost less than a full air ambulance patient?” The answer is simple. Stable patients can sometimes use scheduled commercial service with a clinician. Unstable patients need a flying treatment environment.
Ground segments and coordination
The part people overlook most often is everything happening outside the aircraft.
A complete mission may include:
- Medical record review
- Sending physician coordination
- Ground ambulance dispatch at pickup
- Airport handling and timing
- Receiving facility acceptance
- Ground ambulance dispatch on arrival
- Documentation for billing or reimbursement
A quote that omits one of these items may not stay low for long.
Ask one direct question: “Is this quote fully bedside-to-bedside, including both ground ambulances and coordination?”
Special situations that raise the cost
Some missions cost more because the patient does, in practical terms, require a different aircraft setup.
Here are the most common examples:
- Bariatric transport often requires reinforced interiors, wider stretcher access, specialized loading equipment, and weight planning.
- International transport adds customs, permits, language coordination, and more complex receiving arrangements.
- Two-patient or companion-heavy missions can limit aircraft options because cabin space is finite.
- Fragile transfers involving complex lines, respiratory support, or infection-control concerns narrow the list of suitable operators.
None of those factors are “extras” in the way families often fear. They’re mission requirements. The right question isn’t whether they cost more. It’s whether the quote accounts for them upfront.
Navigating Insurance Coverage and Payment
At 9 p.m., a case manager gets the acceptance call from the receiving hospital. The aircraft can be ready tonight. Ten minutes later, the family asks the question that decides whether the trip moves ahead. “Will insurance cover this, and what happens if it doesn’t?”
Medical necessity is the center of the case
Coverage starts with one issue. Why did this patient need an air medical transport, on this date, with this level of care?
Payers usually want the answer in plain clinical terms. The record should show why a ground unit, wheelchair service, private car, or commercial flight was not a safe option. For a specialized mission, that explanation often needs more detail than families expect. A bariatric transfer may require weight and loading limits documented in advance. An international repatriation may need physician notes explaining why the patient cannot tolerate a standard airline itinerary, border delays, or multiple handoffs. A multi-patient or companion-heavy mission can also trigger questions about aircraft choice and whether all travelers were medically or operationally necessary.
If prior approval is part of the process, it helps to explore prior authorization with Simbie AI so everyone involved understands what the payer is likely to request and where delays usually start.
Medicare, commercial insurance, and out-of-network friction
Each payer looks at the same transport from a slightly different angle.
Commercial plans often focus on network status, pre-authorization rules, and whether the chart supports the level of service billed. Medicare has its own coverage standards and payment structure. Families who are sorting through that piece can start with this overview of whether Medicare covers air ambulance.
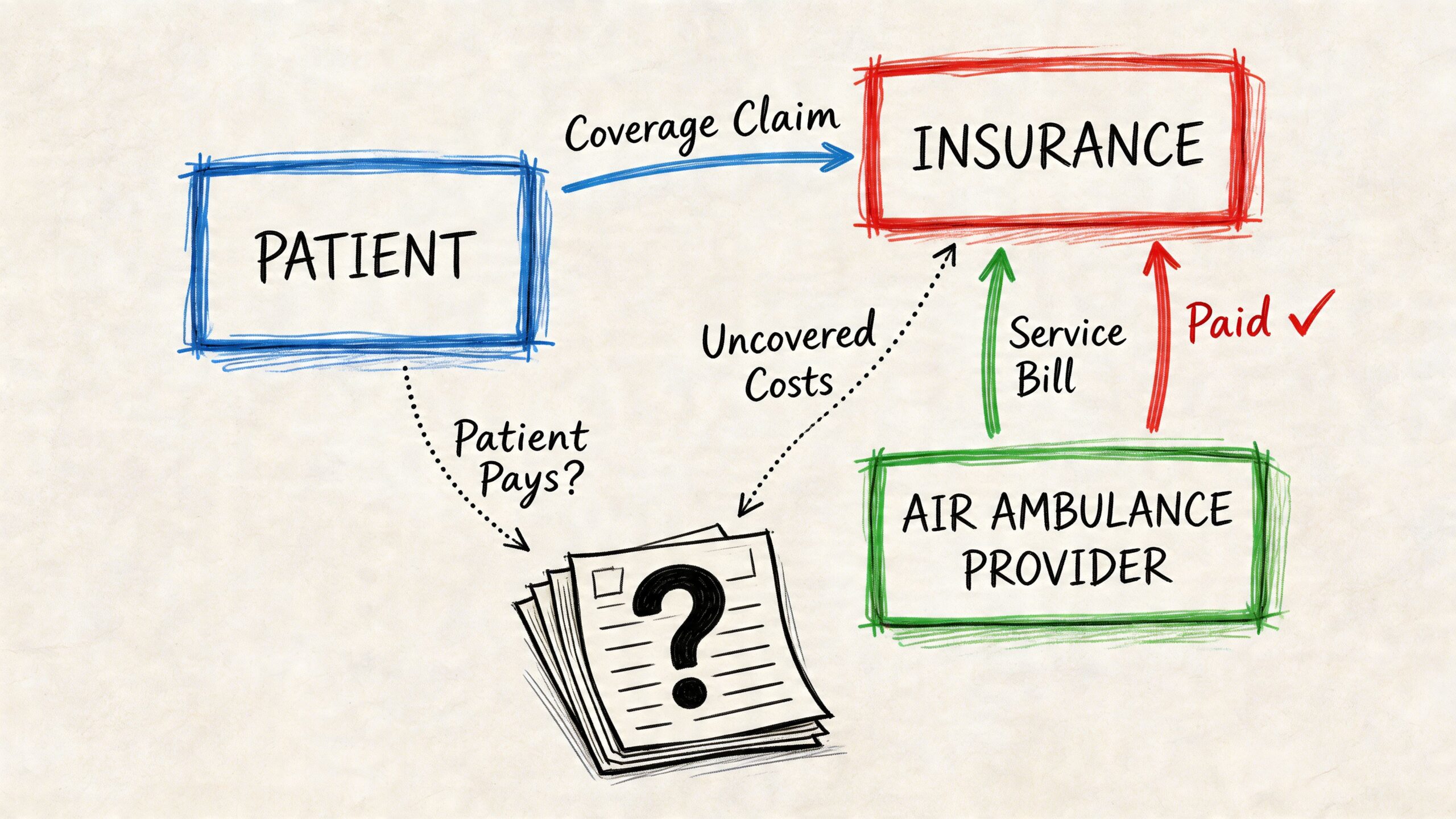
One point causes confusion in higher-acuity transfers. Approval and full payment are not the same thing. Earlier cost reporting on the fixed-wing market showed billed charges, insurer allowed amounts, and Medicare payment levels moving in very different directions over time. In practical terms, that means a claim can be approved and still leave a gap.
That gap tends to widen in specialized transports. Bariatric missions may require an aircraft with fewer operator options. International flights can involve foreign providers, translation, permits, and cross-border billing that do not fit neatly into a domestic insurance workflow. If two patients are traveling together, or if the care team must accommodate more than one medically necessary attendant, the insurer may question every seat and every line item unless the paperwork is unusually clear.
After you’ve reviewed the documents, this short explainer can help people on the family side understand how billing relationships typically work.
How to keep payment surprises under control
A short call list prevents a lot of trouble later.
| Ask this question | Why it matters |
|---|---|
| Is this transport covered as medically necessary under this plan? | Coverage can fail even before pricing is discussed if the chart does not support air transport |
| Is the operator in-network, and if not, what is the out-of-network payment method? | An out-of-network approval may still leave a larger patient balance |
| Does this case require pre-authorization or a case reference number? | Non-emergency transfers are commonly delayed or denied for missing authorization steps |
| Are special mission factors documented in the file? | Bariatric, international, isolation, and multi-patient transports often need extra justification |
| Who is handling claim submission and clinical records? | Families and bedside staff should not be left to assemble the file on their own during a crisis |
| What deposit is due before launch, and is any portion refundable if the payer later denies the claim? | This determines immediate cash exposure, especially in private-pay or international cases |
Write down the payer name, call reference number, and the representative’s name before the aircraft is dispatched.
Payment itself may involve a deposit, a letter of financial responsibility, insurer assignment, wire transfer, card payment, or assistance-company coordination. In my experience, the hardest cases are not always the sickest ones. They are the ones where the flight was medically appropriate, but the insurance file did not clearly explain the special transport requirements before wheels up.
Example Scenarios and Typical Cost Ranges
At 2 a.m., a family may hear “air ambulance” and assume there is one standard price. There is not. A short domestic transfer for a stable patient and an international bariatric repatriation can differ dramatically in aircraft type, crew setup, permits, ground handling, and what insurance will approve.
A state-to-state hospital transfer
A common example is a patient who has finished the highest-acuity phase of care in one state and needs rehab, a specialty bed, or follow-up treatment closer to home. The patient is stable enough for a fixed-wing transfer, but still needs monitoring in flight, medication support, and coordinated ground transport at both airports.
Earlier cost data in this article placed many domestic fixed-wing transfers in a broad middle range. In practice, this is the mission families often expect to be straightforward, but the total still shifts based on runway access, after-hours scheduling, rural pickup points, and whether the sending and receiving hospitals can move the patient without delay.
Ground ambulances on both ends are often the overlooked piece here. If either airport is far from the hospital, that can change the final number more than families expect.
A long-haul or international repatriation
A traveler admitted overseas may need to return home for continued treatment, insurance network reasons, or family support. These flights usually require a medical jet because the distance is too great for a rotor-wing aircraft and the clinical handoff has to stay consistent across many hours.
Costs rise due to factors that do not show up in simple mileage estimates. International permits, customs timing, overflight clearances, airport handling fees, language coordination, and crew duty limits all affect the mission plan. If the patient needs a nurse and physician instead of a standard clinical team, the quote rises again.
I often tell families that international pricing is built from layers, not one expensive item. A medically stable patient can still generate a high quote if the routing is complex, the country requires extra paperwork, or the return leg cannot be efficiently scheduled.
Insurance is also harder here. Many plans cover emergency transport more readily than a planned repatriation, especially across borders.
A bariatric patient transfer
Bariatric transport changes both aircraft selection and loading logistics. It is not just a standard mission with a higher weight figure on the chart.
The aircraft may need a wider loading path, different stretcher equipment, additional crew for safe movement, and stricter weight-and-balance planning. Some airports and ground units are better equipped for this than others. If one link in that chain cannot safely manage the transfer, the operator may need a different aircraft or a different routing plan, and both affect cost.
According to Emergency Assistance Plus on air ambulance cost considerations, bariatric-capable medical flights often cost materially more than standard flights. I also see more insurance friction in these cases, because payers may question whether the upgraded equipment and staffing were medically required or merely preferred. That is why the clinical documentation has to be specific about dimensions, mobility limits, transfer risk, and any equipment needed during loading and flight.
A vague request for a “bariatric flight” usually slows things down. Exact patient measurements and handling requirements lead to better aircraft matching and fewer last-minute price changes.
A multi-patient flight
These missions get less attention, but they do come up. Examples include neonatal twins transferring together, a parent and child traveling on the same medically supervised mission, or disaster-related evacuations where more than one patient is moved under a coordinated plan.
Sometimes a shared mission lowers the cost per patient. Sometimes it does not. The answer depends on acuity, whether each patient needs separate monitoring equipment, how the cabin must be configured, and whether one patient’s care needs limit aircraft options for everyone else on board.
This is also an insurance gray area. Even when the transport is clinically reasonable, payers may review each passenger separately and ask why a combined mission was appropriate. That can create billing complications families do not expect at the start.
The useful takeaway is simple. Price ranges are real, but they only become meaningful after the operator knows the patient’s condition, the route, and the special transport requirements that make one mission routine and another highly specialized.
How to Get an Accurate Quote and Reduce Costs
The best quotes come from good intake information. The worst delays happen when a provider has to keep calling back because the diagnosis, oxygen needs, pickup location, or receiving facility details are incomplete.
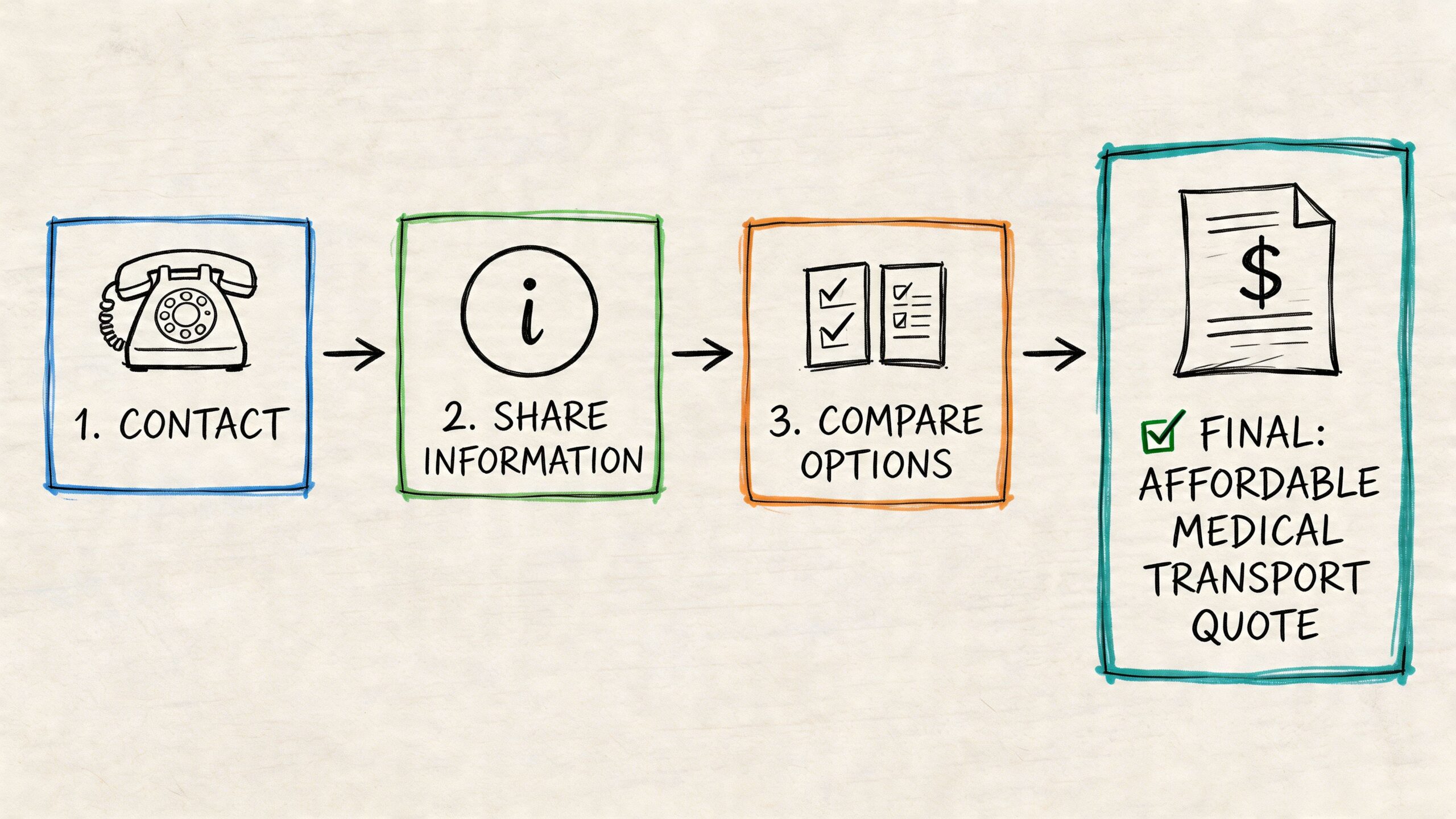
Gather these details before you call
Have this ready:
- Patient status including diagnosis, current stability, and any isolation concerns
- Current support needs such as oxygen, monitoring, medication infusion, or mobility limitations
- Origin and destination with facility names, unit, room, and contact person
- Receiving acceptance because many flights stall when the destination hasn’t formally agreed to take the patient
- Insurance information including payer name, member ID, and case manager contact if there is one
If the patient is bariatric, say that at the start. Don’t wait. It affects aircraft assignment immediately.
Questions that expose hidden costs
Some families ask, “What’s your price?” A better approach is to ask what the quote includes and what could still change.
Use questions like these:
- Is this quote all-inclusive? Ask specifically about both ground ambulances, airport handling, and medical crew.
- Are you the operator or a broker? Operators control their aircraft and crews directly. Brokers coordinate with outside operators.
- Will the aircraft come from another location first? Repositioning can affect scheduling and cost.
- What level of medical team are you assigning? The answer should match the patient’s condition.
- Who handles insurance paperwork? You want a provider that can support documentation, not just transport.
What can reduce cost without cutting safety
Not every patient needs a dedicated jet. For a stable patient, a commercial medical escort may be the more practical option. It won’t fit every case, but when it does, it can avoid paying for a full airborne ICU environment the patient doesn’t need.
Working with an owned-fleet operator can also simplify quoting because the company isn’t shopping your case around after the initial call. One example is Med Jets by Air Trek, which coordinates fixed-wing medical flights, escorts, and ground transport as part of a bedside-to-bedside transfer model.
What doesn’t work is choosing purely by the lowest number. A thin quote often becomes a thick invoice.
Frequently Asked Questions About Medical Flights
Can a family member fly with the patient
Sometimes, yes. It depends on aircraft configuration, patient acuity, and crew space. Ask early, because the answer affects aircraft choice.
Can pets travel on a medical flight
Sometimes they can, but this is operator-specific and mission-specific. Always disclose it before the quote is finalized so logistics can be checked properly.
What’s the difference between an operator and a broker
An operator controls the aircraft and crew. A broker arranges transport through operating partners. Either can be part of a legitimate transfer, but you should know which one you’re dealing with because it affects communication and responsibility.
How fast can a medical flight be arranged
It depends on patient readiness, hospital records, aircraft availability, crew assignment, and receiving-facility acceptance. Some cases move quickly. Others are delayed by paperwork rather than aviation.
Will membership programs or travel coverage pay for everything
Sometimes they help, but families shouldn’t assume a card or membership means every transfer is automatically covered. Check the transport criteria, exclusions, and authorization requirements.
What should I ask first on the phone
Start with this: “Given this patient’s condition, what transport mode is medically appropriate, and is your quote fully bedside-to-bedside?” That question usually gets you to the truth faster than asking for a price alone.
Medical plane cost is high because the service is complex, clinical, and time-sensitive. The good news is that the quote becomes much easier to judge once you know what belongs in it, what changes it, and what questions keep the process transparent.