If you searched air care international because someone you love needs an international medical flight, the key fact is this: Aircare International was founded in 1982 and trains over 3,500 crew members annually, but it is not a direct patient transport service. What you likely need instead is an air ambulance operator that can move a patient from one hospital, home, or care setting to another with medical staff and equipment onboard.
That distinction matters when you're under pressure. A hospital abroad may be asking for discharge plans. A family may be trying to bring someone home. A case manager may need a transport vendor that can handle paperwork, bedside pickup, and in-flight care without losing time. The name sounds close enough to what people expect that it's easy to head down the wrong path.
This guide is for that exact moment. It separates aviation safety and training companies from direct medical flight providers, then walks through what families and discharge planners need to know to arrange transport safely.
When a Medical Crisis Requires a Flight Home
A typical call starts with confusion.
Someone is hospitalized far from home. The treating team says the patient is stable enough to move, but not stable enough for a standard airline seat. A relative starts searching terms like "air care international," "medical flight home," or "international medevac." They aren't really looking for an aviation training company. They're looking for a safe way to move a patient.
What air care international actually does
Aircare International is a real and established aviation company. It was founded in 1982 and is a leader in medical and safety training for business aviation, not a direct patient transport service. It trains over 3,500 crew members annually through its Aircare FACTS® program, supporting flight departments rather than flying patients, according to the NBAA profile of Aircare International.
That means Aircare International operates in the broader safety ecosystem around aviation. It helps crews prepare for emergencies. It doesn't function as the company a family calls to move a patient from a hospital in one country to a receiving hospital in another.
Practical rule: If your immediate need is "How do I get my mother home from a hospital overseas?" you need an air ambulance provider, not a training vendor.
The question most families are really asking
Queries for this topic usually aren't about training volume or aviation support services. They're asking:
- Can my loved one fly safely right now?
- Who provides the nurse, paramedic, or physician onboard?
- How does hospital-to-hospital transfer work across borders?
- Who handles the timing when the patient can't sit upright or needs monitoring?
Those are air ambulance questions.
A direct patient transport provider coordinates the medical review, aircraft selection, bedside pickup, airport handling, and receiving-facility handoff. If the patient is time-sensitive, the issue isn't just transportation. It's whether the transport team can preserve the patient's condition during every handoff and during the flight itself.
That matters even more when families are up against the medical realities often described as the golden hour in urgent medical transport. Delays in choosing the right type of service can cost precious time.
What works and what doesn't
What works is narrowing the problem quickly.
If the patient needs oxygen, monitoring, a stretcher, medication management, or supervised transfer between facilities, start with an air ambulance coordinator. If a patient can travel on a commercial flight with minimal support, a medical escort may be enough. But if the family starts with the wrong type of company, hours can disappear into calls that never solve the actual transport problem.
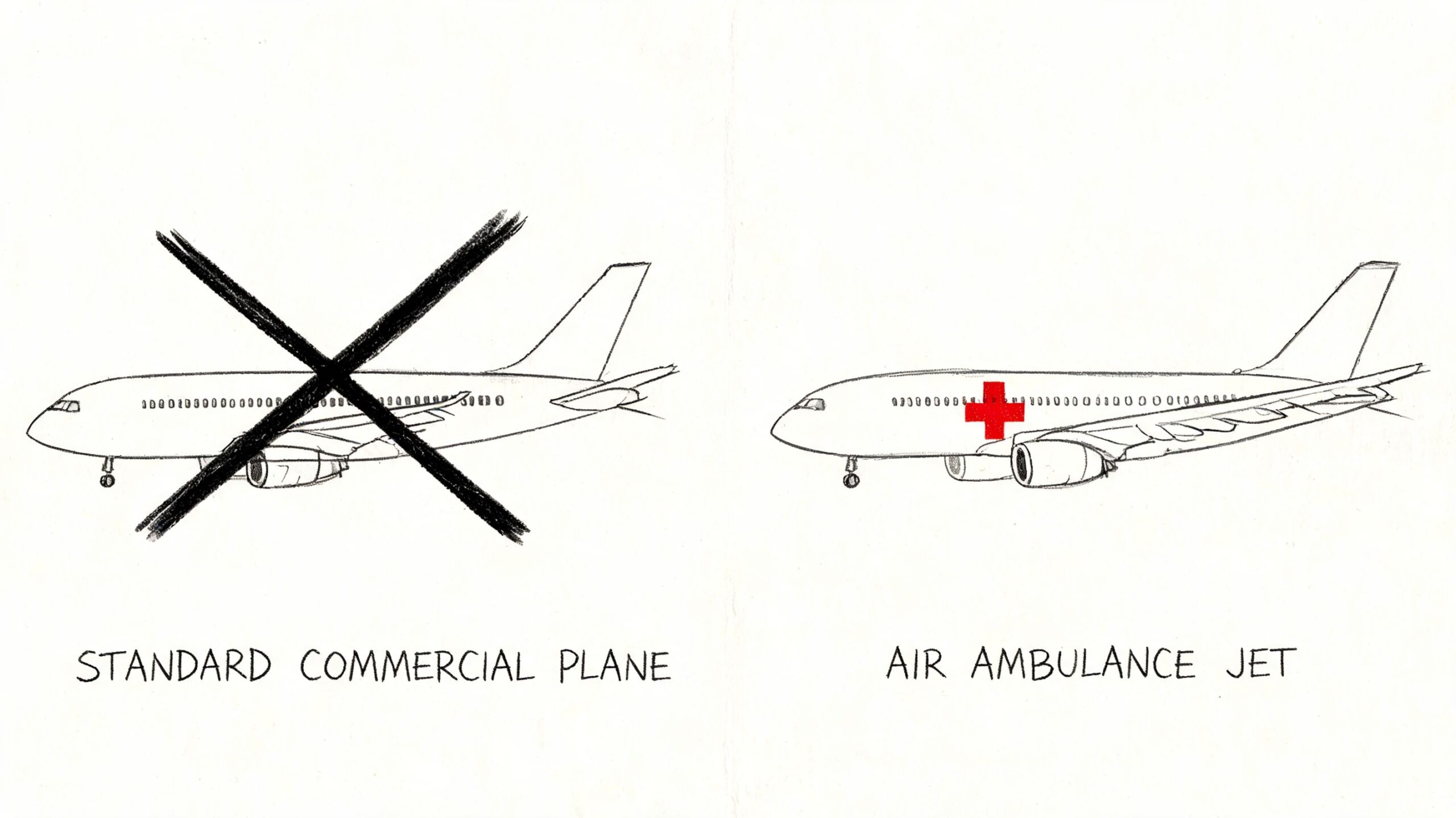
What doesn't work is assuming any aviation company with "air care" in the name can dispatch a medical aircraft.
Understanding Your Air Medical Transport Options
An air ambulance is best understood as an ICU in the sky, configured for the patient's condition and the trip. It's not just a jet. It's a clinical environment with a transport plan attached to it.
Some missions are urgent. Others are scheduled with careful timing around discharge, receiving-bed availability, and paperwork. Families often lump all of this under "medical flight," but the service types are different.
Two common mission types
The first is emergency medevac. That's used when a patient needs rapid movement because local resources are limited, the destination offers a higher level of care, or the current location isn't appropriate for ongoing treatment.
The second is medical repatriation or scheduled transport. In that situation, the patient may be stable enough to move, but still requires a stretcher, monitoring, medication support, or clinical supervision that a regular airline can't provide.
Why bedside-to-bedside matters
The best way to evaluate a transport service is to ask whether it handles the full chain of care.
A true bedside-to-bedside model usually includes:
- Clinical intake: The transport team reviews records, current stability, and travel tolerance.
- Aircraft planning: The operator selects an aircraft based on range, airport access, and patient needs.
- Ground coordination: Ambulances or medical vehicles move the patient to and from airports.
- Receiving coordination: The destination hospital, rehab center, or home-care setting is prepared before wheels up.
Families often focus on the aircraft because that's the visible part. The harder part is the chain around it. Miss one handoff, one document, or one receiving approval, and the mission can stall.
A smooth air medical mission usually looks calm from the outside because the coordinator solved problems before the family ever saw them.
Fixed wing or helicopter
For international transfers and longer domestic routes, fixed-wing aircraft are usually the practical choice. Helicopters have an important role, but they serve a different mission profile.
If you're comparing options, this overview of fixed-wing vs rotary-wing medical transport gives a useful framework for matching the aircraft type to the distance, urgency, and pickup environment.
What doesn't work in real cases
Commercial travel with wheelchair assistance is often mistaken for medical transport. That can work for a stable traveler who mainly needs mobility help. It doesn't work well for a patient who can't tolerate upright seating, needs suction, needs active monitoring, or may deteriorate in transit.
That's why the service model matters more than the label. "Medical flight" can mean several things. What you need is the option that fits the patient's actual condition.
Who Can Fly and What Care is Provided Onboard
The right question isn't "Can this patient fly?" It's "Can this patient fly safely, with the right team, equipment, and plan?"
That's a more useful clinical question because many patients who cannot travel commercially can still travel safely on an air ambulance.
Patients commonly considered for transport
Air ambulance providers regularly review transport for patients such as:
- Post-surgical patients who aren't ready for a standard airline seat and need pain control, wound oversight, or monitored transfer
- Stroke or neurologic patients who need positioning support, close observation, and careful handoff planning
- Cardiac or respiratory patients who may require oxygen, cardiac monitoring, or medication during flight
- Bariatric patients whose transfer requires the right loading method, cabin setup, and stretcher configuration
- Older adults or medically fragile travelers who may be stable but can't manage a standard airport and airline process safely
Not every patient is immediately flight-ready. Some need stabilization first. In practice, the transport physician or clinical team reviews current vitals, oxygen needs, medication timing, bleeding risk, airway concerns, and whether the patient can tolerate altitude and movement.
What onboard care should include
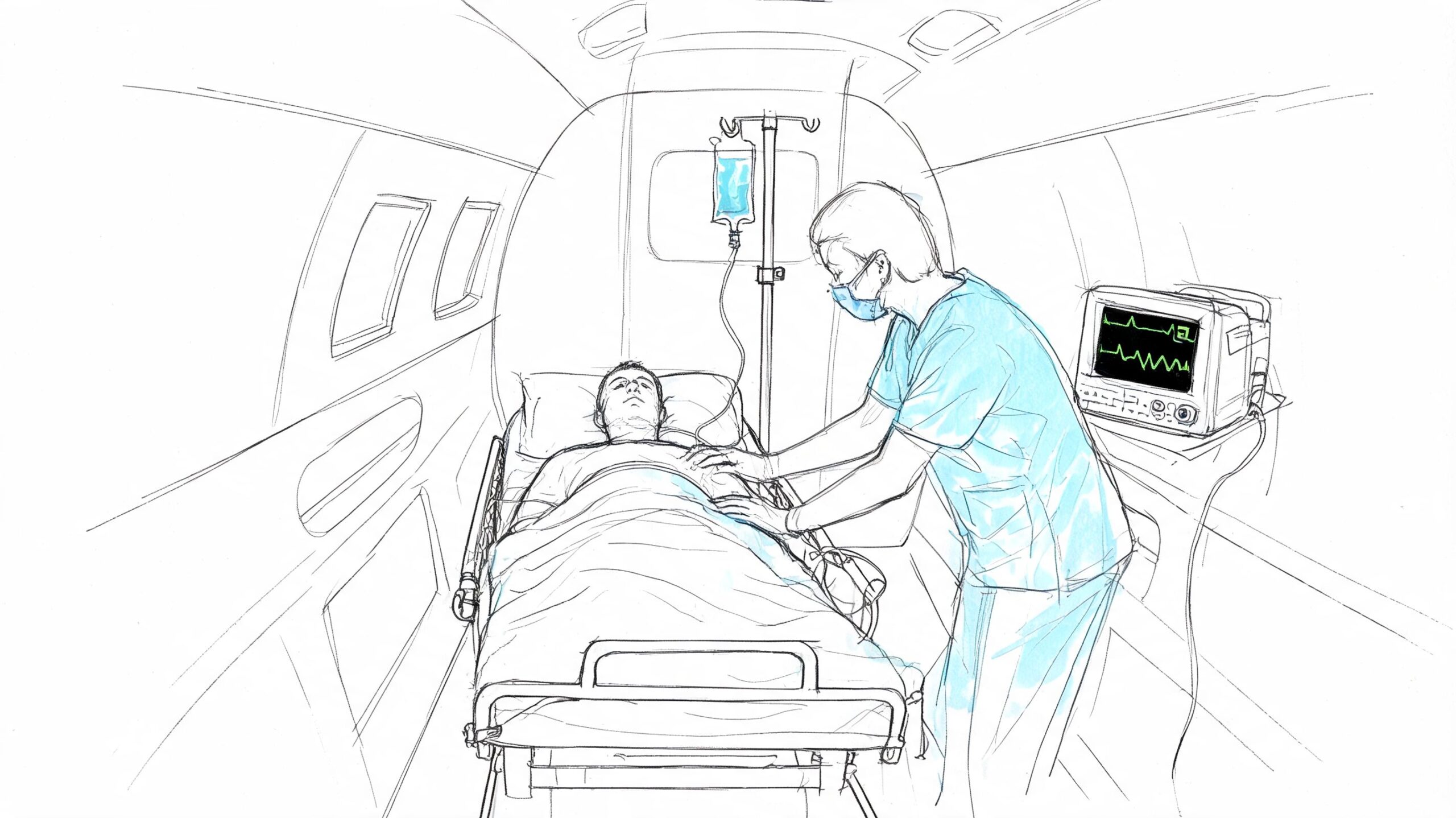
A capable provider doesn't just place a patient on a stretcher and hope the flight is uneventful. The crew should match the case.
That often means a combination of medical professionals such as flight nurses, paramedics, respiratory support personnel, or a physician when the case requires that level of care. The exact mix varies by mission. What matters is whether the crew can manage the patient's known risks and respond if the condition changes in the air.
Advanced air ambulances may also integrate telemedicine systems that transmit real-time vital signs to ground-based physicians, helping crews respond more quickly to in-flight events. That capability can help bridge the golden hour problem in in-flight medical care, especially when cabin pressure, distance, and isolation make clinical deterioration harder to manage.
When I evaluate a transport request, I don't only ask whether the patient is stable right now. I ask what could change three hours into the trip, and whether the aircraft team is equipped for that turn.
Language and documentation can also become a safety issue on international cases. Medication histories, allergies, diagnosis summaries, and consent forms can't be vague. If records cross borders or languages, it's worth reviewing the risks discussed in this article on understanding medical translation risks.
Training still matters, even when you're booking a transport
Families don't need a lecture on crew training in the middle of a crisis, but they do need the result of that training. Teams that rehearse emergencies in realistic environments tend to perform more reliably under pressure.
Later in your vetting process, ask how the crew trains for cabin emergencies, patient deterioration, and handoff failures. You don't need marketing language. You need clear answers.
A short look at how onboard care works can help families picture the environment more clearly:
From First Call to Safe Arrival The Logistics
The first call is rarely neat. A daughter is standing in a hospital hallway. A discharge planner has partial records. A spouse is trying to answer questions while also calling relatives. Good coordination starts by reducing noise.
A transport coordinator usually begins with three essentials: who the patient is, where the patient is now, and what the treating team says about current condition. From there, the process becomes more structured.
How the mission usually unfolds
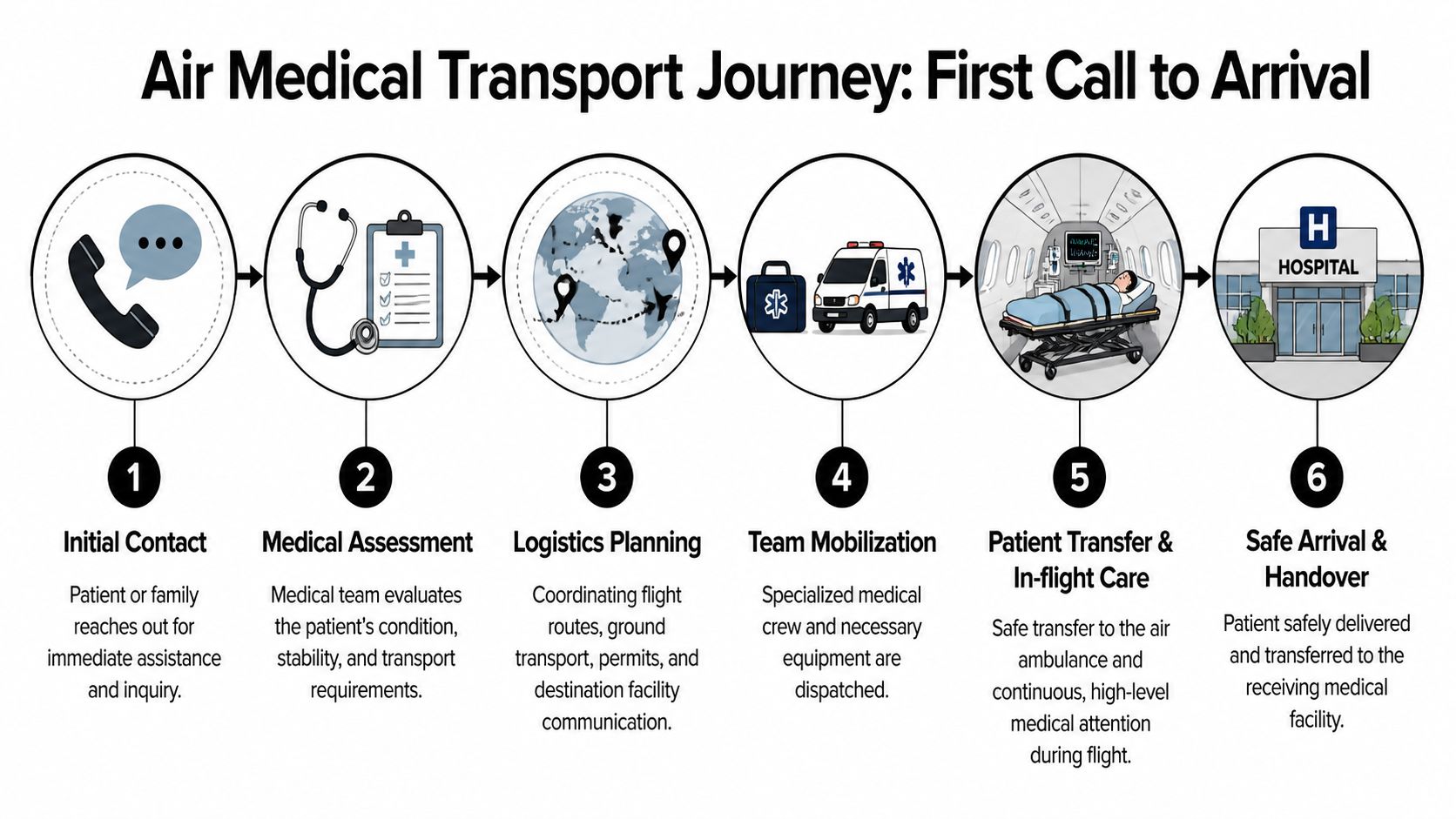
Once records arrive, the clinical team reviews whether the patient is fit for transport and what support is needed onboard. That review affects nearly everything that follows, including aircraft choice, crew composition, airport selection, timing, and ground transfer setup.
Then the logistics side takes over in parallel. Someone secures the flight plan. Someone confirms the sending facility can release the patient at the expected time. Someone confirms the receiving hospital or destination facility is ready. Ground ambulances must align with aircraft arrival windows, not just approximate them.
A realistic family view of the process
From the family's perspective, the experience should feel like this:
- You provide records and contact names. The coordinator asks for treating physician details, current medications, and destination preferences.
- The provider reviews medical suitability. If the patient isn't ready, you hear that plainly.
- The transport team builds the route. That includes airport choices, ground vehicles, and handoff timing.
- Paperwork is assembled. Depending on the case, that may include identity documents, release forms, medical summaries, and receiving acceptance.
- The patient is moved with supervision. Each transition is planned, not improvised.
- The receiving team gets report. The handoff should be direct and clinically useful.
The best coordinators don't just arrange aircraft. They close gaps between hospitals, airports, families, insurers, and clinicians.
Where missions usually get delayed
Delays usually don't come from one dramatic issue. They come from small misses that stack up.
Common trouble spots include:
- Incomplete records: Missing medication lists, imaging summaries, or physician notes slow medical review.
- Unclear destination acceptance: A family may want a specific hospital before that hospital has accepted the transfer.
- Passport or identity issues: International movement often stalls if documents aren't checked early.
- Ground timing gaps: The aircraft may be ready while the ambulance or hospital release process isn't.
When providers handle this well, the family feels informed without being overloaded. One option in this space is Med Jets by Air Trek, which coordinates end-to-end patient transfers including medical flights, medical escorts, and ground transport as part of a single transport process.
That kind of unified coordination matters because every extra handoff creates another chance for error.
Navigating Air Ambulance Costs and Insurance
Families usually ask about cost after they've asked whether the patient can fly. That's understandable. They need a plan that is both medically safe and financially possible.
The hard part is that there isn't one universal air ambulance price. The mission has to be built first. Only then can anyone explain the cost structure accurately.
What drives the cost of a mission
The wider aviation services industry includes companies with substantial revenue. Some B2B providers are estimated at over $60 million annually, but that doesn't tell a family what a single patient mission will cost. The practical issue is understanding the line items and why they exist, as reflected in this industry context on Aircare International and related aviation services.
A transport quote usually reflects factors like:
- Distance and route complexity: International legs, airport access, and positioning all affect planning.
- Aircraft type: The cabin setup must match the patient and mission range.
- Clinical acuity: A patient who needs higher-level monitoring or a larger crew changes the medical side of the mission.
- Ground services: Ambulances at both ends, and sometimes specialized loading support, are part of the total picture.
- Timing: Urgent launches and tightly timed discharges are operationally different from flexible scheduled moves.
How to talk to insurance without losing time
Insurance can help, but families often expect broader coverage than the policy provides. Health insurance, travel insurance, employer assistance programs, and membership products all behave differently.
If you're sorting through public coverage terms as part of a broader care plan, this overview of understanding Medicare and Medicaid differences can help you ask cleaner questions before you call.
When you speak with an insurer, ask for specifics:
- Medical necessity: What documentation does the insurer require from the sending physician?
- Covered mode of transport: Is air ambulance covered, or only commercial repatriation under certain conditions?
- Network or authorization rules: Does the insurer require prior approval or designated vendors?
- Destination rules: Will they cover transfer to the nearest appropriate facility, or to the patient's home region?
Ask the insurer to state coverage conditions in writing. Verbal reassurance during a stressful call isn't enough.
Documents that usually matter
Keep these ready as early as possible:
- Treating physician statement
- Recent clinical notes
- Medication list
- Passport or identity documents
- Insurance card and policy details
- Receiving facility contact information
If you want a plain-language breakdown of the moving parts, this guide to air ambulance pricing factors and medical flight costs is a useful starting point.
What doesn't work is focusing only on the top-line quote. The right question is whether the quote includes the full mission the patient needs.
A Checklist for Evaluating Air Ambulance Companies
Families often compare providers too late. They look at speed first, then price, and only afterward ask about safety, crew quality, or who has control of the aircraft. That's backwards.
A better approach is to evaluate the operator as if you're hiring a clinical transport partner, because that's exactly what you're doing.
Air Ambulance Provider Evaluation Checklist
| Criteria | What to Look For | Why It Matters |
|---|---|---|
| Accreditation and inspections | Ask what clinical or aviation oversight applies, and whether the company can explain it clearly | Outside review doesn't guarantee perfection, but it helps verify that the operator follows defined standards |
| Medical crew model | Ask who flies on cases like yours, how staffing is chosen, and who makes clinical decisions | The right crew mix determines whether the team can manage deterioration, medications, oxygen, and handoffs |
| Aircraft access and control | Ask whether the provider owns, operates, or brokers the aircraft, and who controls dispatch decisions | More control usually means fewer communication gaps and fewer surprises on timing |
| Bedside-to-bedside coordination | Confirm the provider handles ground ambulances, records flow, hospital communication, and final handoff | Families shouldn't have to stitch together five vendors during a medical crisis |
| Experience with your case type | Ask about stroke, post-surgical, respiratory, bariatric, pediatric, or international transfer experience | A provider may be competent overall but still not be the right fit for a specific clinical profile |
| Communication style | Notice whether they answer direct questions directly, including what they can't do | Clear communication is a safety feature, not just a customer service preference |
| Training standards | Ask how crews rehearse emergencies, handoffs, and cabin scenarios | Top-tier aviation crews achieve over 90% retention in emergency procedure proficiency through immersive simulation training, which is a meaningful safety signal according to Aircare International's training overview |
Questions worth asking on the first call
Some questions reveal a lot very quickly:
- Who reviews the medical records before you accept the case?
- Will you coordinate both ground legs, or do I need separate ambulances?
- What happens if the patient worsens before departure?
- Who gives report to the receiving facility?
- Are you speaking as the direct operator or as a broker?
A provider that answers those questions cleanly is usually easier to work with when the case gets complicated.
What families often miss
Many people focus on the aircraft cabin photos. That's understandable, but it's not enough.
The stronger predictor of a smooth mission is usually whether the company can manage exceptions. Delayed discharge. Changed oxygen requirement. Receiving bed moved. Border document issue. Family member added. Those are the moments that test a provider.
Safety isn't just equipment. It's what the team does when the original plan stops being the plan.
Your Action Plan and Common Questions Answered
When people search air care international, they're often trying to solve an immediate medical transport problem. By this point, the path is clearer. If you need a patient moved, focus on direct air ambulance providers and start gathering the information they'll need.
A simple action plan
- Get the current clinical picture: Ask the treating team for diagnosis, current stability, oxygen needs, medication list, and whether the patient is fit for transfer.
- Identify the destination: Confirm whether the patient is going to a hospital, rehab center, skilled nursing facility, or home with services.
- Collect documents early: Passport, insurance details, treating physician contact, and receiving facility information should be ready before you start comparing options.
- Ask transport-specific questions: Don't ask only "How fast can you fly?" Ask who provides onboard care, who handles ground transport, and who coordinates the final handoff.
- Request a full mission explanation: You want to know what's included, what isn't, and what could delay departure.
Common questions
Can a family member fly with the patient
Sometimes yes. It depends on the aircraft setup, patient condition, weight and balance, and the clinical space required for the crew to work safely.
Can a patient fly on oxygen or monitoring
Often yes, if the transport provider is equipped and the case has been medically reviewed in advance. The key issue is not whether the patient has a diagnosis. It's whether the flight team can manage the likely risks.
Is this the same as buying a seat on a commercial plane
No. A medical transport mission is built around clinical supervision, equipment, transfer handling, and coordination across multiple handoffs.
Can pets come too
Some providers can accommodate this on certain missions, but it has to be discussed early because it affects planning, paperwork, and cabin arrangement.
If you're making decisions under pressure, keep it simple. Confirm the patient's readiness, choose the right type of provider, and insist on clear answers. A calm, experienced transport team can take a chaotic situation and turn it into a manageable one.
If you need to arrange an international or domestic medical flight, contact a direct air ambulance provider that can review the case, explain the transport options, and coordinate the mission from first call to safe arrival.