When a hospital team tells you an air ambulance may be the fastest way to move someone you love, the decision can feel brutally simple. Say yes, move fast, hope for the best. Then the fear hits. You search for terms like medical flight crash, and suddenly you're reading about wreckage, investigations, and worst-case scenarios.
That fear is understandable. It also helps to know that air medical risk isn't random. It sits on a spectrum shaped by aircraft type, weather, crew judgment, maintenance discipline, cabin design, and the pressure built into emergency care. Families and case managers usually can't control the mission itself, but they can ask questions that reveal whether an operator runs on disciplined systems or on hope.
The right way to think about a medical flight is not “safe” versus “unsafe.” The useful question is whether the operator manages known risks well, and whether the clinical benefit of flying outweighs the aviation exposure on that specific day.
Understanding Medical Flight Risk
A medical flight is not a commercial airline trip with a stretcher in the back. The mission profile is different from the start.
An air ambulance may launch on short notice, fly into changing weather, use smaller airports, or land in environments that aren't as forgiving as major commercial hubs. The crew also has to balance flight operations with active patient care. That combination changes the risk picture.
A widely cited U.S. safety review found that 55 EMS aircraft accidents occurred between January 2002 and January 2005, causing 54 fatalities, and noted that this level of activity had not been seen since the 1980s. The same review reported 41 helicopter accidents and 14 airplane accidents during that period, which shows both aircraft types were involved, with helicopters accounting for the larger share of incidents in that review (EMS aircraft accident review).
Why medical missions differ from airline flying
Commercial airlines operate in a tightly structured system built around scheduled routes, large airports, and broad operational margins. Medical transport crews often work inside narrower margins.
That doesn't mean medical flying is reckless. It means the variables are different:
- Time pressure matters: A patient may need faster access to surgery, specialty care, or a higher-acuity hospital.
- Route flexibility matters: The aircraft may need to go where the patient is, not where conditions are easiest.
- The cabin is a treatment space: Clinicians aren't just monitoring. They may be ventilating, infusing medication, or managing instability during transport.
Risk is managed, not erased
The most useful safety mindset is practical. Every flight involves exposure. Strong operators reduce that exposure through conservative planning, equipment standards, crew coordination, and refusal to launch when conditions don't support a safe mission.
Practical rule: If an operator talks only about speed and availability, ask more questions. Safety-minded providers also talk about screening, limitations, and reasons they might decline or delay a flight.
Families often want certainty. Aviation can't offer that. What it can offer is disciplined risk control. That's what separates a well-run mission from a vulnerable one.
Common Causes of Air Ambulance Accidents
Most air ambulance accidents don't come from a single dramatic failure. They come from a chain. One weak decision, one missed maintenance issue, one weather assumption, one rushed handoff. Then the chain tightens.
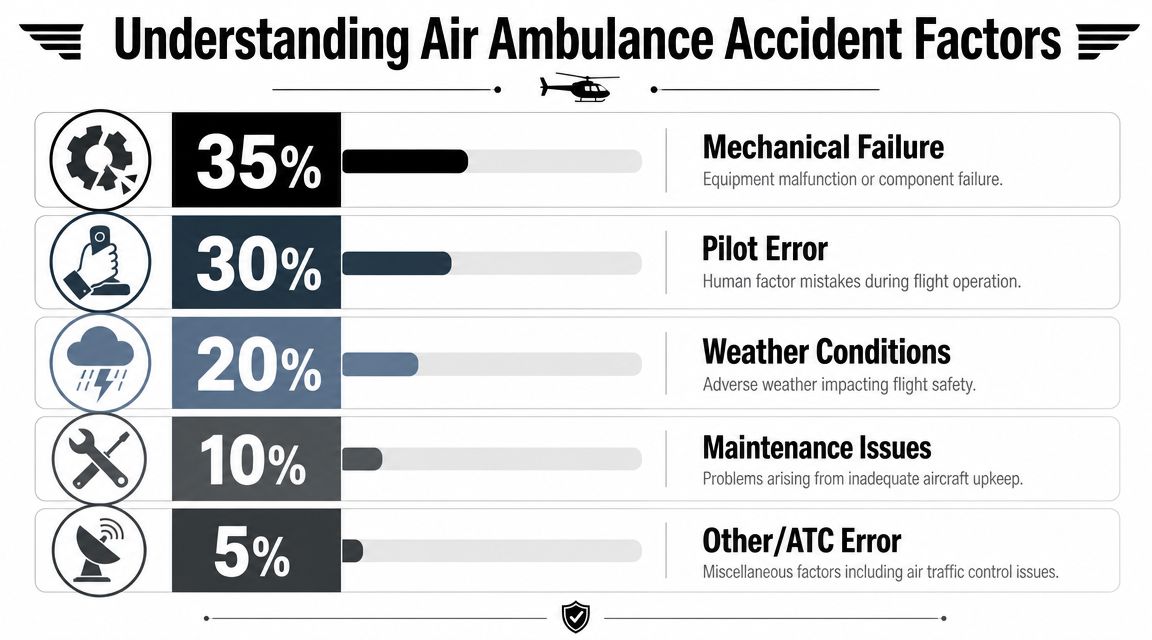
Aviation-accident analyses consistently identify pilot error, mechanical error, and weather as leading causal categories, with one summary citing mechanical errors in 22% of crashes and inclement weather in 12% of crashes (aviation accident causes summary).
How the accident chain usually forms
The categories sound simple, but real flights are messy. A pilot may accept a marginal launch because the patient needs specialty care. The weather may still meet minimums, but only barely. At the same time, a small equipment issue may increase workload in the cockpit. Then a routine task becomes a high-stress one.
That's why “pilot error” is often too shallow an explanation. Sometimes the pilot made the last wrong move. But the system may have set up that move with pressure, poor dispatch filtering, weak crew challenge culture, or maintenance drift.
The three failure points that matter most
| Risk area | What it looks like in practice | What tends to help |
|---|---|---|
| Mechanical problems | Component failure, unresolved discrepancies, configuration mistakes | Strong maintenance control, documented write-ups, no pressure to fly with “watch items” |
| Weather exposure | Deteriorating visibility, cloud layers, icing risk, crosswinds | Conservative thresholds, real-time updates, willingness to cancel |
| Human performance | Missed cues, rushed decisions, poor communication, fixation | Crew resource management, standard callouts, disciplined go/no-go review |
Weather rarely acts alone. Trouble usually starts when a crew keeps going after conditions stop matching the original plan.
A family member won't see most of this from the bedside. But an operator's culture shows up in simple answers. If they can't explain how they handle maintenance discrepancies, changing forecasts, or cockpit cross-checks, that's not a paperwork problem. It's a safety signal.
How Safety Is Engineered Into Medical Jets
Avoiding a crash is only part of aviation safety. The other part is survivability. In a medical flight crash, cabin design and restraint design can determine whether occupants walk away, suffer serious injury, or don't survive.
A medical review of aircraft accidents explains that crash survivability is driven by acceleration magnitude, direction, duration, and onset rate, and that occupant position, restraint, and support materially change injury risk. It states that when crash forces exceed human tolerance by 2x, survival is unlikely, while forces below that threshold depend heavily on the specific setup of the cabin and restraints (medical review of aircraft accidents).
Why cabin layout matters
People often focus on the aircraft model. That matters, but interior configuration matters too. A medical cabin isn't just a place to fit equipment. It has to control what happens to the patient, clinician, and family member if the aircraft stops violently.
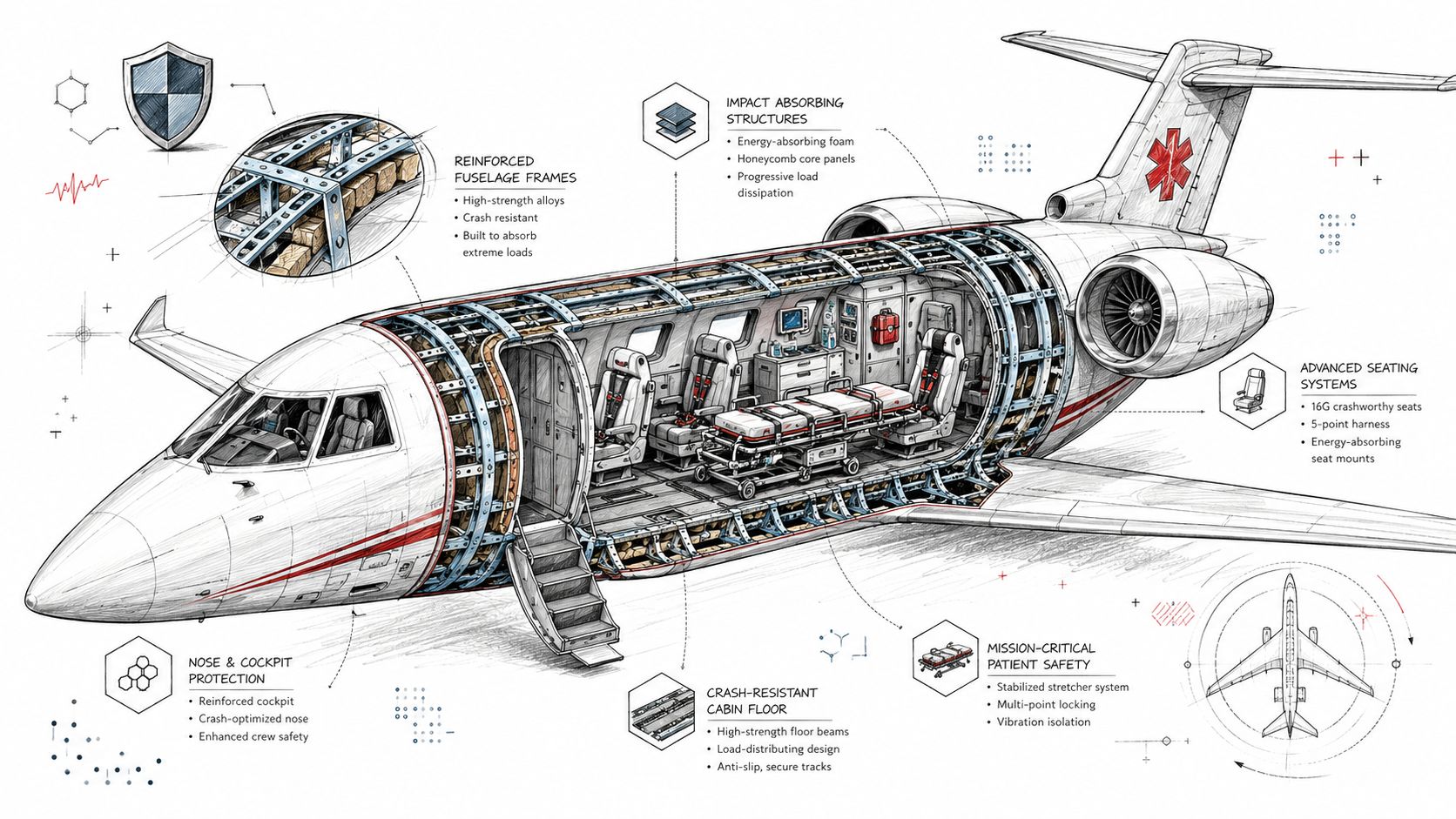
The most important design elements include:
- Restraint systems: Seats, belts, and harnesses must limit harmful movement.
- Crashworthy stretchers: The patient support system has to stay attached and distribute force appropriately.
- Cabin orientation and support points: The direction the body faces and what supports it changes how force travels through the spine, head, and chest.
Why fixed-wing missions can differ operationally
For many interfacility transfers, fixed-wing aircraft offer a different operational profile than rotor-wing aircraft. They typically use airport infrastructure rather than improvised landing zones, and their cabin space and mission planning process often fit longer transports well. If you want a plain-language overview of that format, this explanation of fixed-wing air ambulance transport is a useful starting point.
That still doesn't make any aircraft automatically safer in every case. It means the engineering choices, airport environment, and mission type need to match the patient's needs.
Good safety design isn't cosmetic. In a survivable impact, the stretcher mount, seat restraint, and occupant orientation may matter as much as the airframe.
When evaluating a provider, ask what they've done inside the cabin, not just what logo is on the tail.
The Investigation and Regulatory Process
When a medical flight crash happens, the aftermath follows a disciplined process. That matters for two reasons. First, families deserve answers grounded in evidence. Second, every serious accident should produce lessons that prevent recurrence.
What happens after the crash
The sequence usually moves through several stages:
Initial response
Emergency teams secure the site, care for survivors, and protect evidence.Evidence collection
Investigators gather maintenance records, crew information, weather data, air traffic communications, and onboard recording devices if available.Reconstruction and analysis
Specialists map the event sequence, review aircraft systems, and examine operational decisions.Reporting and recommendations
The investigation identifies probable cause and contributing factors, then issues safety recommendations.
For readers trying to understand how technical crash analysis works in litigation or major investigations, an accident reconstruction expert witness can help explain how physical evidence, flight path, impact dynamics, and records are interpreted.
Why missing data is a serious safety issue
One of the most troubling operational signals is not just a crash itself, but an avoidable loss of investigative data. Reporting on the Philadelphia air-ambulance crash said the aircraft's cockpit voice recorder was reportedly nonfunctional for years, and the NTSB found the tape had no usable audio after cleaning and repair. That kind of gap limits post-crash reconstruction and raises hard questions about oversight of mandatory safety equipment (report on the Philadelphia cockpit voice recorder issue).
The NTSB investigates accidents and identifies probable causes. The FAA regulates operations, standards, and compliance. Families don't need to master agency roles, but they should understand this: the system works best when operators treat recorders, logs, inspections, and reporting requirements as living safety tools, not box-checking exercises.
How Reputable Operators Actively Mitigate Risk
The strongest predictor of safety is usually not marketing, fleet paint, or a polished brochure. It's operational culture. Reputable operators build systems that make the safe decision easier, even when that decision costs time, revenue, or convenience.
A tragic example of why this matters came from the Philadelphia crash reporting discussed earlier. A cockpit voice recorder that was reportedly nonfunctional for years doesn't point to bad luck. It points to a systems failure around oversight, maintenance accountability, or both.
What a strong safety culture looks like
You can often recognize a mature operation by how it talks about limits. Good operators are comfortable saying no.
They also tend to rely on a few essential elements:
- Conservative launch decisions: They won't let urgency erase weather, maintenance, or crew-rest concerns.
- Open reporting: Crew members can flag hazards, mistakes, or equipment issues without fearing punishment for speaking up.
- Standardized briefings: Pilots, medical crew, dispatch, and maintenance work from shared checklists and common language.
Process beats personality
Families sometimes assume safety comes down to having a “great pilot.” Skilled pilots matter, but personality is not a system. A fatigued crew in a weak organization can still make bad decisions.
What works better is a layered process:
| Safety control | What it prevents |
|---|---|
| Maintenance discipline | Deferred problems turning into in-flight emergencies |
| Crew resource management | One person's error going unchallenged |
| Mission screening | Launching into conditions that don't support a safe outcome |
| Equipment verification | Discovering too late that critical gear is missing or inoperative |
An operator should also be able to explain how medical equipment is managed, secured, and checked before departure. A practical reference point is the range of aeromedical supplies used in patient transport, because every item in the cabin has to support care without compromising safety.
This is also the right place to mention one provider example without turning it into a sales pitch. Med Jets by Air Trek provides medical flights and medical escorts, which is relevant because some patients need a dedicated air ambulance while others may be safer and more appropriate with medically managed escorted transport. That kind of mode selection is part of risk management, not just logistics.
The safest operators don't promise that nothing will go wrong. They show you how they catch problems before those problems reach the runway.
Critical Questions to Ask Your Air Ambulance Provider
The most useful conversation is not “Can you fly today?” It's “Why is flying the right transport choice for this patient today, and how do you control the risks of doing it?”
That question matters because one of the biggest unresolved issues in public understanding is when a medical flight is safer or more appropriate than ground transport. Risk varies by aircraft type, mission, and weather, so the critical decision is not just availability. It's what clinical benefit justifies the aviation risk on that specific transfer (discussion of air versus ground trade-offs in medical transport).
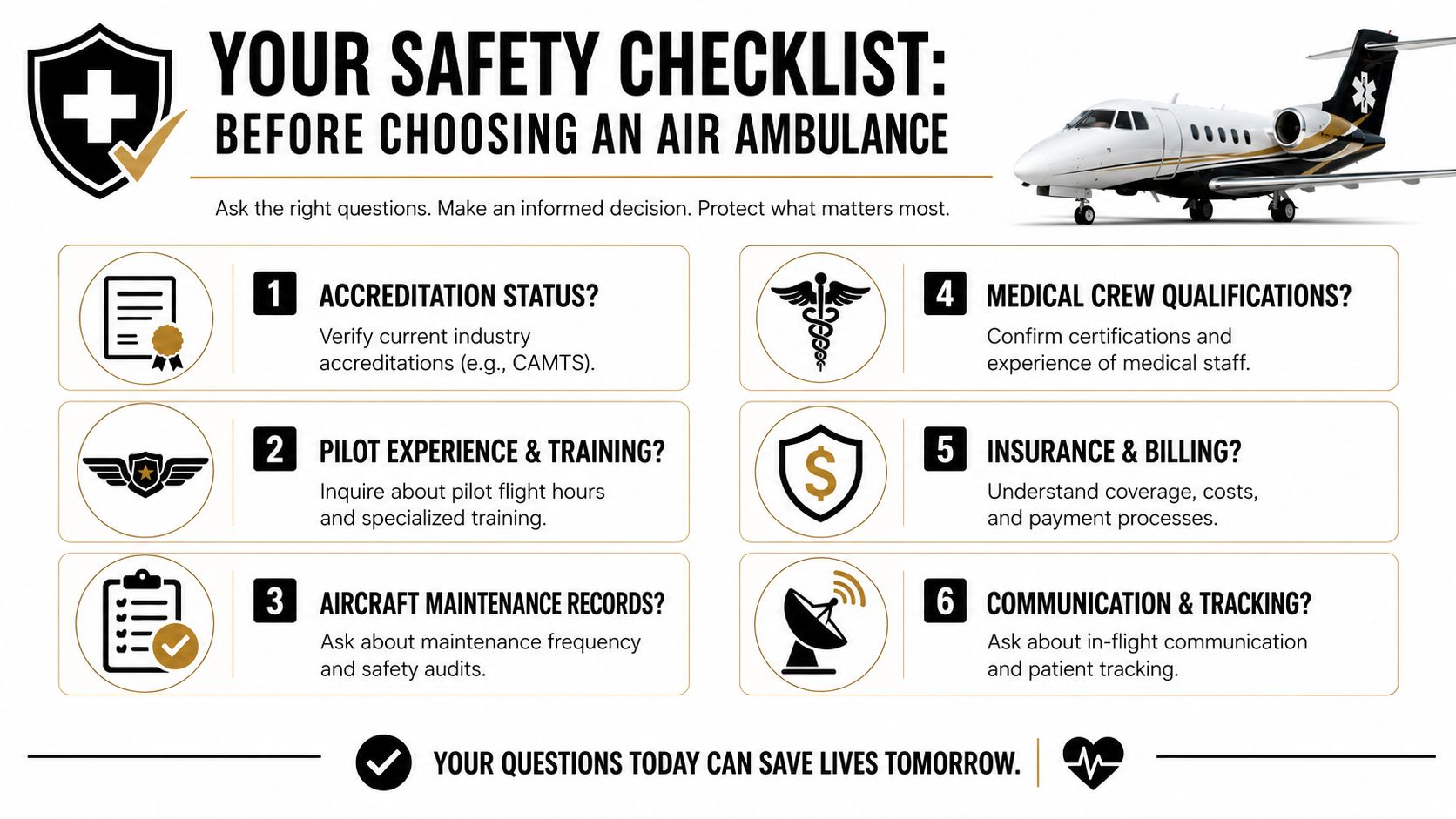
A quick visual checklist helps families organize that conversation.
Start with the transport decision itself
Before asking about aircraft, ask about necessity.
- Why is air transport clinically better than ground today? A serious provider should tie the answer to time, distance, patient acuity, required interventions, or destination capability.
- What would make you delay or decline this mission? You want to hear clear limits, not vague reassurance.
- Is this mission better suited to fixed-wing, helicopter, or medical escort transport? Different platforms solve different problems.
Families who want to understand how crews prepare for these transports can review the basics of patient transport training for medical aviation teams.
Later in your review process, it can help to watch this overview and listen for whether the provider's language centers safety, preparation, and clinical fit rather than speed alone.
Questions that reveal real safety commitment
Use these as direct prompts, not as a quiz show:
- Tell me about your maintenance program. Ask who performs maintenance, how discrepancies are documented, and what happens when an aircraft has an unresolved issue.
- How do you make go or no-go weather decisions? Listen for objective standards and crew authority to cancel.
- Who has final authority to stop a mission for safety reasons? The answer should not be muddled.
- How are patients and equipment secured in the cabin? This tells you whether the operator understands crash survivability and cabin discipline.
- What qualifications do your clinical crew hold for this type of patient? The medical challenge during transport matters as much as the flying.
- How do you communicate with the sending hospital, receiving hospital, and family during the transfer? Good communication reduces rushed decisions and handoff errors.
Answers that should concern you
A few responses should make you pause:
| Concerning answer | Why it matters |
|---|---|
| “We can usually make it work.” | May signal mission pressure overriding limits |
| “Our pilots handle that.” | Can indicate weak team-based safety culture |
| “Maintenance is standard.” | Too vague to show real process control |
| “We've never had an issue.” | Overconfidence is not the same as transparency |
Ask for specifics, not slogans. A careful operator can describe process, limitations, and how decisions get made under pressure.
A Guide to Safe Medical Flight Choices
A medical flight crash is every family's fear. The better response to that fear is not panic and not blind trust. It's informed scrutiny.
The right provider should be able to explain why air transport is justified, what aircraft and crew setup fits the patient, how maintenance and weather decisions are handled, and how the cabin protects the patient if something goes wrong. Safety lives in those details.
You don't need to become an aviation investigator to make a sound decision. You need to listen for discipline. Clear answers. Defined limits. A willingness to delay, decline, or recommend a different transport mode when the risk-benefit balance doesn't support flight.
That's how safe choices are made. Not by assuming every medical flight is dangerous, and not by assuming every provider is equally prepared.
If you're arranging transport now, speak with a trusted flight coordinator and ask the hard questions early. The safest operators won't be bothered by them. They'll expect them.
Frequently Asked Questions About Medical Flight Safety
Are helicopters more dangerous than medical jets
Risk depends on mission type, weather, landing environment, and operational pressure. Helicopters often work in more variable settings, while fixed-wing aircraft usually operate through airport infrastructure. The better question is which aircraft fits the mission safely.
Is a medical flight always safer than driving
No. Sometimes air transport offers a clear clinical advantage. Sometimes ground transport may be more appropriate. The decision should be based on patient condition, distance, time sensitivity, weather, and operational conditions that day.
What should I ask first if I'm worried about a medical flight crash
Start with this: Why is flying medically necessary today, and what would make you decline the mission? That question gets past sales language and into risk management.
Do cabin restraints and stretcher systems really matter
Yes. In any survivable impact, restraint design, stretcher security, and cabin orientation affect injury outcomes. These are core safety features, not optional upgrades.
What if an operator says safety equipment problems don't affect the mission
That should concern you. Required safety equipment and documented maintenance issues tell you whether the operator treats compliance as part of real safety practice.
Can families request a different transport option
Often, yes. Depending on the clinical situation, options may include a dedicated fixed-wing air ambulance, a rotor-wing transfer, or a medically managed escort model. Asking about alternatives is appropriate and often wise.
If you need help evaluating transport options for a specific patient, contact a qualified air medical coordinator and ask for a mission-by-mission risk explanation before you consent.