A transfer can fall apart even when every individual clinician is competent.
A daughter is trying to move her father from a community hospital to a specialty center. The sending team says records were faxed. The receiving team says they only got part of the chart. The medication list has one version in the nurse's notes and another in the discharge packet. The transport crew is waiting on confirmation of oxygen needs. Nobody is careless, but the patient still sits in the middle of a broken relay.
That's where patient continuity of care stops being an abstract healthcare phrase and becomes a safety system. In complex transfers, especially long-distance moves and air ambulance coordination, continuity means the patient's story, risks, plan, equipment needs, and family instructions travel intact from bedside to bedside. When that handoff is solid, care feels organized. When it's weak, small gaps turn into delays, duplicated work, and avoidable danger.
What Is Patient Continuity of Care
Patient continuity of care is often misunderstood as “seeing the same doctor over time.” That matters, but it's only part of the picture. In real-world transfers, continuity is the quality of the handoff.
If you're arranging a move for a medically fragile loved one, continuity works like a medical passport. It carries the patient's diagnosis, recent changes, medication list, allergies, baseline function, goals of care, pending tests, family contacts, and practical constraints into the next setting. Without that passport, each new team has to rebuild the case under pressure.
The World Health Organization's continuity framework is useful here because it shifts the focus away from a single relationship and toward reliability across settings. As summarized in the WHO practice brief, continuity isn't just about staying with one doctor. It also depends on reliable records, medication reconciliation, and coordinated planning across settings, which is why families and case managers should treat it as a handoff quality issue during medical transport and other complex transitions in care (WHO continuity and coordination brief).
What families usually mean when they ask about continuity
Most families aren't asking for theory. They're asking practical questions:
- Who has the current plan
- Who is responsible during the move
- Will the receiving team know what changed today
- What happens if the patient declines in transit
- Who do we call if the paperwork doesn't match
Those are continuity questions.
Continuity fails long before anyone says the transfer failed. It fails when one team assumes another team has the information.
What continuity looks like in practice
A strong transfer usually includes:
- One current medication list that everyone is using
- A clear clinical summary that explains why the patient is moving
- Confirmed acceptance from the receiving clinician or facility
- Transport instructions matched to the patient's condition and equipment needs
- A family communication plan so updates don't get lost or contradicted
When people understand patient continuity of care this way, they stop treating transport as a travel task and start treating it as a coordinated clinical handoff.
Why Seamless Care Transitions Save Lives
Fragmented care isn't just frustrating. It changes outcomes.
In a study of Medicare patients, researchers found that when hospitalists' schedules allowed for greater continuity of care, patients had significantly lower mortality rates, fewer 30-day hospital readmissions, and were more likely to be discharged home instead of to other facilities (AHA summary of the Medicare continuity study).
That finding matters because the danger point isn't only the illness itself. It's the moment responsibility changes hands. A transfer from one hospital to another, a discharge to rehab, or a move from ICU transport to receiving-floor admission all create opportunities for the care plan to fracture.
The baton can't be dropped
A patient transfer works like a relay. The patient is the baton, but the essential exchange is information, accountability, and timing.
If the sending team leaves out a new medication, the receiving team starts with a flawed picture. If transport arrives before acceptance is finalized, the patient waits in limbo. If the family hears one plan from one clinician and another from a discharge office, trust erodes immediately.
A broader evidence review reinforces that continuity has consequences beyond convenience. An extensive review covering 25 studies found that greater continuity of care has a statistically significant protective effect on all-cause mortality and is also associated with fewer avoidable hospitalizations, lower costs, and higher patient satisfaction (continuity evidence review from ACT Center).
Why this matters during transport
Transport compresses time. Decisions happen faster, communication channels multiply, and everyone is working from a moving target if the chart isn't current. That's why the handoff itself has to be designed, not improvised.
A practical support tool in this environment is patient messaging. If your team is evaluating communication workflows, this roundup of research on patient engagement texting is useful for thinking about reminders, follow-up prompts, and reducing missed communication after transitions.
Practical rule: A transfer is safest when the receiving team knows the patient before the patient arrives.
The Three Pillars of Effective Care Continuity
The cleanest way to evaluate continuity is to look at three pillars. If one is weak, the transfer becomes harder to trust. If two are weak, the team is usually doing damage control.
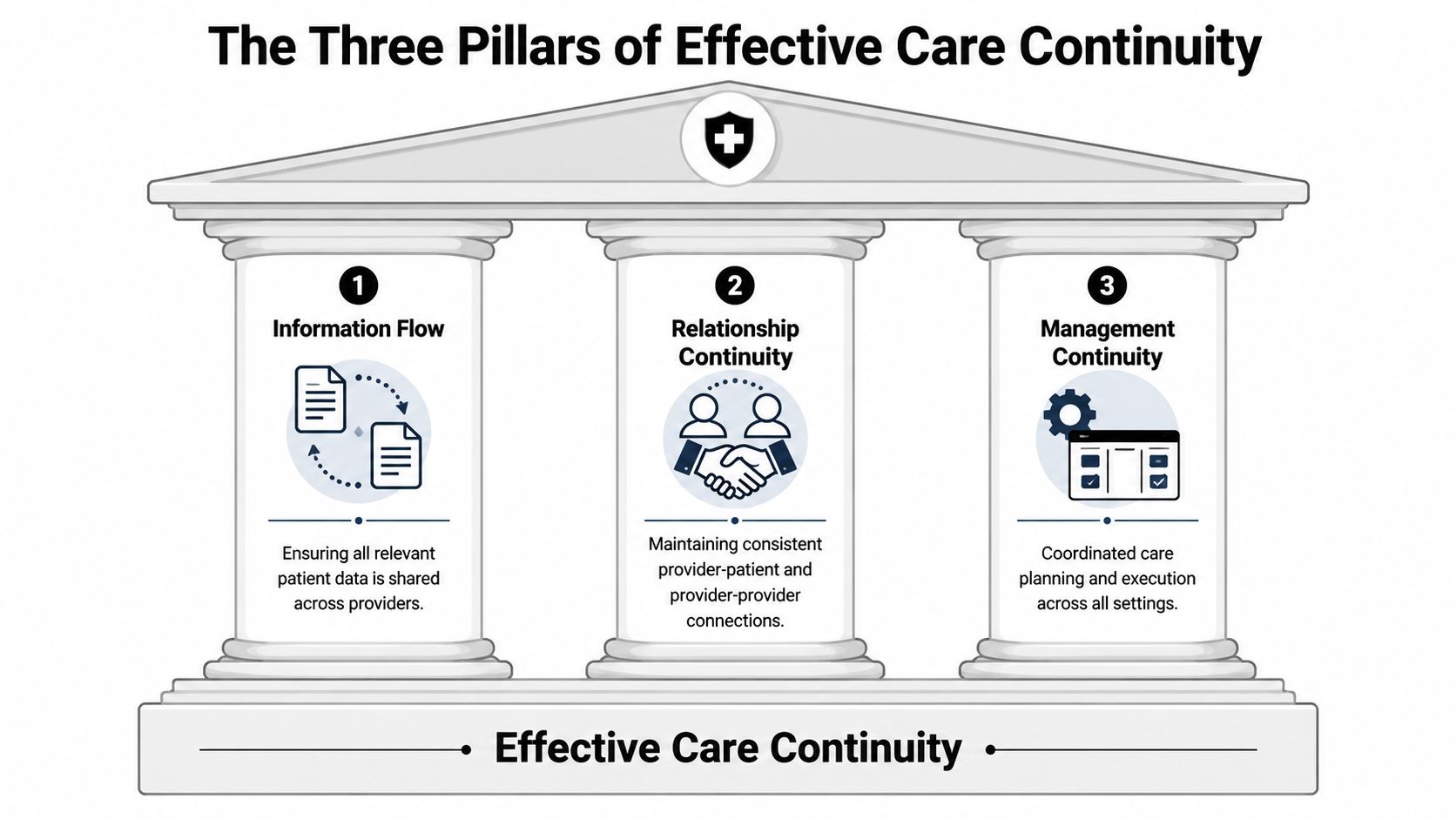
The continuity literature separates care into informational continuity, management continuity, and relational continuity. It also makes an important point. Transitions often fail when any one of these pillars is weak (continuity framework in the clinical literature).
Informational continuity
This is the backbone.
Informational continuity means the next team receives an accurate, usable picture of the patient. That includes history, values, preferences, active problems, recent imaging or labs if relevant, mobility status, equipment needs, and the current treatment plan. In transfer work, it also includes the details people forget to write down, such as whether the patient becomes confused at night, whether they need bariatric handling, or whether a family member holds the healthcare proxy.
A practical example is simple. If the receiving hospital gets the latest MRI report, current medication list, oxygen settings, and code status before wheels-up, they can prepare correctly. If they don't, the same transfer becomes a scramble on arrival.
Management continuity
Management continuity is the coordinated plan that adapts as the patient moves through settings.
Many transfers falter when records arrive, but nobody has translated them into an operational plan. The sending physician intends one thing. The transport clinician is briefed on another. The receiving service expects something else.
Good management continuity answers questions such as:
- What is the immediate plan on arrival
- Which therapies continue during transport
- What should trigger escalation
- Who confirms medication reconciliation
- What follow-up must already be scheduled
Without that coordination, everyone is acting with partial authority.
Relational continuity
Relational continuity gives families and clinicians a stable line of trust.
In a complicated move, this doesn't always mean the same physician stays with the patient. It often means one reliable coordinator remains visible from start to finish. That may be a case manager, transport coordinator, or lead clinician who can say, “Here is the current plan, here is what changed, and here is who owns the next step.”
Here's a quick way to assess the three pillars during a transfer:
| Pillar | What it should answer | Warning sign |
|---|---|---|
| Informational | Does the next team have the full current story | Different teams are using different medication lists |
| Management | Is there one coordinated plan across settings | Transport, sending team, and receiving team describe different next steps |
| Relational | Does someone stay accountable across the handoff | Family doesn't know who to call for a real update |
When teams strengthen all three, patient continuity of care becomes visible. Delays shrink, repeated questions decrease, and the receiving side can act instead of reconstruct.
Common Barriers That Disrupt Patient Care
Most continuity failures are ordinary. That's what makes them dangerous. They don't look dramatic at first. They look like missing pages, rushed sign-out, unclear ownership, or one unchecked assumption.
Records that don't move cleanly
Electronic records often don't travel as smoothly as people expect. Different systems may not share data well. Scanned documents may arrive out of order. A discharge summary may lag behind the current bedside picture.
The fix is procedural, not magical. Before transport is confirmed, someone should verify exactly which documents were sent, which were received, and whether the receiving team can open and interpret them. For teams trying to tighten this workflow, these medical documentation standards for transfers help frame what “complete” should mean.
Bedside handoffs that are too rushed
Shift change is a known weak point in practice, especially when a transfer is also being arranged. A nurse gives report quickly. A physician assumes the case manager relayed the latest update. The transport crew gets a packet but not the context.
A better handoff includes three layers:
- Clinical status such as current stability, recent changes, and key risks
- Operational status such as acceptance, destination readiness, and equipment needs
- Family status such as who has consent authority and who expects updates
The receiving team doesn't just need documents. They need the story behind the documents.
Medication reconciliation failures
Medication errors don't always come from a dramatic mistake. Often the list hasn't been reconciled after a change in unit, provider, or discharge plan. During transport, that can create confusion around dosing schedules, holds, discontinued medications, or what was given just before departure.
A useful countermeasure is to identify one final, time-stamped medication list and one person accountable for confirming it against the transfer packet.
Families left outside the communication loop
Families often spot inconsistencies before anyone else. They know the patient's baseline, behavioral changes, swallowing issues, home supports, and previous complications. Yet they're sometimes treated as passive observers.
That's a mistake. Families should know the destination, timing, transport plan, precautions, and primary contact. One designated family communicator also reduces mixed messages and repeated calls that pull staff away from coordination work.
A lot of what disrupts patient continuity of care is fixable. The pattern is usually the same. Nobody owns the handoff end to end, so every team only sees its slice.
A Practical Checklist for Families and Case Managers
Good continuity depends on disciplined basics. The safest transfers use a repeatable checklist, not memory.
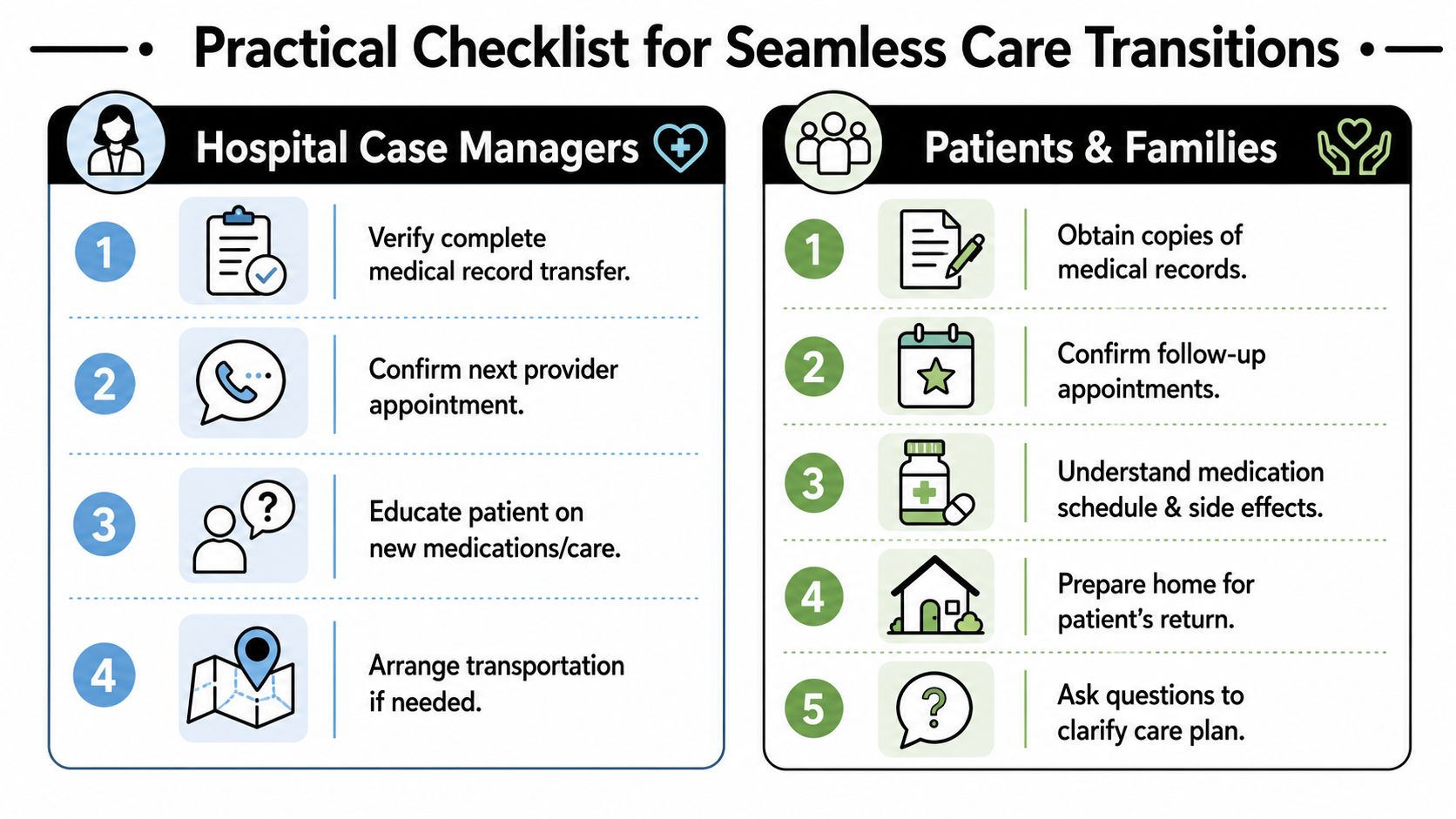
Best practices for continuity include using structured handoff tools such as SBAR, I-PASS, or ISHAPED, reconciling medications before discharge, and completing a follow-up call within 72 hours to catch early complications (continuity transition best practices). That standard gives both professionals and families something concrete to work from.
Checklist for hospital case managers
Use this as a transfer-readiness screen before the patient moves.
- Confirm clinical acceptance: Make sure the receiving clinician or facility has formally accepted the patient and understands why the transfer is happening.
- Use a structured handoff tool: SBAR, I-PASS, and ISHAPED all create more reliable communication than freeform sign-out.
- Lock the current medication list: Reconcile additions, holds, and recent administrations before the packet goes out.
- Send records in usable form: Include the latest summary, active orders as appropriate, allergies, code status, imaging reports if relevant, and key consultant notes.
- Match transport to need: Confirm oxygen, monitoring, mobility requirements, infection precautions, and any special loading or bariatric considerations.
- Schedule the next step before discharge: If the patient is leaving one setting for another level of care, don't leave follow-up vague. Confirm what happens next and who owns it.
- Plan the 72-hour contact: Early follow-up is where hidden problems surface.
- Give the family one point of contact: Confusion drops when one person owns updates.
A discharge planning resource can help teams pressure-test the basics. This hospital discharge checklist with 8 key steps is a practical companion for transitions that involve both clinical and logistical coordination.
Checklist for families
Families don't need to run the case. They do need to ask clear questions.
Who is our main contact today
Get one name, one role, and one phone number.What is the exact destination and level of care
“Another hospital” isn't enough. Ask for the unit or service if available.What changed in the last 24 hours
That question often reveals the risk points most likely to matter during transport.Can we review the current medication list together
Ask what was stopped, started, or held.What records are traveling with the patient
Don't assume everything moved because someone said it was sent.What should we bring or prepare
Think advance directives, insurance information, mobility aids, hearing aids, glasses, and charger cables for communication devices.Who should we call after arrival
The answer should be specific.
A simple family communication rule
- Choose one family spokesperson: This reduces conflicting instructions.
- Write down answers in real time: Verbal updates blur together fast.
- Repeat back the plan: “So the patient is going to X facility, transport is set for Y, and Z is our receiving contact.” That catches misunderstandings immediately.
Coordinating Air Ambulance Transport Seamlessly
At 2 a.m., a patient is accepted by a higher-level hospital three states away. The sending nurse has updated vitals, the family is calling for answers, the aircraft is on a schedule, and the receiving team needs a clean report before the patient lifts off. In air medical transport, continuity of care is won or lost in those handoffs.

Long-distance transfer exposes problems that a local move can sometimes absorb. Missing records, unclear code status, outdated medication lists, and vague arrival plans create delays and risk. An air ambulance transfer works best when the team treats it as one continuous bedside-to-bedside clinical operation with multiple handoffs, each of which has to be deliberate.
What Effective Transport Coordination Requires
Safe air transport usually depends on a few disciplined basics:
- One current clinical summary that travels with the patient and reflects the latest status
- Direct clinician-to-clinician report between the sending and receiving teams
- A transport crew matched to the patient's condition, including likely airway, cardiac, medication, or mobility needs
- Timing that protects the handoff, so ground pickup, aircraft departure, and hospital arrival do not leave the patient waiting in the wrong setting
- Clear communication with family, including who will call, when updates will come, and what happens on arrival
Logistics around the flight matter too. Families are often trying to arrange housing, destination planning, and responsibilities left behind at home. If a pet also needs to be relocated, it helps to find safe pet movers through a separate service so the medical plan does not get derailed by avoidable last-minute decisions.
Why one coordinator matters
Air transport goes more safely when one team owns the moving parts. Someone has to confirm the accepting facility, verify records, align ground units with flight timing, communicate changes in condition, and keep the family from getting three different versions of the plan.
That central coordination role reduces one of the most common transfer failures: everyone assumes someone else made the call. A service such as Med Jets by Air Trek's bedside-to-bedside flight coordination can serve as the operational link between facilities, transport legs, and family updates during a complex transfer.
A short visual overview helps show how these moving parts come together in practice.
Where air ambulance handoffs break down
Problems usually start with assumptions.
- Assuming the receiving hospital already has the full chart
- Assuming the flight crew got the last clinical update
- Assuming consent, contact names, or decision-maker details are already documented
- Assuming equipment and medication needs were confirmed before departure
- Assuming “stable for transport” means the patient needs only routine planning
In practice, those gaps show up fast. A patient arrives without the latest imaging report. The receiving unit expects telemetry, but the bed request says med-surg. A medication infusion continues in transit, but the receiving team was not told it was restarted.
Patients can still make it through those failures. The transfer is harder than it needed to be, and the risk shifts to the bedside team catching mistakes under time pressure.
Your Role in Championing Safer Transfers
Patient continuity of care doesn't happen because good people are involved. It happens because someone insists on a complete handoff.
If you're a family member, your role is to ask precise questions, keep one current version of the plan, and speak up when details don't line up. If you're a case manager or discharge planner, your role is to turn scattered tasks into one coordinated transfer.
Advocacy is part of continuity. Families who need help speaking up can use practical guidance like these tips for advocating with your doctor to ask better questions and get clearer answers.
The strongest transfers are rarely the quietest. They're the ones where communication is deliberate, responsibilities are named, and no one treats the handoff as an afterthought.
Frequently Asked Questions About Continuity of Care
Who is responsible for continuity during a transfer
Responsibility is shared, but shared responsibility can become no responsibility if nobody is clearly named. In practice, the safest transfers have a visible lead at each stage: a sending clinician or case manager, a transport lead, and a receiving contact. Families should always ask who owns the next step right now.
Is continuity of care only important for long-term chronic care
No. It matters in chronic care, but it is just as important during short, high-risk transitions such as hospital discharge, rehab placement, and air medical transfer. An extensive review of 25 studies showed that greater continuity of care has a statistically significant protective effect on all-cause mortality and is also associated with fewer avoidable hospitalizations, lower costs, and higher patient satisfaction.
What should families prepare before a complex transfer
Start with the essentials:
- Current medication list
- Insurance and identification documents
- Advance directives or decision-making paperwork
- Primary family contact information
- A simple written medical timeline
- Baseline functional details, such as mobility, communication limitations, and equipment use
Those basics help every team understand the patient faster.
What if the patient is traveling across state lines or internationally
Complex geography increases the number of handoffs. That means more attention has to go to records, receiving acceptance, transport medical capability, and family communication. The core principle stays the same. The patient's clinical story and plan have to move intact, not just the patient.
How can I tell whether continuity is weak
Look for operational clues. Different teams describe different plans. The medication list keeps changing depending on who you ask. No one can name the receiving clinician. The family gets vague answers about timing or destination. Those are early warnings that the handoff needs to be tightened before the transfer proceeds.