You're often asked to solve the same problem under very different conditions. A patient is stable enough to leave the sending facility, but not mobile enough to manage the trip without help. The family wants reassurance. The bedside team wants a safe handoff. The receiving facility wants an accurate ETA and no surprises at the door.
That's when a patient transport chair stops being a piece of hallway equipment and becomes part of the care plan.
In hospital work, discharge planning, and long-distance medical transport, the chair affects more than convenience. It shapes how a patient is transferred out of bed, through corridors, into elevators, across ramps, through ambulance doors, and sometimes all the way to an aircraft. It also affects whether staff can do that work repeatedly without unnecessary strain. If the chair is the wrong type, poorly fitted, or hard to control, you feel the consequences immediately.
I've seen new case managers assume a transport chair is just a lighter wheelchair. That assumption causes avoidable problems. A standard wheelchair is often built around user propulsion. A patient transport chair is built around attendant-driven movement, quick transfers, and controlled handling in clinical environments. Those differences matter most when the route is long, the patient is frail, or the handoff involves multiple teams.
More Than a Wheelchair Why Transport Chairs Are Critical
A patient might leave a med-surg floor in one city, transfer by ground to an airport, continue by medical flight, then finish with another ground leg to rehab or home. On paper, that looks like a sequence of transports. In practice, it's one continuous chain of positioning, monitoring, lifting risk, fatigue, and patient dignity.
What makes a transport chair different
A patient transport chair is designed for assisted movement. The caregiver drives it. The patient rides in it for a transfer that may be short, repeated, or operationally complex. That sounds simple until the patient has weak trunk control, oxygen tubing, post-op precautions, or anxiety about being moved through busy public spaces.
The chair has to do several jobs well:
- Support the patient safely: It needs stable seating, secure foot placement, and restraint options appropriate to the trip.
- Protect staff mechanics: Brakes, handles, and steering behavior matter when teams are pushing through long corridors or managing ramps.
- Fit the route: Door widths, elevators, ambulance loading, and aircraft access all affect whether the chair is workable.
- Preserve dignity: Patients notice whether they're slumped, exposed, rushed, or repeatedly repositioned.
Practical rule: If the transfer requires planning around lines, fatigue, body habitus, positioning, or multiple handoffs, treat the chair as clinical equipment, not furniture on wheels.
Where people get into trouble
Problems usually start with a shortcut. Someone picks the chair nearest the nurses' station, not the chair suited to the patient and route. The patient is comfortable for ten minutes, then starts sliding. The footrests interfere with a pivot. The brakes are awkward. A staff member leans and reaches instead of working from a neutral posture. None of that shows up on a simple discharge checklist, but all of it changes the safety profile of the move.
For a new case manager, that's the key mindset shift. Don't ask only, “Do we have a chair?” Ask, “Is this the right patient transport chair for this specific transfer?”
Understanding the Four Main Types of Patient Transport Chairs
Not all transport chairs belong in the same category. Some are basic discharge tools. Some are built for larger patients. Some improve entry and exit. Others solve a stair problem. If you use one label for all of them, you'll miss the trade-offs.
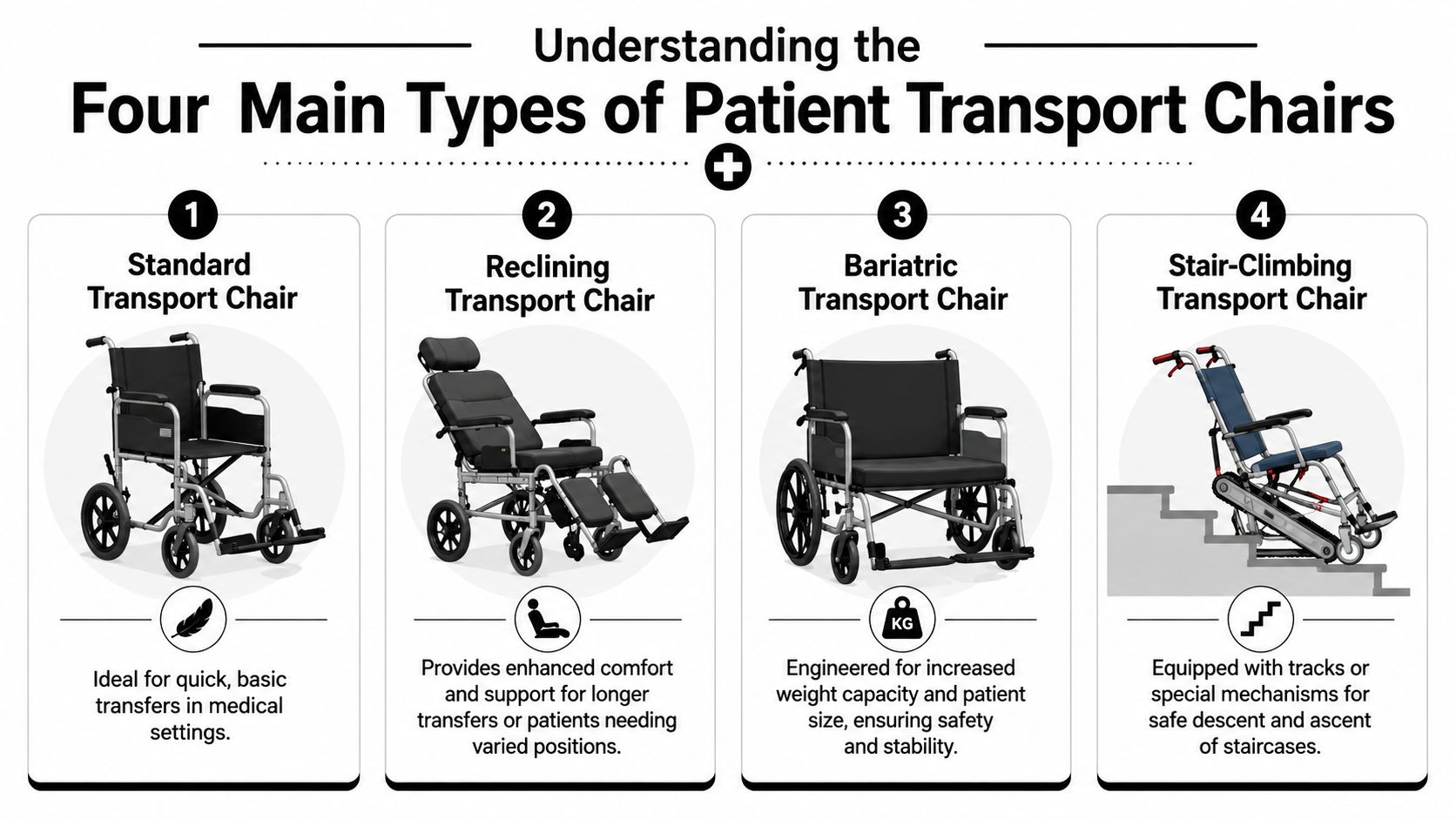
Standard transport chairs
This is the workhorse that often comes to mind first. It's typically used for hospital discharge, clinic movement, and short assisted trips where the patient can sit upright and doesn't need special positioning.
A standard chair works best when the patient needs mobility help but not complex seating support. It's a practical choice for routine facility movement, especially when storage space and fast turnover matter. Industry specifications also show that the category has grown beyond very light-duty models. A standard folding transport chair line may be rated up to 400 lb, while specialized motorized patient transport chairs may be rated up to 750 lb, which shows how far the equipment class has expanded for standard and bariatric use according to patient transport chair product specifications from PHS West.
Bariatric transport chairs
These aren't just wider chairs. A bariatric patient transport chair changes the entire handling equation. Capacity matters, but so do frame strength, stability during turns, the load path through the chair, and whether staff can control it without awkward body mechanics.
Use this type when the patient's size, weight distribution, or need for a more stable seating platform would make a standard chair unsafe or impractical. In real operations, bariatric planning also affects doorway clearance, ramp approach, and whether the receiving team has compatible equipment.
Staxi and ambulatory-style chairs
This category helps with a very specific problem. Some patients can bear some weight, pivot with help, or step into a seat more easily than they can transfer into a low or deep transport chair. Staxi-style designs can help entry and exit, but they aren't the right answer for every route or every staff member.
These chairs can be useful when access is the main challenge, not prolonged sitting support. They may be less forgiving if the route includes ramps, long pushes, or repeated turns.
Reclining and stair-climbing chairs
These are very different tools, but both belong in the “special problem” category.
A reclining transport chair helps when the patient can't tolerate full upright sitting for the whole transfer, needs postural support, or is at risk of discomfort during a longer move. A stair-climbing transport chair is chosen when stairs are the operational barrier and there's no better route available.
Patient Transport Chair Types at a Glance
| Chair Type | Primary Use Case | Ideal Patient Profile | Key Feature |
|---|---|---|---|
| Standard transport chair | Routine discharge and facility transfers | Patient who can tolerate upright seated transport with attendant assistance | Simple attendant-driven mobility |
| Reclining transport chair | Longer transfers or positioning-sensitive movement | Frail, fatigued, or posture-dependent patient | Adjustable back support |
| Bariatric transport chair | High-capacity transport and added stability needs | Larger patient needing wider seating and stronger frame support | Heavy-duty capacity and reinforced design |
| Stair-climbing transport chair | Routes with unavoidable stairs | Patient needing controlled stair ascent or descent with trained staff | Stair mechanism or track system |
The best chair type is the one that matches the whole route, not just the first five minutes of the trip.
Decoding Key Features for Safe and Efficient Transfers
A chair can look acceptable in a product photo and still perform poorly in real transfer work. The details that matter most are usually the ones people skip over during procurement. Handling, brake design, restraint options, and access around the patient all matter more than cosmetic comfort features.

Start with braking and handling
If staff have to bend, reach, or reposition their bodies every time they stop the chair, fatigue builds quickly over repeated transports. That's why brake design deserves more attention than it usually gets.
The Stryker Prime TC is a good example of how manufacturers frame this issue. The company states a 500 lb (226.8 kg) weight capacity and a one-touch central brake intended to reduce caregiver bending and reaching in repeated hospital transfers, as shown in the Stryker Prime TC product specification sheet. That's the right lens for evaluation. Don't just ask whether a chair has brakes. Ask whether the braking system supports controlled workflow without forcing poor body mechanics.
Features that help the transfer itself
Once the chair is stopped, the transfer begins. That's where access features become important.
Look for these practical elements:
- Swing-away or removable footrests: These reduce interference during pivots and help staff position close to the patient.
- Armrests that don't trap the transfer: Fixed structures can make lateral or assisted seated transfers harder than they need to be.
- Push handle placement: A handle that's too low or poorly shaped can make the chair harder to steer over a long route.
- Secure restraint options: A lap belt may be enough for one patient. Another may need more trunk support and closer observation.
Clinical accessories matter more than people expect
A chair used in medical transport often carries more than a patient. It may need to coexist with oxygen, a drain, a line set, or a monitoring setup. That doesn't mean every chair should be loaded with accessories. It means the team should think through what must travel with the patient and what should stay with the escort or ground crew.
Questions to ask before approving a chair
- Will the patient remain upright comfortably for the entire route?
- Can staff secure lines, tubing, and belongings without creating snag points?
- Does the chair allow clean access for reassessment, repositioning, or emesis management if needed?
- Can the receiving team use the same chair through the next handoff, or will another transfer be required?
The wrong feature set usually doesn't fail at the start. It fails midway, when the patient is tired, the hallway gets crowded, or a handoff team has to improvise.
Selecting the Right Chair for Hospital and Air Transfers
A patient transport chair that works beautifully inside one hospital may be a poor choice for a long ground leg or an air medical mission. The route changes the answer. So does the patient's tolerance for time upright, the number of transfers, and whether the environment is controlled or constrained.
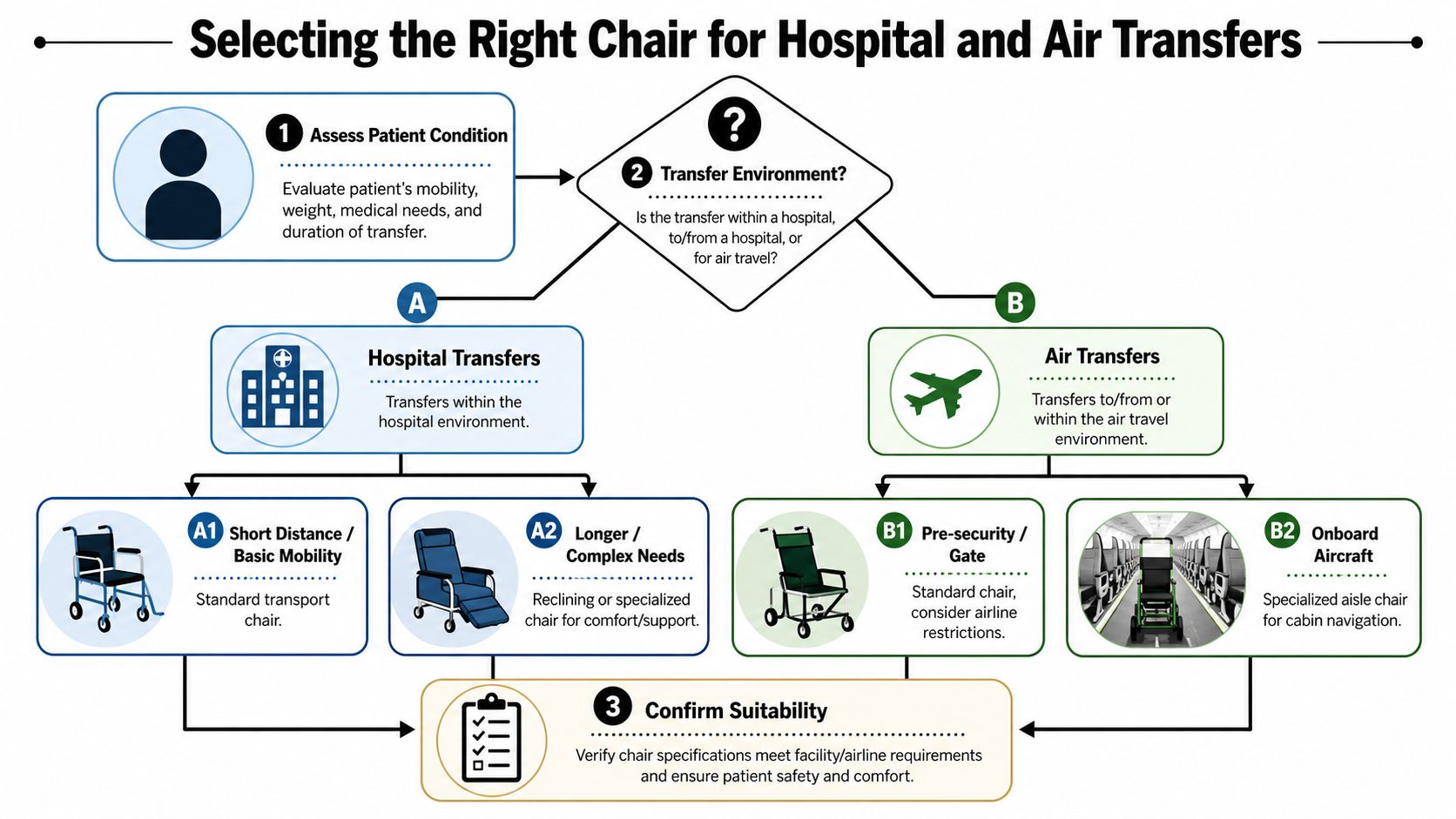
Match the chair to the transport environment
For in-hospital movement, efficiency usually matters most. You need a chair that moves cleanly through corridors, parks securely for bedside transfer, and doesn't create extra work for nursing or transport staff.
For hospital-to-facility discharge, comfort and route fit become more important. The patient may spend longer in the chair, and the transfer often includes elevators, curb cuts, van or ambulance loading, and a receiving entrance that may not be ideal.
For air transfer, the decision gets narrower. The chair may be perfect for terminal movement or bedside preparation and still be unsuitable for cabin access or final aircraft loading. In aviation-linked transport, teams often use more than one mobility device across the full chain, because no single chair solves every access point well.
Positioning becomes more important on long routes
For frail or bariatric patients, prolonged upright time can become the main issue. Positioning is not just a comfort question. It affects tolerance, belt fit, pressure distribution, and whether the patient arrives more fatigued than when they left.
The University of Michigan wheelchair transportation safety guidance notes that up to 30 degrees of backrest recline relative to vertical and up to 30 degrees of seat incline can be acceptable, while also warning that too much incline can load the abdomen rather than the pelvis, as explained in the UMTRI wheelchair transportation safety FAQ. That's highly relevant for long transfers. If the patient needs some recline, the chair must support that positioning appropriately, not just loosely “lean back.”
A chair that keeps a patient in the wrong position for an hour can become a bigger problem than a shorter transfer with an extra equipment change.
Questions I'd want answered before an air-linked transfer
Not every trip needs the same level of scrutiny, but these questions consistently matter:
- How many total handoffs are planned? Every extra transfer increases fatigue and coordination risk.
- Will the patient tolerate a standard upright chair for the full preflight and postflight segments?
- Does the route include narrow passages, stairs, jet access issues, or long terminal movement?
- What equipment must stay with the patient throughout the trip?
- Will the final receiving environment accept the same chair, or does the plan change at arrival?
If the family or facility is still deciding between local discharge options and long-distance medical transport, the planning process usually starts with the full route and level of support, not the chair alone. That's where a service such as medical flight planning for hospital-to-home transport enters the discussion.
Navigating Clinical and Safety Considerations
The safest patient transport chair is the one that protects both the passenger and the people pushing it. In daily operations, those two goals are tied together. If the patient is poorly positioned, staff compensate. If the chair steers badly or stops awkwardly, the patient feels every correction.
Patient safety on longer transfers
Short trips can hide problems. A patient may look fine leaving the room and start to slide, lean, or guard against pain halfway down the route. That's why I pay close attention to posture, foot placement, line management, and whether the patient has enough support to stay aligned without constant hands-on correction.
Clinical concerns usually include:
- Pressure and tolerance: Frail patients may need repositioning or a different seating approach if the route is long.
- Post-op protection: Hip precautions, sternal precautions, or painful abdominal surgery can change transfer setup.
- Attachment management: Oxygen tubing, drains, and infusion lines need a clean path with enough slack and clear visibility.
- Emotional tolerance: An anxious patient may need slower movement, clearer communication, and fewer abrupt transitions.
Caregiver strain is not a minor issue
A 2020 ergonomic study comparing three patient transport chairs found measurable differences in caregiver biomechanics during transport. The study reported greater wrist flexion with one chair compared with two others, and greater peak trunk flexion with another, showing that chair design can materially affect physical strain for transport staff according to the ergonomic patient transport chair study indexed on PubMed.
That finding matches what crews already know from practice. Handle position, steering behavior, and brake access change how staff move their own bodies. Over repeated transports, those small differences become operationally important.
What usually works better
- Neutral pushing posture: Staff should be able to move the chair without sustained wrist bend or leaning.
- Predictable turning behavior: A chair that tracks cleanly reduces abrupt corrections in crowded spaces.
- Simple brake engagement: If the stop sequence is clumsy, transfers become less controlled.
- Adequate staffing for route complexity: Stairs, long ramps, and heavier patients need planning, not improvisation.
Good transport work looks calm. That calm usually comes from setup, not luck.
Maintenance, cleaning, and staff readiness
Even an excellent chair becomes unreliable if the brakes drift, the footrests loosen, or the upholstery is hard to disinfect between uses. Facilities should treat these chairs like frontline transport equipment. That means scheduled inspection, clear cleaning protocols, and consistent staff use standards.
Training matters just as much as the hardware. Teams need to know how to approach the patient, lock the chair, protect lines, and move through environmental obstacles without rushing. Case managers who want a better feel for those operational issues can review patient transport training resources for coordinated medical transfers.
Procurement Checklist for Case Managers
When you're choosing a patient transport chair, the fastest way to make a bad decision is to shop by appearance or by seat width alone. Procurement works better when you move in order: patient, route, features, environment, then vendor support.
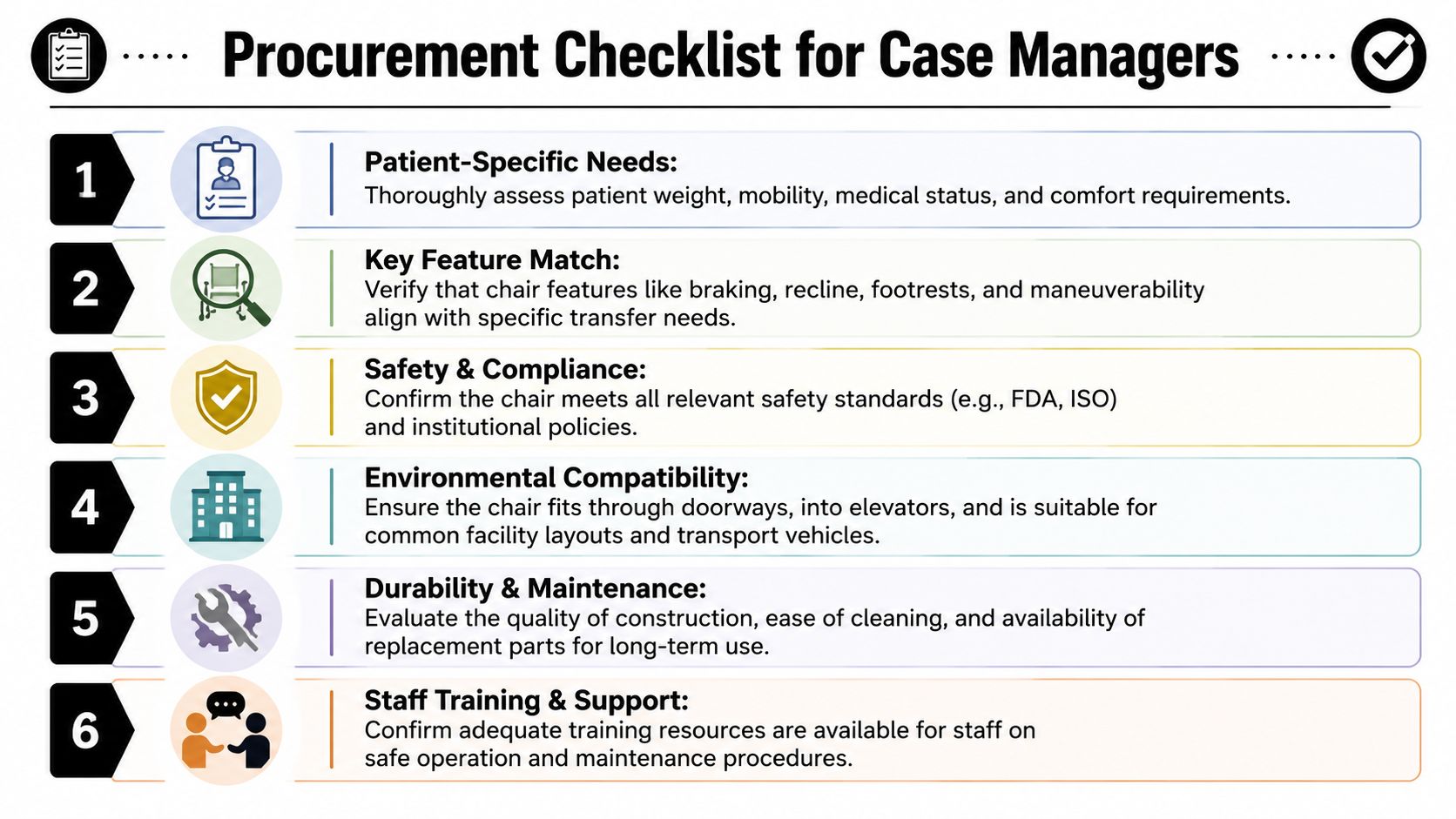
A practical chair selection checklist
Clarify the patient profile
Start with mobility, trunk control, transfer ability, weight-bearing status, pain, and any medical attachments that must travel with the patient. If the patient is frail, bariatric, or prone to sliding, note that before you look at product options.Map the full route
A chair that works from bed to elevator may fail at the ambulance bay or receiving entrance. Check doorways, ramps, long corridors, uneven exterior surfaces, and any stair exposure.Identify the transfer method
Ask how the patient will get into and out of the chair. If the patient needs pivot help, lateral transfer support, or extra foot clearance, those needs should shape the feature list.
Features and vendor questions that save time later
Use these questions during rental or purchase review:
- Braking and handling: Is the brake easy for staff to engage without bending awkwardly?
- Patient support: Does the chair provide the restraint and positioning options appropriate for this patient?
- Environmental fit: Will it work in the sending facility, vehicle, and receiving site?
- Cleaning and upkeep: Can your team disinfect it quickly and inspect it easily between uses?
- Training: Will staff receive practical setup and operation guidance?
- Availability: Can the vendor deliver the correct model when the transfer happens, not just in theory?
Keep the workflow documented
The best procurement note is short and specific. It should explain why this chair was selected for this patient and route. That helps the next team, supports continuity, and reduces last-minute substitutions.
If you coordinate transfers often, it helps to keep a standard reference set for vendors, patient criteria, and route planning. Many discharge planners build that into their case manager transfer planning resources.
Patient Transport Scenarios and FAQs
A patient transport chair decision gets easier when you test it against real cases. The goal isn't to find a perfect chair in the abstract. It's to find the right chair for the actual journey.
Scenario one with a bariatric long-distance transfer
A sending hospital needs to move a larger patient from acute care to an out-of-state facility. The patient can sit up, but the route includes a long interior push, ground loading, and another handoff on arrival.
The right approach is usually a bariatric transport chair with a stable frame, enough seating width, and handling characteristics the staff can manage safely. Capacity alone isn't enough. The team also needs to verify route clearance, receiving-site compatibility, and whether the same chair can stay with the patient through multiple handoffs.
Scenario two with a frail patient who fatigues easily
An older adult with limited endurance needs transfer from hospital to rehab. The patient becomes uncomfortable when fully upright for extended periods and tends to slump as fatigue sets in.
A reclining transport chair may be more appropriate than a standard model, assuming the positioning supports the patient rather than just letting them slide backward. The team should also reduce unnecessary time in the chair and plan reassessment during longer waits.
Scenario three with a short discharge that still needs care
A patient is going home after surgery and only needs a brief move from unit to vehicle. It's tempting to use whatever chair is nearby.
That can still go wrong if the footrests interfere with the transfer, the patient has precautions, or the family tries to help without guidance. Even simple discharges go better when staff confirm the brakes, route, and transfer plan before the patient stands.
Common questions people ask
Is a patient transport chair the same as a wheelchair
No. A transport chair is generally intended for attendant-driven use, while many standard wheelchairs are designed with user propulsion in mind.
Can one chair handle every part of a hospital-to-air transfer
Usually not. Long-distance transport often requires different equipment solutions for bedside movement, airport or terminal transitions, and final aircraft access.
What matters most for staff safety
Brake access, steering control, handle position, route planning, and enough staffing for the terrain. Those are the factors that most often separate a smooth move from a strained one.
Should families buy or rent
That depends on how long the equipment will be needed, how specialized the chair is, and whether the route is a one-time transfer or part of ongoing care. For many complex transfers, the better first question is whether the equipment can be coordinated as part of the transport plan.
If you're arranging a complex transfer and need help matching the patient, route, and medical support level, the team at Med Jets by Air Trek can coordinate end-to-end transport planning, including air medical options, ground logistics, and clinician-guided handoffs.