
You're often dealing with this under pressure. A patient is ready for transfer, the sending unit wants a timeline, the family wants reassurance, and someone asks a simple question that turns out not to be simple at all: “Do we have the right lift?”
For bariatric transport, that question affects every handoff. It affects whether the patient can move from bed to stretcher without improvisation, whether the ground crew and flight crew are working from the same plan, and whether the receiving facility is prepared for safe arrival. Good bariatric lift equipment isn't just a hospital purchasing issue. It's a bed-to-bed transport issue.
That's where case managers and discharge planners usually need the clearest guidance. Many articles explain hospital lifts in isolation. Fewer explain what happens when the patient has to move through several environments in one chain: inpatient room, hallway, elevator, ambulance, air base, aircraft, destination ambulance, receiving facility. That chain is where small mismatches become big safety problems.
What Is Bariatric Lift Equipment
When standard patient handling is no longer safe, bariatric lift equipment becomes the working system that protects both the patient and the staff. It replaces manual lifting with mechanical assistance and gives the team a structured way to manage higher weight, larger body dimensions, limited mobility, and fragile medical status.
That matters because “bariatric” does not mean only “heavier patient.” In transport planning, it also means wider support surfaces, stronger frames, appropriate slings, better stability, and enough clearance to move through real spaces without forcing unsafe workarounds.
According to Robson Forensic's overview of bariatric patient injury risks, bariatric patient lifts are part of a broader category of specialized bariatric equipment intended to reduce the risk of injury to both patients and caregivers during transfers, including overhead or ceiling lifts, portable hydraulic lifts, specialized slings, and reinforced hospital beds.
Why standard equipment often isn't enough
A standard transfer setup may work well for many patients. It stops being appropriate when the patient's size, weight distribution, mobility limits, or medical complexity exceed what that setup was built to handle.
In those cases, the issue isn't convenience. It's safety.
Practical rule: If the team is discussing “how many people it will take” instead of “which mechanical aid matches the transfer,” the plan needs another look.
Case managers often ask, “Isn't a lift just a lift?” No. Bariatric lift equipment is built around different demands:
- Higher load handling: The lift and sling must support more weight without operating at the edge of their rating.
- Greater stability: The base, boom, and spreader bar have to control sway and maintain balance during movement.
- Wider patient support: The sling and contact surfaces must fit the patient's body safely and comfortably.
- Safer workflow: The transfer should reduce manual repositioning, not create more of it.
Think in terms of the whole care pathway
The right question isn't only, “What lift is in the room?” It's, “What equipment will be used from the first move to the final handoff?”
That broader view is especially useful when the patient's care pathway may also involve surgery, rehabilitation, or long-term mobility planning. For families trying to understand the larger bariatric care journey, Pause Medical's 2026 bariatric surgery guide can help frame the medical side of that discussion.
For transport, the practical takeaway is simple. Bariatric lift equipment is not a single device. It's a coordinated set of tools and procedures that lets the team move a patient with dignity, predictability, and less risk.
Common Types of Bariatric Patient Lifts
Not every bariatric lift solves the same problem. Some are best for in-room transfers. Some are built for repeated movement across different spaces. Others depend on the patient being able to bear some weight. If you're coordinating transport, you need to know the role each device plays.
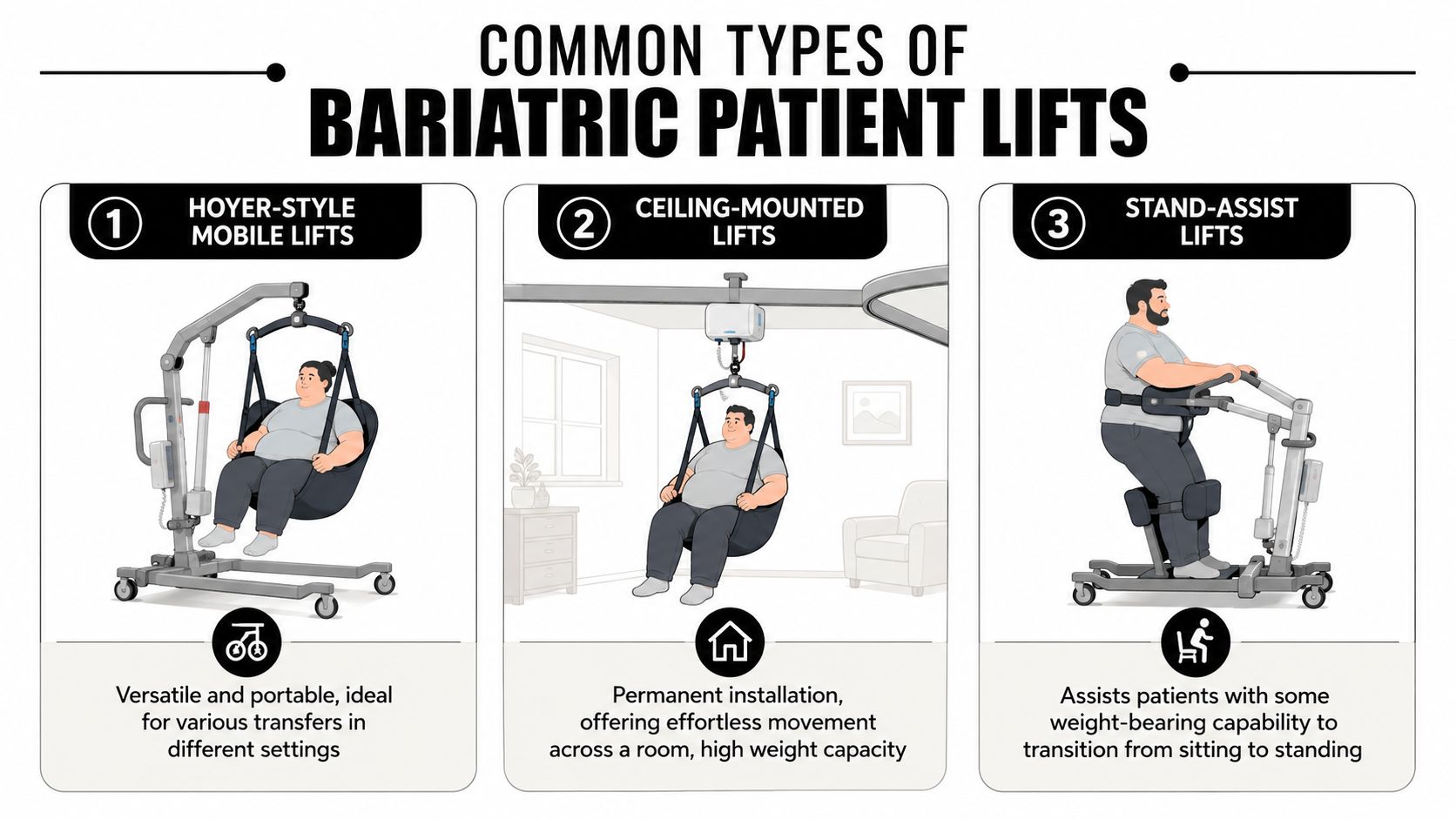
Mobile floor lifts
This is the lift many people picture first. A Hoyer-style mobile lift rolls on a wheeled base, uses a boom and spreader bar, and lifts the patient in a sling. It's useful when the patient has to move between bed, chair, commode, stretcher, or exam surface in spaces that don't have an overhead track.
Mobile lifts are often the practical choice when the transfer path extends beyond one room. They can also be relevant when a team has to work around variable layouts at the sending or receiving facility.
Portable bariatric lifts may use hydraulic or electric actuators and powered base-widening mechanisms that adjust the support footprint to maintain stability. They may also include emergency manual overrides for safe descent if power fails, as described by Rehabmart's bariatric lift equipment overview.
Ceiling-mounted lifts
A ceiling-mounted lift runs on a fixed overhead track. In the right room, it can provide smoother, more controlled transfers with less pushing and turning than a floor lift. Staff often prefer it for frequent bed-to-chair or bed-to-commode movement because it reduces floor clutter.
Its limitation is obvious. It only works where the track exists. That makes it excellent for inpatient rooms and less useful once the patient leaves that environment.
Stand-assist lifts
A stand-assist lift is for a patient who can participate and bear some weight. It helps with seated-to-standing transitions and short transfers. It is not the right device for someone who cannot safely support weight, has poor trunk control, or needs a full-body lift.
That distinction matters because people sometimes hear “lift” and assume all devices are interchangeable. They aren't.
Slings and transfer accessories
The sling is not an accessory you pick at the last minute. It is part of the lifting system. Sling shape, attachment style, size, and body support need to match both the patient and the lift.
A poorly matched sling can turn a technically available lift into an unsafe option.
Here's a quick comparison case managers can use:
| Equipment type | Best use case | Main limitation |
|---|---|---|
| Mobile floor lift | Moving between different rooms or surfaces | Needs adequate floor space and turning room |
| Ceiling-mounted lift | Repeated in-room transfers | Fixed to specific rooms |
| Stand-assist lift | Patient can bear some weight | Not for full dependent transfers |
| Specialized sling | Supports positioning and body fit | Must match both patient and lift |
If your team also uses seated transfer solutions in non-lift scenarios, patient transport chair options can help clarify where a transport chair fits and where it does not.
The right device is the one that fits the patient's function, the environment, and the next step in the transfer. Not the one that happens to be closest.
Understanding Key Technical Specifications
A great deal of confusion arises. Someone hears that a lift is “bariatric rated” and assumes that means it's automatically suitable. It doesn't. You need to look at the specifications that affect real transfer safety.
Safe working load
The most important figure is the Safe Working Load, or SWL. Bariatric patient lifts typically have SWL ratings starting around 600 lb, with heavy-duty models exceeding 1,000 lb, and best-practice guidance recommends a safety margin of at least 20 to 25% above the patient's weight to accommodate dynamic loading and reduce mechanical stress, according to Design Specific's review of bariatric medical equipment features.
That safety margin is not just a paperwork detail. During a transfer, the load shifts. The patient may lean, the sling may settle, the lift may roll over uneven flooring, and the equipment experiences more than a static straight-up weight.
A useful question to ask is: What is the patient's actual current weight, and what is the rating of the exact lift being used?
Footprint and clearance
A second issue is physical fit. A lift can have enough capacity and still fail operationally if it can't get under the bed, through the doorway, or into position at the stretcher.
Some bariatric lift designs have wide bases for stability, but that width can become a problem in tight hallways, elevator lobbies, or aircraft-adjacent transfer areas. Closed-base dimensions matter. Open-base dimensions matter. Ground clearance matters.
Ask practical questions such as:
- Will the base fit under the hospital bed or stretcher frame
- Can it clear the doorway and room layout
- Is there enough turning space in the transfer area
- Will the receiving unit accept the same equipment profile
Power and control systems
Electric and hydraulic systems each have a place. In transport, what matters most is controlled movement, reliable operation, and a fail-safe plan if power is interrupted.
A lift with emergency lowering capability is easier to integrate into a high-acuity transfer plan than a device that leaves the team stuck if the power system fails.
If the lift rating is close to the patient's weight, you're not planning a routine transfer. You're planning a threshold event.
The spec sheet should answer operational questions
Case managers don't need to become biomedical engineers. They do need enough fluency to ask the right questions before transport day. Capacity, base width, under-bed clearance, boom range, and emergency controls all translate into one operational question: Can this device complete the transfer safely in the actual spaces involved?
Safety Standards and Training Requirements
A bariatric lift does not create safety by itself. The team does. The device is only one piece of a safe patient handling system, and that system depends on training, inspection, maintenance, and clear role assignment during the move.
That's why I tell case managers to listen carefully for how a provider talks about process. If the conversation stays focused on equipment names alone, you're only hearing part of the story.
What staff training should cover
A trained crew should know how to select the right sling, confirm compatibility, stage the room, protect lines and drains, manage patient anxiety, and coordinate commands during the lift. They also need to know when to stop and escalate if the setup is not right.
Questions worth asking include:
- How are crews trained on bariatric transfer equipment
- How do they verify sling and lift compatibility
- What do they do if the sending room is too tight for the planned lift
- Who has final authority to pause an unsafe transfer
For organizations reviewing formal education pathways, patient transport training resources can help clarify how transport-specific preparation fits into safe handling.
Maintenance matters as much as training
Bariatric transfers place high demands on equipment. A lift that is overdue for inspection, missing a component, or paired with a worn sling is not a minor issue.
A strong provider should be able to explain:
| Safety area | What you want to hear |
|---|---|
| Equipment checks | The team inspects lifts and sling condition before use |
| Maintenance process | Devices follow a documented service schedule |
| Crew roles | Each person has a defined job during transfer |
| Escalation | The crew can delay or redesign the move if needed |
Safety is a culture, not a checkbox
Some of the safest transports I've seen were not the fastest. They were the most deliberate. The crew paused, re-measured, repositioned, or changed the plan because the first approach didn't give enough margin.
“We can move the patient” is not the same as “we can move the patient safely through every handoff.”
That distinction protects everyone involved.
Coordinating Ground and Air Medical Transport
Most transport failures don't start in the aircraft. They start earlier, when one stage of the plan is built without the next stage in mind.
That's why end-to-end coordination matters so much in bariatric cases. Publicly available literature offers sparse practical guidance on how bariatric lift equipment is integrated into end-to-end patient transfers, particularly the handoff from ground EMS to air ambulance, creating a critical knowledge gap for case managers arranging complex transports, as noted by Diagnostic and Interventional Cardiology's discussion of bariatric mobility equipment and facility considerations.

The handoff chain has to be continuous
A clean bariatric transfer usually follows a sequence like this:
Sending facility review
The team confirms patient weight, dimensions, mobility level, lines, respiratory needs, and the equipment available at bedside.Ground transfer planning
The dispatcher verifies that the ambulance, stretcher, and loading process match the patient and the departure environment.Aircraft interface review
The flight team confirms access path, loading method, onboard configuration, and receiving arrangements.Arrival planning
The destination team prepares the room, receiving staff, and appropriate transfer equipment before the patient lands.
Each step affects the next one. If the hospital uses one sling system, the ground crew uses another, and the flight team needs a different attachment method, somebody may end up doing unnecessary manual repositioning in the middle of the journey.
Ask whether the plan is bed to bed
This is the question that often reveals the quality of the coordination: Who owns the bed-to-bed plan?
If nobody does, pieces get missed.
A transport provider offering bariatric air ambulance coordination should be able to discuss the full sequence, not just the flight segment. That includes who provides the ground leg, how the patient is loaded, what equipment must match across handoffs, and what the receiving team needs before arrival. Med Jets by Air Trek is one example of a service that coordinates these bariatric transport elements as part of air medical planning.
Later in the recovery process, families sometimes ask about seating and home comfort after discharge. A practical non-clinical reference is Gates Furniture's complete recliner guide, which helps explain how lift-style seating differs from transport equipment.
Before a move, some teams benefit from a visual overview of the flow involved.
Where case managers should press for detail
Use direct questions:
- What equipment is used at each handoff
- Will the same sling or transfer method continue across settings
- Who confirms door widths, elevator access, and bedside clearance
- What happens if the sending unit's lift cannot interface with the transport stretcher
Those questions prevent day-of-transfer surprises.
A Checklist for Case Managers and Families
When a bariatric transfer is being arranged, you need something practical. This is the checklist I'd want in front of me during planning calls.
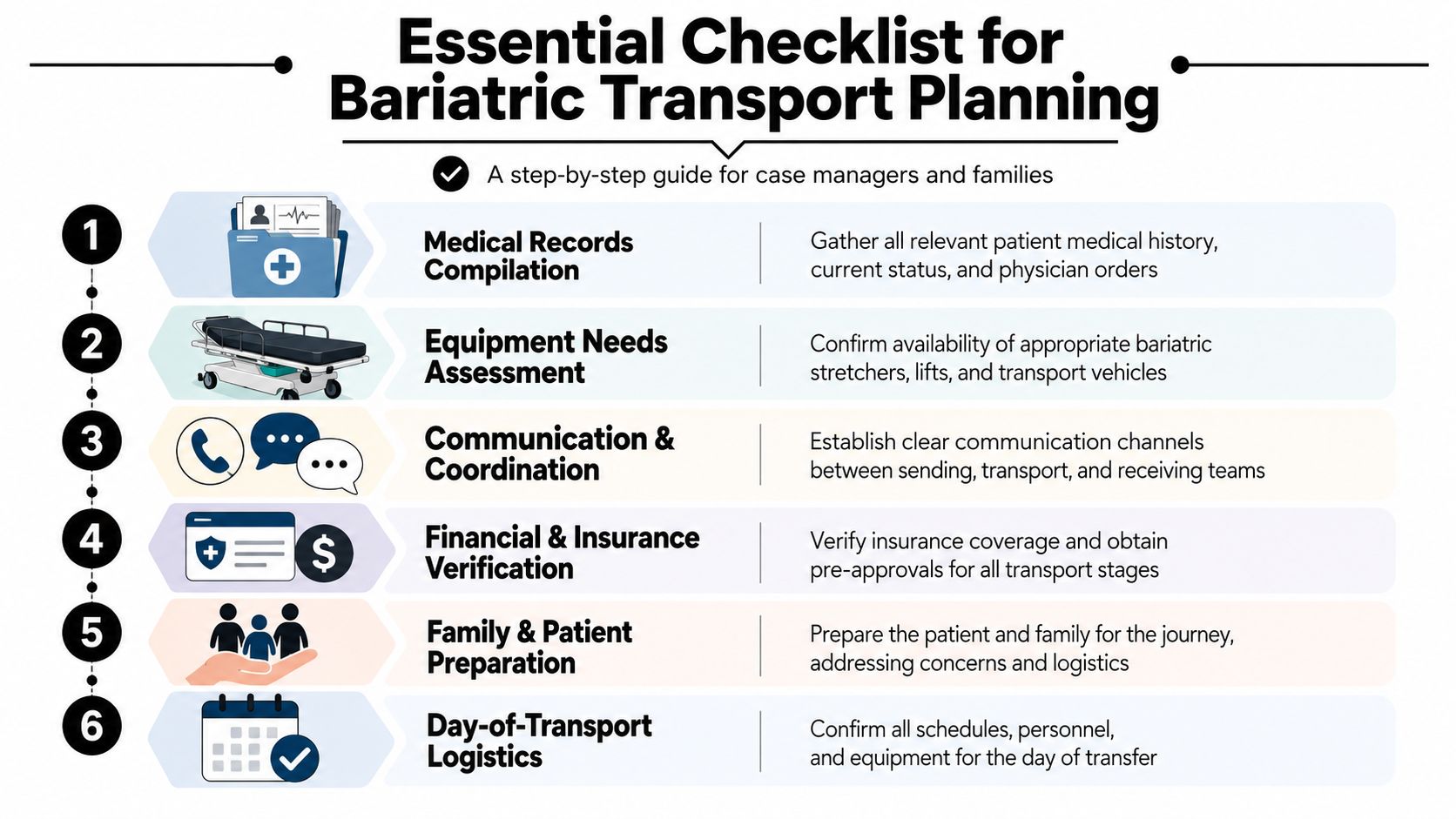
Before transport is scheduled
- Confirm current patient weight: Use the most recent verified weight available. Don't rely on an older estimate.
- Document body dimensions and mobility level: Note width concerns, ability to assist, and any limitations with sitting, standing, or turning.
- List all active medical needs: Oxygen, drains, wound care, cardiac monitoring, or pressure-injury precautions can change the transfer setup.
During provider coordination
- Verify the rating of every lift and stretcher: Ask for the exact equipment planned at the sending facility, ground segment, and air segment.
- Ask about sling selection: Make sure the sling is appropriate for the patient's size and the specific lift system.
- Confirm crew experience: You want a team that routinely handles bariatric transfers, not one improvising on the day.
Checklist cue: If a provider answers in general terms, ask them to walk you through the actual bed-to-bed sequence.
On the day of transfer
- Reconfirm the route: Check room access, hallways, elevators, ambulance loading area, and receiving room setup.
- Clarify who gives the go-ahead: One person should coordinate the transfer timeline and communicate changes.
- Prepare the family: Explain what the patient will see, how long handoffs may take, and why pauses are sometimes necessary for safety.
Here are the questions people often forget to ask:
| Question | Why it matters |
|---|---|
| Does the lift fit the room and the route | Capacity alone doesn't guarantee usable access |
| Is the receiving facility ready with matching equipment | A smooth arrival depends on pre-positioned resources |
| What is the backup plan if conditions change | Delays, room changes, or equipment issues happen |
A printed checklist reduces last-minute confusion and helps families feel informed rather than sidelined.
Bariatric Transport FAQs
Families and case managers usually reach the same final set of questions once the transfer is close. These are the ones that matter most.
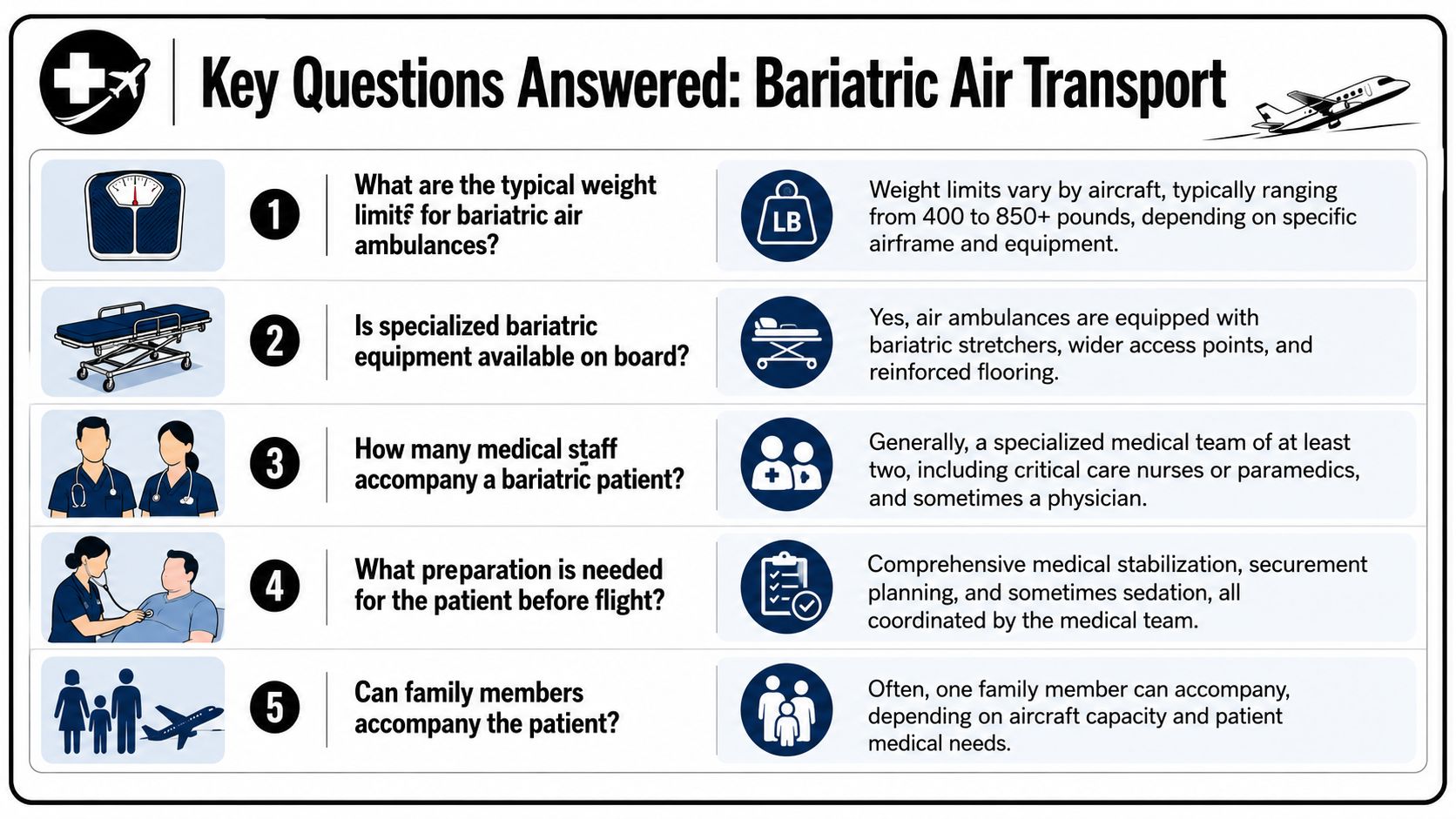
Is a bariatric air ambulance lift the same as a hospital bariatric lift
Not necessarily. There is no widely published, neutral comparison of minimum safe patient weight ratings for air ambulance bariatric lifts versus hospital-grade lifts, leaving families and case managers to rely on operator-specific information rather than codified performance benchmarks, according to this review of gaps in published guidance.
That means you should ask the operator for specifics. Don't settle for “Yes, we handle bariatric patients.” Ask what equipment is used, what its rated capacity is, and how it fits into the loading process.
What does bariatric capability mean in aviation
It should mean more than a marketing label. In practice, it should refer to an aircraft setup, loading plan, stretcher configuration, ground interface, and crew workflow that can safely accommodate the patient being transported.
If you're a case manager, ask: What exactly changes in the plan because this is a bariatric transport? The answer should be concrete.
What if the patient's weight is close to the equipment limit
That should trigger a deeper review, not a quick reassurance. When equipment is close to its threshold, the margin for dynamic movement, positioning changes, and operational error shrinks.
A careful team may decide to change equipment, alter the route, increase personnel, or redesign the transfer sequence.
Can the same sling and transfer method be used from hospital to aircraft
Sometimes yes. Sometimes no. Compatibility depends on the lift system, attachment points, patient condition, and transport setup. That's why handoff planning matters so much.
You want to hear that the teams have already discussed sling compatibility and transfer continuity before pickup.
What should families ask during the first call
Keep it direct:
- What is the exact bariatric equipment plan
- How will the patient move from hospital bed to aircraft stretcher
- What are the clearance or access concerns
- What information do you need from the sending facility today
- Who coordinates the receiving handoff
Ask for the sequence in plain language. If the team can explain the transfer clearly, they're more likely to execute it clearly.
A safe bariatric transfer is rarely about one piece of equipment. It's about whether the entire chain works without forcing the patient or crew into avoidable risk. That's the standard worth holding.