When a doctor says your loved one needs to move to another hospital, the room changes fast. You may hear terms like air ambulance, ICU transfer, flight team, authorization, accepting physician, or bedside-to-bedside coordination. Families often think the next question is only about speed. In reality, the bigger question is whether the patient can be moved without losing the level of care they need right now.
That's where critical care transport comes in.
For case managers, discharge planners, and families, this process can feel overwhelming because medical urgency and logistics arrive at the same time. One team is managing the patient's airway, blood pressure, medications, and monitoring. Another is confirming the receiving facility, transport mode, records, timing, and communication. Both matter. If either side breaks down, the transfer gets harder.
What Is Critical Care Transport
A transfer can become its own phase of treatment.
A patient may be leaving one hospital because the next hospital offers something the current team cannot, such as a trauma service, cardiac intervention, stroke care, neonatal support, transplant capability, or a supervised trip home with medical support. The patient can leave the room, but they still cannot leave ICU-level observation. During that window between beds, the transport team has to protect both the patient's condition and the plan of care.
Critical care transport is the organized transfer of a seriously ill or injured patient while high-acuity treatment continues during the trip. The goal is continuity. Medications still have to run on time. Breathing support still has to be managed. Alarms, rhythm changes, blood pressure shifts, pain control, and sudden deterioration still need trained eyes and hands.
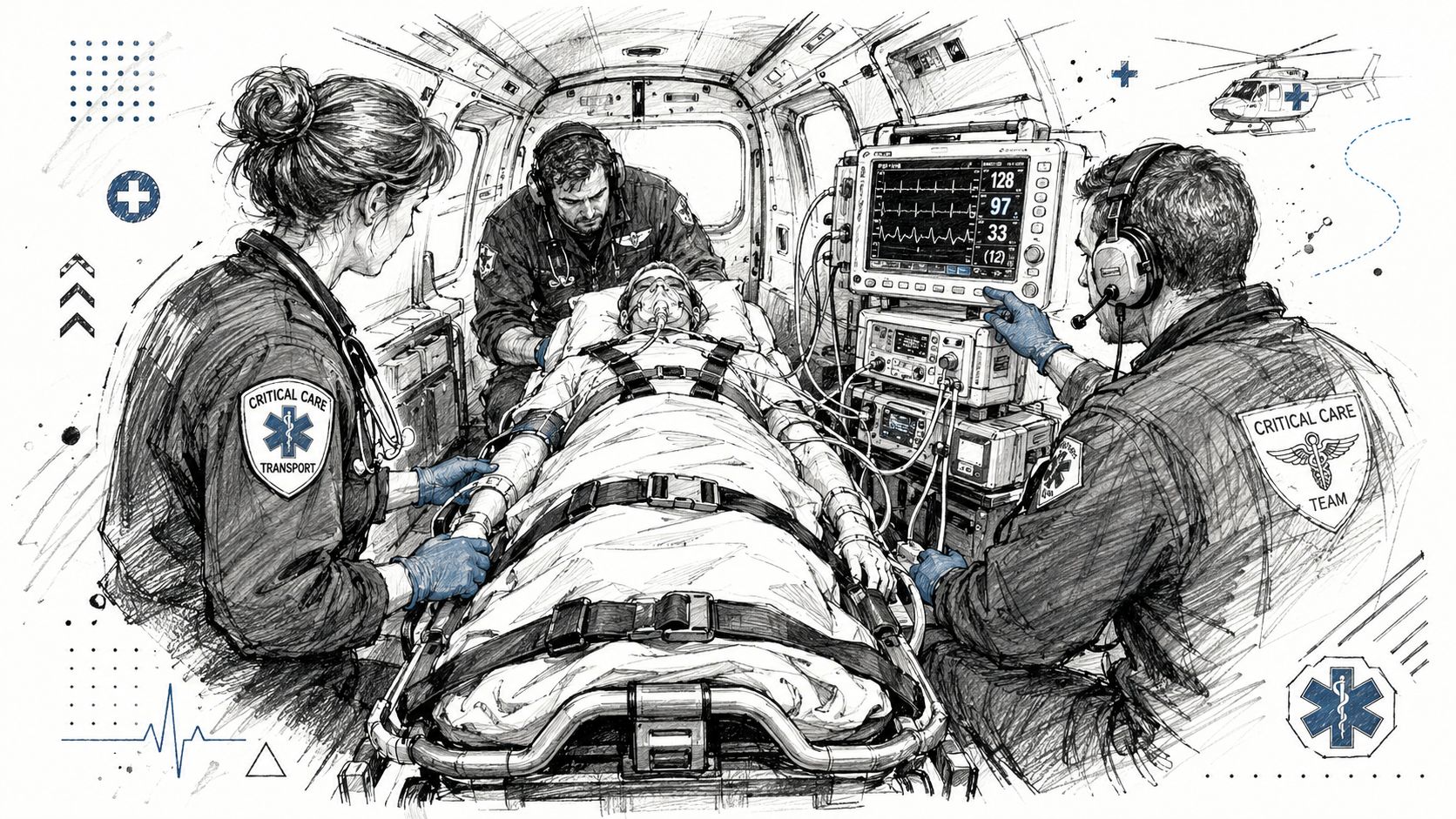
If the patient would normally require close ICU observation in the hospital, the transport team must reproduce enough of that care environment to move the patient safely. That includes advanced monitoring, oxygen delivery, infusion pumps, emergency medications, and clinicians who can make treatment decisions while the ambulance or aircraft is in motion. Families often focus on the vehicle first. The safer question is whether the level of care inside that vehicle matches the patient's current needs.
That distinction matters. A standard medical ride is built to move a patient. Critical care transport is built to move a patient and keep complex treatment going without interruption.
For families, this often relieves one major fear. Your loved one is not being “sent out” and then watched until arrival. A properly arranged critical care transfer includes clinical oversight and logistical coordination at the same time. The sending team, transport crew, receiving team, dispatch staff, and case management all have to stay aligned so that equipment, records, timing, and bedside readiness come together in the right order.
That coordination is one reason preparation matters as much as speed. Even the aeromedical supplies used during high-acuity transport have to match the patient's condition before departure, not halfway through the trip.
People often ask whether this only applies to emergencies. It does not. Some transports are urgent and time-sensitive. Others are planned but medically complicated. The common factor is simple. The patient needs more monitoring, treatment, and clinical judgment than a routine transfer can provide safely.
The Mobile ICU Team Equipment and Protocols
Inside a true critical care transport vehicle, the goal is continuity. The patient shouldn't feel like hospital care stopped and travel started. The trip should function like a controlled extension of the ICU.
Who's on the team
The exact crew depends on the patient and the program. In practice, families may hear about transport nurses, flight paramedics, respiratory therapists, physicians, pilots, drivers, dispatchers, and communication staff. What matters most is not the title alone, but whether the team is trained to care for unstable patients in motion.
These crews work differently from routine transport staff. They do not merely observe. They assess trends, adjust treatment, manage equipment, and prepare for sudden deterioration. If a patient's oxygen level drops or blood pressure changes, they need to recognize it early and respond in a confined, noisy environment.
What the vehicle must carry
Standards for critical care transport vehicles call for them to function as a mobile ICU, including cardiac monitoring with 12-lead capability, non-invasive blood pressure monitoring, defibrillation, cardioversion, transcutaneous pacing capability aligned with ACLS guidance, and the ability to trend and print vital signs and major clinical events during transit (ACCT standards document).
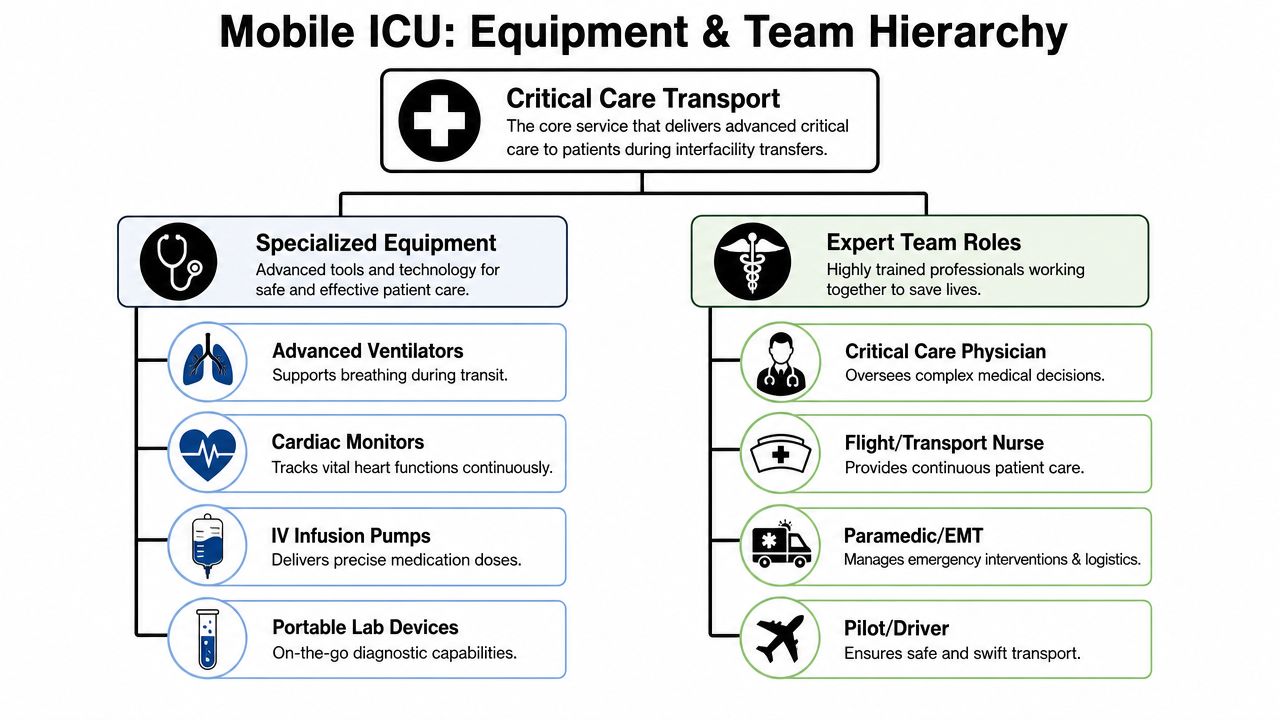
That list can sound technical, so here's what it means in plain language:
- Continuous heart monitoring: The crew can watch rhythm changes in real time and identify dangerous patterns quickly.
- Immediate electrical therapy capability: If the patient develops a life-threatening rhythm problem, the team has equipment to shock, cardiovert, or pace as needed.
- Trend data, not just snapshots: Teams need to see whether the patient is getting better, worse, or staying stable during the trip.
- Reliable power and transport-ready setup: Equipment has to work continuously, even through loading, unloading, and handoff.
For families trying to understand the gear involved, a provider's overview of aeromedical supplies and transport equipment can help make the setup more concrete.
Why protocols matter so much
Good critical care transport isn't built on improvisation. It's built on preparation. Before departure, the crew reviews the diagnosis, current therapies, airway status, medication drips, recent changes, destination, route, and contingency plans.
Practical rule: The safest transfer is usually the one where the crew already knows what they'll do if the patient worsens before that problem actually happens.
That's why experienced teams spend time on checklists and handoff details. Families sometimes worry when the crew appears to pause before leaving. In most cases, that pause is a sign of caution, not delay. They're making sure the patient can travel with the same level of vigilance they were receiving in the hospital.
Choosing Between Air and Ground Critical Care Transport
The most common transport question is simple: Should this patient go by ground or by air? The answer depends on more than distance.
A commonly cited rule of thumb suggests ground transport for under 50 miles, helicopter for 50 to 150 miles, and fixed-wing aircraft for more than 150 miles, but the same review stresses that total transport time and mission constraints can matter more than mileage alone. It also notes that in time-sensitive conditions such as stroke, myocardial ischemia, intracranial hemorrhage, and severe injury, aeromedical transport may save time even over shorter distances (review of transport mode selection).
That means a shorter trip isn't automatically a ground trip. A hospital on the map may be nearby, but traffic, road access, loading delays, weather, landing options, and the patient's condition can change the decision.
A side by side view
| Factor | Fixed-Wing Air Ambulance | Ground Ambulance |
|---|---|---|
| Best fit | Longer interfacility transfers, regional or international moves | Shorter transfers, local and regional hospital moves |
| Time profile | Fast over long distances, but includes airport and ground coordination on both ends | Direct bedside-to-bedside route in many local moves |
| Access | Needs airport logistics and coordinated ground legs | Reaches hospitals directly by road |
| Weather sensitivity | Can be affected by aviation conditions and scheduling variables | Can be affected by traffic, road closures, and local driving conditions |
| Cabin environment | Built for medical flight operations, with aircraft-specific constraints | More familiar loading and unloading process for many facilities |
| Family decision point | Useful when the destination is far away or crossing regions | Useful when distance is modest and direct access matters most |
A more detailed overview of fixed-wing and rotary-wing transport differences can help when a team is choosing among aircraft options rather than deciding between road and air.
Questions that sharpen the choice
Families and case managers usually get better answers when they ask focused questions such as:
- How urgent is the specialty care need? If treatment at the receiving center can't wait, speed may carry more weight.
- How stable is the patient right now? Some patients tolerate movement poorly and need a mode that best supports safe monitoring and intervention.
- What does the full trip look like? Total time includes loading, departure prep, travel, arrival coordination, and handoff.
- What could disrupt this plan? Weather, airport access, traffic, and bed availability all affect the actual timeline.
The right mode is the one that gets the patient to the correct level of care with the fewest avoidable risks, not simply the fastest machine available.
That distinction matters. Families sometimes hear “air” and assume it's automatically more advanced. Sometimes it is the right tool. Sometimes a well-equipped ground critical care unit is the cleaner, safer choice. The decision should reflect the whole mission, not one dramatic part of it.
How Medical Transfers Are Arranged
At 2 a.m., a family may see only one moment. New faces enter the room, monitors are checked, papers are signed, and the patient is prepared to leave. What feels sudden at the bedside usually reflects many small decisions already made between hospitals, physicians, coordinators, and the transport team.
A transfer starts once the current medical team decides the patient needs care that the present facility cannot provide or cannot continue to provide safely. The next step is acceptance by the destination hospital, unit, and physician. Then coordination shifts into motion. Staff match the patient's condition to the right crew, equipment, timing, route, and receiving plan.
That coordination matters because a transfer is not one event. It works like a relay race. The sending team, receiving team, transport coordinator, bedside nurse, insurer or assistance company, and transport crew each carry one part of the handoff. If one person misses a detail, the whole timeline can slow down.
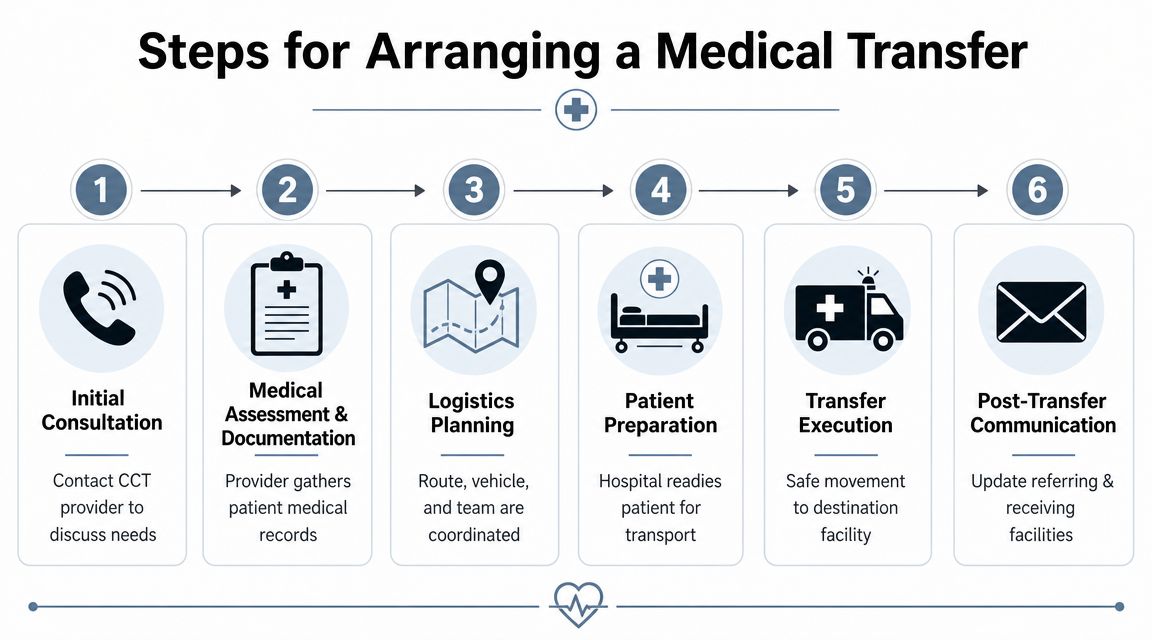
The usual sequence
Clinical decision
The treating physician determines that transfer is medically necessary. The reason may be a higher level of monitoring, a specialist service, surgery, advanced imaging, or ongoing ICU support that is unavailable at the current hospital.Receiving facility acceptance
The destination confirms more than interest. It must have the right bed, the right service, and a physician willing to accept the patient.Record and status review
The coordinator gathers the information the crew will need to move the patient safely. That usually includes diagnosis, allergies, medications, airway status, drips, recent vital trends, code status, isolation precautions, and whether imaging or records have been sent ahead.Authorization and financial review
Depending on the situation, staff may contact insurance, an employer assistance program, a medical assistance company, or the family member making decisions. If you need a plain-language overview before giving consent, this guide to medical flight transport cost factors can help you ask better questions.Mission planning
The transport service assigns the crew and vehicle, confirms any special equipment, and works out timing with both facilities. A patient on multiple infusions or a ventilator may need a different crew setup than a stable patient who still requires close monitoring.Bedside handoff and transfer
At departure, the crew receives report, checks equipment, verifies medications and lines, and prepares the patient for movement. At arrival, they give a full handoff so the receiving team can continue care without gaps.
Why communication systems matter
Families often focus on the ambulance or aircraft because it is the visible part of the process. The harder work is usually coordination. Someone has to keep the sending unit, accepting hospital, transport crew, and financial contacts aligned on the same plan at the same time.
That is why one clear point of contact helps so much. In some systems, a dedicated coordination hub handles updates, confirms details, and reduces repeated phone calls between departments. For a non-clinical look at that layer, the strategic value of a medical call center shows how organized communication supports urgent healthcare operations.
A useful question for families is: “Who is coordinating the transfer right now, and how will I get updates?”
For case managers, the highest-value work is often quiet and methodical. Confirm the accepting physician. Confirm the bed. Confirm that key records go with the patient or arrive before the patient does. Confirm that the crew knows about oxygen needs, infusions, infection precautions, and any device that cannot be interrupted during the trip.
Those checks may sound simple. In critical care transport, simple checks prevent complicated problems.
A Checklist for Patients Families and Case Managers
When people are stressed, they don't need more theory. They need a short list they can trust.
For families at the bedside
- Have identification ready: Bring the patient's ID, insurance information, and basic contact details for the person who can make decisions if needed.
- Ask what travels with the patient: Glasses, hearing aids, a phone, legal paperwork, and comfort items may or may not go during transport. Ask before packing.
- Confirm communication expectations: Find out who will update you during the trip, when you'll hear after arrival, and whether a family member may accompany the patient.
- Bring medication information if asked: The hospital usually handles active inpatient medication records, but family-supplied medication lists can still be helpful when histories are incomplete.
- Keep one notebook or phone note: Write down names, direct numbers, destination details, and the receiving unit so you don't have to reconstruct it later.
For case managers and discharge planners
- Verify acceptance: Don't assume the receiving facility, physician, and bed are all aligned until they are clearly confirmed.
- Prepare a clean handoff packet: Include the diagnosis, recent notes, medication list, allergies, code status, isolation status, imaging status, and any special equipment needs.
- Clarify timing windows: A team can be ready and still be delayed by bed turnover, weather, or airport-ground coordination. Build in communication around those realities.
- Flag non-obvious risks: Bariatric requirements, language needs, behavioral concerns, or device-specific support should be communicated early, not at loading time.
- Identify the escort rules: Families often assume accompaniment is automatic. It isn't. Confirm it with the provider.
Questions worth asking before departure
- What level of crew is assigned to this patient?
- What equipment support will continue during transport?
- Who calls the family on arrival?
- What happens if the destination changes or the patient worsens?
- What documents need signatures before departure?
A good checklist doesn't remove the seriousness of the moment. It does make the moment more manageable. That matters because calm, organized handoffs usually support safer transfers.
Why Choose Med Jets by Air Trek for Your Transport
Some providers focus only on getting a patient airborne. A better standard is making sure the patient is ready for transport, then matching the mission, crew, and equipment to the actual medical need.

That approach lines up with a longstanding point in critical care transport literature: bringing ICU-level care to the patient and prioritizing stabilization before departure is often more important for outcomes than only reducing travel time (classic discussion of stabilization over speed). Families sometimes find that surprising, but clinicians usually don't. A rushed departure can be the wrong departure.
What to look for in a provider
If you're comparing air medical programs, focus on practical fit:
- Aircraft configuration: Can the aircraft support the patient's monitoring, oxygen, and treatment needs during flight?
- Care continuity: Is the service organized around bedside-to-bedside coordination instead of just the air segment?
- Special-case capability: Some patients need bariatric planning, multiple escorts, or international coordination.
- Communication: Can the company coordinate with hospitals, families, and case managers around the clock?
One example is Med Jets by Air Trek, a long-running air ambulance provider that coordinates emergency medical flights, medical escorts, and ground segments, with aircraft described by the publisher as configured for one to two patients plus accompanying family and support for specialized transfer needs.
What reassurance should actually sound like
The most reassuring provider isn't the one that makes the trip sound easy. It's the one that explains the plan clearly.
That includes how the patient will be monitored, what happens before departure, who handles records, whether a family member can travel, what the ground legs look like, and how the receiving hospital handoff will be managed. Clear answers are a sign that the service is built around operations, not just marketing.
A short look inside the transport environment can help make that more tangible:
When families ask, “Why can't we just leave now?” the safest answer is often that the crew is doing what a careful ICU team would do on the ground. They're checking lines, medications, monitoring, power, oxygen, documentation, and the route. That isn't hesitation. That's transport medicine done correctly.
Answering Your Critical Transport Questions
How is the cost of critical care transport determined
Cost usually depends on the transport mode, distance, clinical crew required, ground coordination, and how much bedside-to-bedside logistics the provider is handling. International flights, specialty staffing, and complex equipment needs can also affect pricing. The cleanest way to understand cost is to ask for an itemized explanation of what's included in the mission.
Will insurance cover it
Coverage varies by plan, medical necessity criteria, location, and whether the transfer is authorized in advance. Families should ask both the hospital team and the transport coordinator what documentation is being submitted and who is handling authorization. Don't assume approval, but don't assume denial either.
Can a family member travel with the patient
Sometimes yes, sometimes no. It depends on the aircraft, the patient's condition, crew requirements, safety limits, and operator policy. Ask early, because accompaniment rules may affect how family travel is arranged on the destination side.
What happens if the patient gets worse during the trip
That possibility is one reason critical care transport exists. Research shows safety events occur in a meaningful share of transports, with new or recurrent hypoxia identified as the most frequent adverse event type, and transport duration found to be a significant predictor of risk in one study of critical care transport. Related urgent air-medical research found an in-transit critical event in 1 out of every 20 transports of adult patients (patient safety research on PubMed). The practical takeaway is simple. Experienced crews, close monitoring, and careful mission planning matter because patient condition can change en route.
Is faster always better
Not always. In some conditions, time is central. In others, the patient needs additional stabilization before moving. Families often feel pressure to leave immediately, but the safer decision may be to secure the airway, optimize oxygenation, clarify medication support, or confirm hemodynamic stability before departure.
What about international medical transport
International transfers add layers such as passports, customs, receiving arrangements, airport handling, and sometimes multiple handoffs. The core principle stays the same. The trip should be organized so care continues without gaps from the sending location to the destination team.
If you're arranging a transfer right now, ask for one person to walk you through the whole chain. Current bedside status, receiving facility, transport mode, family communication, records, and arrival plan. That conversation usually brings the most clarity when everything feels urgent.
If you need help evaluating transport options for a current patient, ask the provider for a bed-to-bed plan in writing. It's the fastest way to see whether the medical care, logistics, and communication are all lined up before the patient moves.