A medical emergency rarely unfolds in a clean, predictable sequence. A spouse collapses while traveling. A parent is admitted to a small community hospital after a stroke. A child is stabilized in one emergency department, then the staff says the hospital can't provide the specialist care that's needed next.
That's the moment many families realize emergency medical response is bigger than a 911 call and a ride to the nearest ER.
From the operations side, the core work is a chain of decisions. Someone answers the call. Field crews triage and stabilize. A physician decides whether the local hospital can manage the case. A receiving facility has to accept the patient. Transport has to match the patient's condition, distance, weather, and timing. If the case crosses regions or states, coordination gets even tighter. Families and case managers aren't just asking, “How do we get help?” They're asking, “How do we get the right help, to the right place, without losing time or safety?”
What Is Emergency Medical Response Really
A family on vacation in a rural area calls 911 after a loved one develops crushing chest pain. The local ambulance arrives, the nearest hospital begins treatment, and everyone assumes the crisis is now contained. Then the physician explains that the patient needs a higher level of cardiac care at a different facility.
That second phase is still emergency medical response.
In the United States, EMS responds to an estimated 37 million 911 calls each year, with an average response time of about 7 minutes from call to arrival on scene. The same research found response times rise to more than 14 minutes in rural settings, and nearly 1 in 10 encounters wait almost 30 minutes for EMS arrival, according to this EMS response time analysis. Those numbers matter because they show how much location changes what happens next.
Response is a system, not a single event
The phrase is often understood to mean “ambulance arrives.” In practice, it includes several linked handoffs:
- Call intake and dispatch: Someone identifies the complaint, location, and urgency.
- On-scene medical care: EMTs or paramedics assess airway, breathing, circulation, mental status, and immediate threats.
- Transport to the first appropriate facility: Not always the final facility.
- Hospital evaluation and escalation: The local team decides whether the patient needs trauma, burn, stroke, cardiac, neonatal, or other specialty services elsewhere.
- Inter-facility transfer coordination: Transport is arranged with the right crew, equipment, and destination.
If you're a family member, this is why a case can feel like it keeps changing. It is changing. The patient's needs become clearer as tests, exams, and specialist reviews come in.
Practical rule: The first hospital is often the safest place to stabilize a patient. It isn't always the hospital that can finish the job.
Why families get caught off guard
People usually prepare for the emergency itself, not the transfer that follows. They may have a wallet card and insurance information, but no clear plan for who should be called, where records are stored, or how decisions get made if the patient can't speak for themselves. A simple preparedness step is keeping a current list of medications, diagnoses, and decision-makers, like this guide on managing emergency contacts for loved ones.
When a local hospital isn't sufficient, emergency medical response becomes a coordination problem as much as a clinical one. The question is no longer only “Can we treat this patient now?” It becomes “Where can this patient get the care they need next, and how do we move them safely?”
The First Hour Triage and Stabilization
The first hour is about control. Not comfort. Not convenience. Control.
Firefighters don't start by rebuilding a house. They stop the fire from spreading. Medical teams work the same way. They contain immediate threats first, then decide what kind of transport the patient can tolerate.
What crews are doing at the bedside or on scene
Families often see activity without knowing what it means. In those first minutes, clinicians are answering a short list of urgent questions:
- Is the airway open and protected?
- Is the patient oxygenating and ventilating adequately?
- Is circulation failing from bleeding, shock, arrhythmia, or another cause?
- Is there a time-sensitive diagnosis that changes destination decisions?
- Can the patient be moved safely right now, or do they need more stabilization first?
That's why the room can feel repetitive. Blood pressure gets checked again. Oxygen levels are trended. Mental status is reassessed. Pain control may be balanced against blood pressure or breathing. A patient may look calmer while the team is still concerned, or look dramatic while the condition is becoming more stable.
Stabilize first, then move
Transport is not treatment by itself. Transport creates new risks. Movement can worsen bleeding, agitation, airway problems, spinal pain, or unstable blood pressure. Loading a patient too early can turn a manageable case into a dangerous one.
Common early priorities include:
- Airway support: Oxygen, suction, positioning, or advanced airway management if needed.
- Monitoring: Cardiac rhythm, oxygen saturation, blood pressure trends, and neurologic checks.
- Access and medication: IV or other access, fluids when appropriate, and medications for pain, seizures, rhythm problems, allergic reactions, or sedation.
- Immobilization or packaging: Splinting, spine precautions when indicated, pressure offloading, and secure transfer setup.
If the team seems slow, ask whether they're delaying transport or preparing for safe transport. Those are not the same thing.
A transfer done ten minutes later with the right support is often safer than an immediate departure with an unstable patient.
The question families should ask
A useful question is not, “Why aren't we moving yet?”
Ask, “What has to be stabilized before transport is safe?”
That changes the conversation. It gets you specific answers about blood pressure, oxygen needs, airway protection, bleeding control, pain management, or the need for a specialist team. It also helps you understand why some patients can go by standard ground unit while others need a critical care crew or aircraft.
For a broader patient-family explanation of why early treatment windows matter, Med Jets has a helpful overview of the medical golden hour. The principle is simple. Fast matters, but appropriate fast matters more.
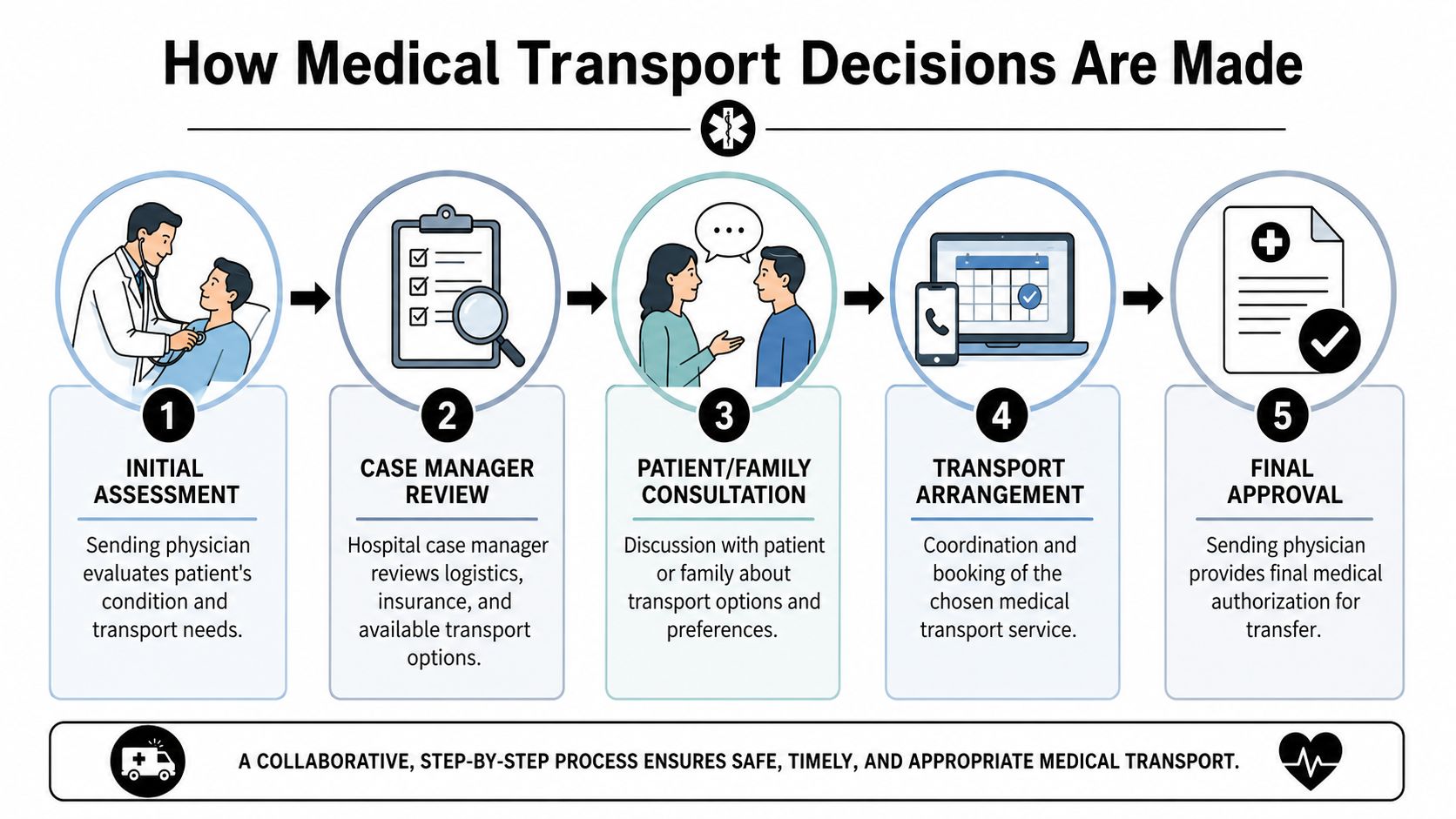
How Medical Transport Decisions Are Made
Once the patient is stabilized enough to move, the decision shifts from “Can we transport?” to “What transport matches the risk?”
That choice is rarely made by one person alone. It's a coordinated judgment call between the physician, the hospital team, the transport coordinator, and often the family.
A quick visual helps frame the workflow.
Who decides what
The sending physician determines medical necessity. That physician decides whether the patient needs a higher level of care and what kind of monitoring or intervention must be available during transport.
The case manager or discharge planner handles the operational side. That usually includes records, authorizations, payer coordination, bed availability, and communication with transport vendors.
The family provides consent, history, preferences, and practical information. Families also surface issues the chart may not capture well, such as baseline cognition, caregiver availability, or whether the receiving hospital is close to the patient's support system.
What drives the transport choice
The core criteria are usually these:
- Clinical condition: Does the patient need advanced airway care, vasoactive medications, cardiac monitoring, or a critical care crew?
- Distance: Some transfers are short enough for ground. Others become unsafe or impractical if travel time is too long.
- Time sensitivity: Stroke, cardiac, trauma, neonatal, and specialty surgical cases may need faster access to a receiving center.
- Terrain and access: Congestion, mountain roads, island geography, and remote pickup points change the equation.
- Weather and aviation limits: Aircraft availability is never a blank check. Safe flying conditions still govern.
Geography matters more than many families realize. The CDC and HRSA note that rural EMS systems are often overstretched and underfunded, making long-distance ground transport difficult or impossible in some settings, as outlined in the CDC's review of EMS disparities in rural communities.
A transport recommendation isn't just about speed. It's about whether the patient can reach definitive care without losing ground en route.
How the conversation usually sounds
A sending physician may say, “The patient is stable enough to transfer, but not for routine transport.” That often means the patient isn't crashing, yet still needs more support than a basic ambulance can provide.
A case manager may say, “We're looking at the receiving facility, crew level, timing, and coverage.” That's not bureaucracy for its own sake. It reflects the fact that every transfer has both a clinical and logistical side.
Later in the process, families often want to see the kind of coordination they're being asked to trust. This short video gives a useful overview of transport planning in motion.
When the decision is made well, the transport mode fits the patient, not the other way around.
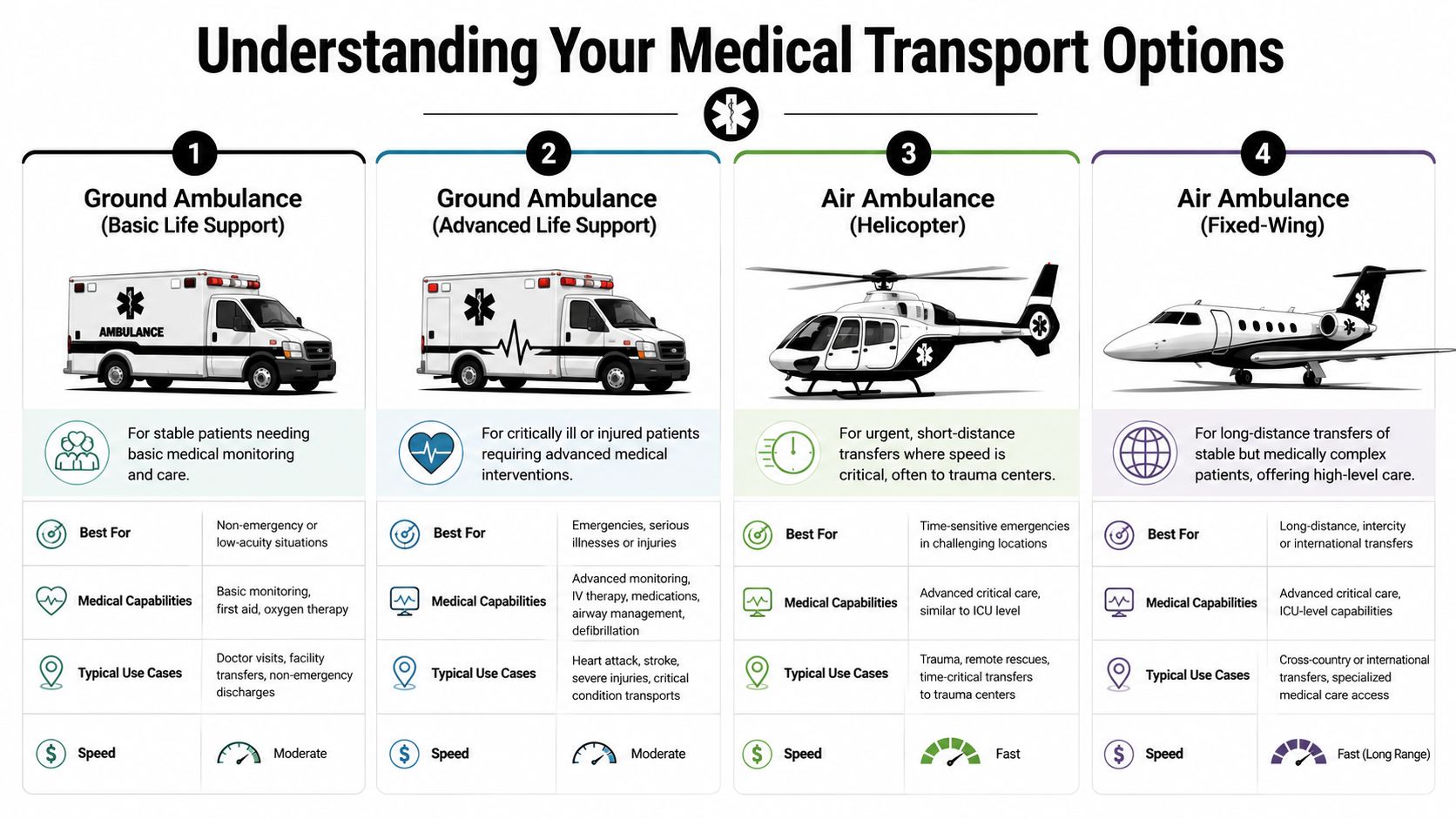
Understanding Your Medical Transport Options
Not every ambulance does the same job. Not every aircraft should be used for the same patient. The safest choice depends on range, cabin space, crew capability, and what might happen during the trip.
This side-by-side view is a useful starting point.
Ground ambulance
Ground remains the right answer for many transfers.
Basic Life Support units fit patients who are stable and need transport, observation, and routine support. These are often appropriate when the patient doesn't require advanced medication infusions, invasive airway management, or continuous critical interventions.
Advanced Life Support units are used when the patient may need more complex monitoring or treatment during transport. If the patient's condition could change on the road, ALS is often the floor, not the ceiling.
Ground transport works well when the receiving hospital is reasonably accessible and road time won't create added risk. It becomes less attractive when distance is long, road conditions are poor, or staffing a multi-hour ground transfer pulls scarce crews away from local 911 coverage.
Helicopter
Helicopters are built for urgency over shorter distances and for places where roads create a major delay. They're often useful for scene calls, trauma routing, and transfers to regional specialty centers.
The trade-off is cabin environment. Space is tighter. Noise is higher. Access to the patient can be more constrained than in a larger vehicle or jet. Weather can also shut down rotary-wing missions quickly.
A helicopter solves one problem very well. It shortens time over difficult geography. It doesn't solve every problem.
Fixed-wing air ambulance
Fixed-wing transport becomes more useful as distance increases and the transfer starts to look less like a local hop and more like an inter-state or cross-country clinical handoff. The cabin is usually better suited to longer-duration care, more equipment, and a more controlled working environment.
That matters for medically complex patients, fragile older adults, and larger patients who need more room, lifting support, and careful positioning. When hospitals need long-distance transfer with bedside-to-bedside coordination, a service such as Med Jets by Air Trek's emergency medical transport services is one option used for fixed-wing air ambulance, medical escort, and coordinated ground legs.
A simple comparison
| Transport type | Best fit | Main strength | Main limitation |
|---|---|---|---|
| Ground BLS | Stable patients with basic monitoring needs | Widely available | Limited advanced intervention capability |
| Ground ALS | Patients needing higher monitoring or treatment en route | Strong short-to-medium range option | Long trips can be hard on patient and local coverage |
| Helicopter | Urgent short-range or hard-access transfers | Fast over traffic or terrain | Tight cabin and weather sensitivity |
| Fixed-wing | Long-distance inter-facility transfer | Better range and cabin environment | Requires airport coordination and ground links |
The mistake families make most often is assuming faster always means better. The better question is whether the crew and platform can safely deliver the patient in the condition they're in now.
Navigating Documentation and Insurance Approval
Transport can be arranged quickly, but approval still depends on documentation. When cases stall, it's often because the chart doesn't yet tell the transport story clearly enough for the next team or the payer.
The most important document in this chain is usually the electronic patient care report, or ePCR.
Why the paperwork matters clinically
An ePCR isn't just a billing form. It captures what happened, what was found, what was done, and how the patient responded. Columbia Southern notes that close to 75% of EMS providers use ePCR to collect more than 400 data points per patient encounter, supporting continuity of care and downstream reimbursement in EMS systems, as described in its overview of the importance of data in EMS.
For a transfer team, that record helps answer practical questions fast:
- What changed today: New neurologic deficit, worsening oxygen need, failed extubation, post-op complication.
- What support is active: Oxygen delivery, drips, monitoring, precautions, isolation needs.
- Why the patient can't go by routine means: Clinical risk during transport, need for specialty destination, or inability of the local facility to provide required care.
What insurers usually need to see
Families often hear the phrase medical necessity without anyone translating it. In transport, it usually means the records must show why this patient needs this level of transport to this destination at this time.
That means gathering:
- Physician transfer order
- Current clinical summary
- Nursing notes and recent vitals
- Medication list and active infusions
- Receiving facility acceptance
- Insurance details and prior authorization contacts
If you're sorting out the payment side, it helps to understand the difference between coverage for the care itself and coverage for the transport platform. This explanation of whether insurance covers air ambulance is a practical place to start.
Documentation advice: Ask the hospital team, “What in the chart shows why this transport level is medically necessary?” If they can answer that clearly, authorization usually moves more smoothly.
Where coding and claims support fit
Case managers and billing teams also run into coding questions after the trip, especially with complex transports and specialty-level documentation. In those situations, outside resources such as specialty EMS coding support can help teams interpret documentation requirements and reduce claim friction.
Families don't need to master coding language. They do need to know that vague notes create delays. Specific records move patients.
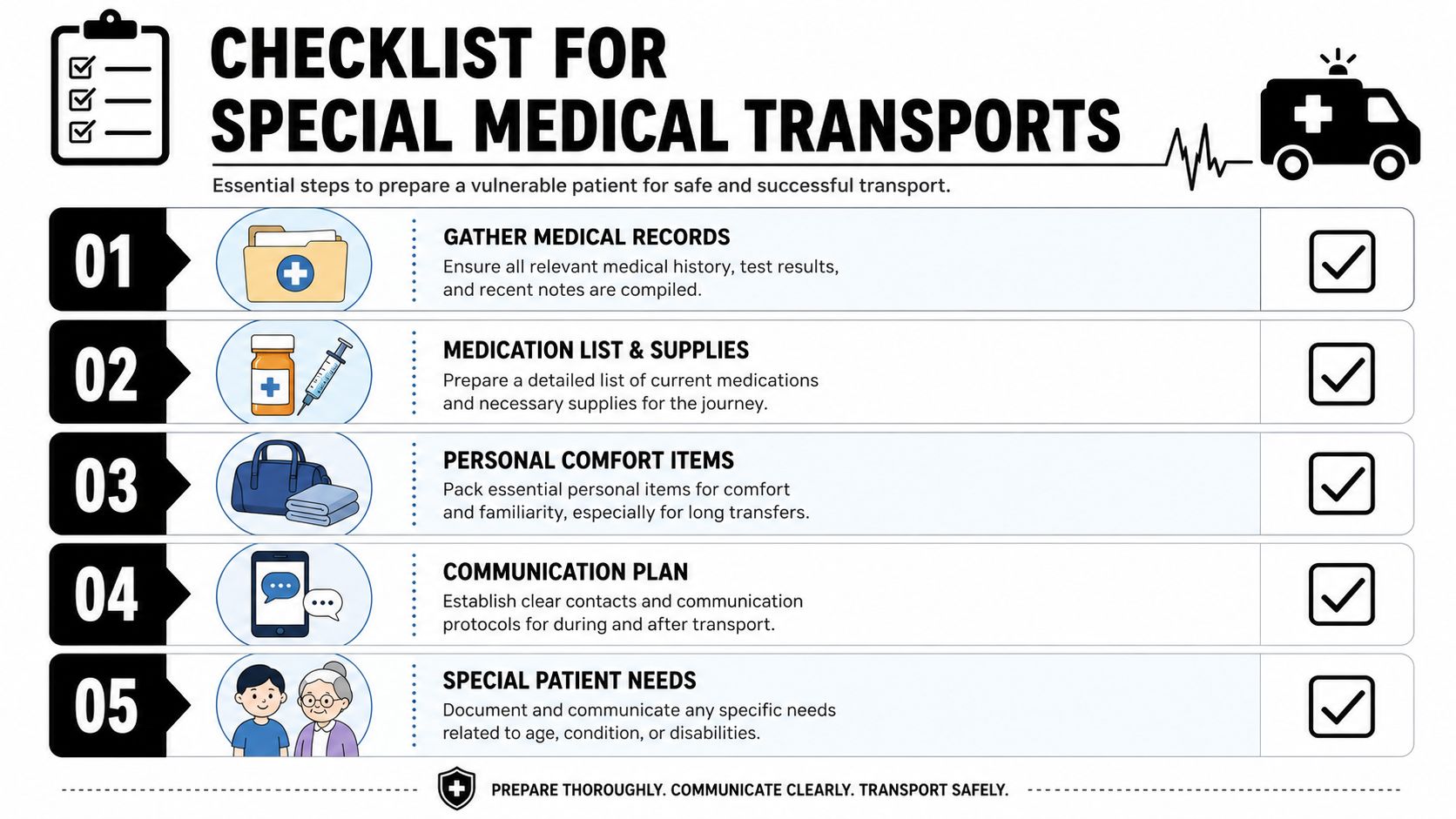
Checklist for Special Medical Transports
Special transports go more smoothly when the sending team, family, and transport coordinator all work from the same preparation list. The details change by patient type, but the pattern is consistent. Gather the record, confirm the meds, prepare the patient, and remove avoidable surprises.
Preparation points by patient group
Pediatrics
- Confirm pediatric capability: Ask whether the crew has the right size equipment, medication dosing process, and age-appropriate monitoring.
- Clarify parent presence: Find out whether one parent or guardian can accompany the child and what identification is needed.
- Bring comfort items: A familiar blanket, toy, or tablet can reduce fear and movement during transfer.
Seniors
- Review baseline status: Tell the team what's normal for cognition, mobility, hearing, and communication.
- Check medication timing: Missed doses matter during long transfers, especially for cardiac, seizure, or Parkinson's medications.
- Plan pressure relief and positioning: Frail skin, joint pain, and delirium risk all increase when transport is prolonged.
Bariatric patients
- Verify lift and loading plan: Don't assume standard equipment will work safely.
- Ask about cabin space and stretcher limits: The right aircraft or ground unit has to be assigned from the start.
- Confirm enough trained personnel: Moving the patient safely may require added hands and a specific packaging approach.
Patients traveling with pets
- Ask early, not late: If a companion animal is part of the relocation or recovery plan, mention it at the first coordination call.
- Separate medical from pet logistics: The patient's clinical needs come first, but pet planning can often be coordinated alongside the trip.
- Prepare records and carrier needs: Vaccination and handling details may matter depending on route and destination.
Medical Transport Preparation Checklist
| Category | Action Item / Question to Ask | Notes |
|---|---|---|
| Medical records | Has the full chart, transfer summary, and receiving acceptance been sent? | Confirm who faxed or uploaded it |
| Medications | Is there a current medication list with last dose times? | Include drips and PRN meds |
| Equipment needs | Does the patient need oxygen, suction, ventilator support, or specialty positioning? | Match this to vehicle capability |
| Family communication | Who gets updates during departure, transit, and arrival? | Name one primary contact |
| Pediatric issues | Can a parent travel, and is pediatric equipment confirmed? | Ask before dispatch |
| Senior care | What is the patient's baseline cognition and mobility? | Document hearing and vision needs too |
| Bariatric planning | Is specialized loading equipment required? | Don't leave this to day-of transport |
| Personal items | What can safely travel with the patient? | Keep valuables with family when possible |
| Pets | Can pet arrangements be coordinated separately? | Raise this at intake |
| Arrival planning | Who meets the patient at the destination? | Confirm unit, floor, and contact person |
A good checklist doesn't add work. It prevents the wrong kind of work at the worst time.
Coordinated Care FAQs and Case Examples
Families usually don't need more theory at the end of a transfer discussion. They need straight answers.

Who arranges the ground transportation to and from the airports
In a coordinated inter-facility transfer, the transport coordinator typically works both ends of the trip. That means ground from the sending hospital to the departure airport, then ground again from the arrival airport to the receiving hospital if fixed-wing is used.
A common failure point is assuming the aircraft booking includes those legs automatically. Sometimes it does. Sometimes it has to be ordered separately. Ask for the movement plan in plain language: pickup point, airport handoff, arrival handoff, and destination bed.
Can a family member travel with the patient
Sometimes yes, sometimes no. The answer depends on the patient's condition, the aircraft layout, weight and balance, infection control concerns, and the crew's need for workspace.
The practical question is not “Do you allow riders?” Ask, “If a family member can't ride, who will update us at each handoff?” Good coordination includes a communication plan, not just a seat assignment.
The calmer transfer is often the one where everyone knows who calls whom at departure, arrival, and receiving admission.
What if the patient is far from home
Optimal end-to-end coordination is essential. A patient may start at a small hospital, transfer to a specialty center, then later need a medically supported move closer to home for ongoing recovery. Each leg has different clinical and administrative requirements.
In those cases, one point of contact helps. The coordinator tracks the sending physician's order, receiving acceptance, records packet, ground links, and timing so the family isn't left stitching together four vendors and two hospitals on their own.
What happens if plans change midstream
They often do. Weather changes. Receiving beds change. A patient who looked stable at noon may need a different crew by evening. That doesn't mean the system failed. It means the system is adapting to the patient.
The safest teams are transparent about those changes. They explain what changed, what the new plan is, and what the family should expect next.
Emergency medical response works best when it stays coordinated from first call to final handoff. For families and case managers, that coordination is what turns a frightening transfer into a manageable one.
When a local hospital can't provide the next level of care, the transfer becomes part of the emergency. The right question isn't only how fast the patient can move. It's how safely, with what crew, to which facility, and with what documentation behind them. Families remember the stress. Clinicians remember the handoffs. Good emergency medical response respects both.