A hospital case manager is trying to arrange a transfer before the receiving ICU bed is released. A daughter is on her phone asking, “Will someone actually be able to care for my dad on the plane?” A spouse is wondering whether a nurse on a private jet is the same thing as a medical escort on a commercial flight.
Those questions are common, and they matter.
When people hear medevac flight nurse, they often picture someone checking vital signs during transport. The role, however, is much more involved. Public information often flattens the role into a job title, even though the work is both clinical and operational, which is one reason families can feel unsure about what level of transport is appropriate for the patient they love, as noted in this Air Force Reserve overview of flight nursing.
A good medical flight doesn't begin at takeoff. It starts with a careful bedside assessment, a plan for what could go wrong in transit, and a clinician who knows how to keep a fragile patient stable in a very small, very demanding environment.
That's where the flight nurse comes in. Think of this role as the person who helps turn an aircraft cabin into a working treatment space, not just a seat with oxygen. If you're arranging a transfer for a stroke patient, a ventilated ICU patient, a senior with multiple medications, or a bariatric patient who needs specialized handling, understanding what the nurse does can make the decision far less overwhelming.
When Your Loved One Needs to Fly
The call often comes fast. Your loved one is stable enough to move, but not stable enough to travel like a typical passenger. The local hospital may not offer the specialty care they need. The receiving team is waiting. Every hour feels heavy.
In that moment, families usually ask practical questions, not technical ones. Who will watch the breathing? What if blood pressure drops in the air? Who talks to the sending hospital, the receiving hospital, and us?
Why the job title can be misleading
A medevac flight nurse isn't merely there for transport. The role combines bedside critical care, transport medicine, and mission coordination. That means the nurse may help determine what equipment must be loaded, what medications need to be ready before departure, how the patient should be positioned, and whether the current condition calls for a dedicated air ambulance rather than a lower-acuity option.
Families often feel calmer once they understand that the nurse's role includes active treatment decisions, not just observation.
This is one of the biggest sources of confusion in air medical transport. Consumer-facing descriptions often compress the role into “nurse on board,” which leaves out the part families care about most. Who manages risk during the transport interval?
What families usually want to know first
Most bedside conversations come down to a short list:
- Can my loved one be treated during the flight? In a proper medevac setting, yes. The nurse is there to provide ongoing care, not just monitor.
- Will the nurse understand complex conditions? For high-acuity transport, that should be expected.
- Is this the same as a commercial medical escort? No. Those can be very different models of care.
- Will someone explain the process in plain language? They should. If a provider can't explain it clearly, keep asking.
When families hear “ICU in the sky,” it can sound dramatic. In practice, it means something reassuring. The patient isn't being moved away from care. Care is moving with them.
The Critical Care Expert at 30,000 Feet
A medevac flight nurse is best understood by function, not title. This clinician extends critical care into the transport environment. On the ground, an ICU nurse has a room full of support, wall oxygen, backup equipment, and nearby physicians. In flight, the nurse works in a compressed care space where every decision has to be deliberate.
That's why I often describe the role as an ICU commander in the sky. The nurse isn't replacing the hospital team. The nurse is carrying forward the treatment plan, adapting it to the aircraft, and responding in real time if the patient changes.
Transport is treatment, not just movement
One of the strongest historical markers for this role is the shift from simple evacuation to true airborne critical care. In a combat-setting air evacuation study, critical care-trained flight crews had a 48-hour mortality rate of 8% versus 15% for standard MEDEVAC crews, with an adjusted 66% lower estimated risk of death within 48 hours, according to this PubMed study on critical care air transport.
That matters because it shows a flight crew's clinical skill can affect survival, not just speed. Rapid assessment, airway support, medication management, and critical care transport capability can change outcomes.
Practical rule: If a patient's condition could worsen during travel, the right medical crew matters as much as the aircraft.
What makes this different from other nursing roles
A hospital nurse usually hands off a patient before the ambulance or aircraft leaves. A flight nurse takes responsibility during the interval when the patient is away from both hospitals. That gap is where hidden risk lives.
Here's a simple comparison:
| Role | Main setting | Primary focus |
|---|---|---|
| Hospital ICU nurse | ICU room | Ongoing bedside critical care with full hospital resources |
| Ground transport nurse | Ambulance | Critical care during road transfer |
| Medevac flight nurse | Aircraft cabin | Critical care under altitude, vibration, noise, and space constraints |
The aircraft environment changes everything. Noise affects communication. Space limits movement. The team has to think ahead because stopping to get more supplies isn't an option.
Questions people often ask
- Is the nurse allowed to make decisions in the air? In a critical care transport model, the nurse works with protocols, physician direction as needed, and advanced clinical judgment.
- Does the nurse only care for one patient? On a dedicated medical flight, the patient is the center of the mission.
- Is the nurse there mainly for reassurance? Reassurance is part of the job. Active medical management is the core of it.
Essential Certifications and Training
A calm voice is comforting. Competence is what keeps a transport safe.
When you're evaluating a provider, one of the most useful things to ask is not “Do you have nurses?” but “What kind of nurses are they?” A qualified medevac flight nurse typically brings 5+ years of recent critical care or emergency nursing experience and advanced certifications such as ACLS, PALS, and often CFRN, based on this flight nurse qualification overview.
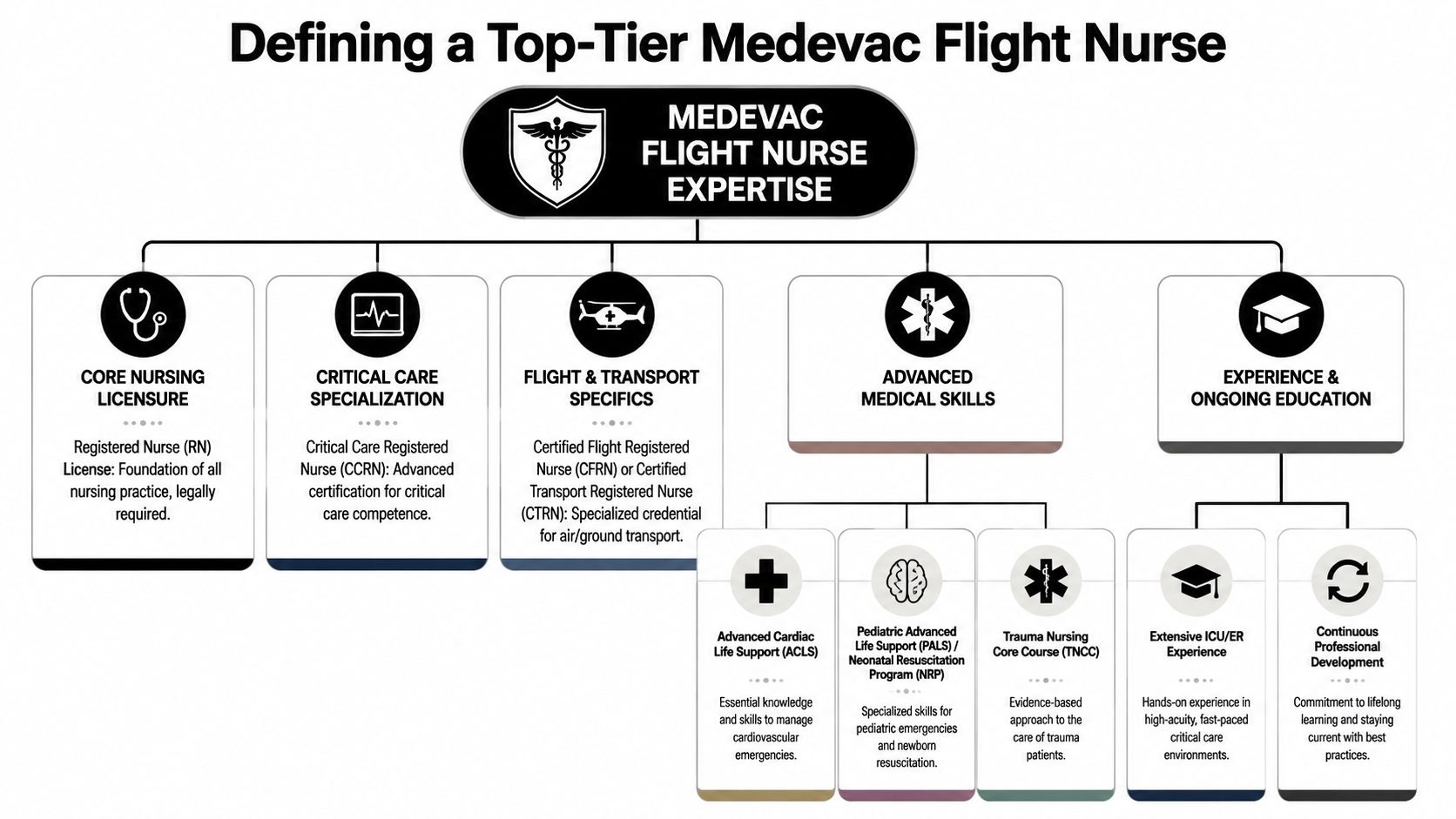
What those letters mean in plain English
Credentials can sound like alphabet soup. Here's the practical translation families and case managers can use.
- RN means the nurse is licensed as a Registered Nurse.
- ACLS means training in advanced cardiac life support. Think rhythm problems, cardiac emergencies, and medication-based resuscitation.
- PALS points to pediatric advanced life support.
- NRP applies to neonatal resuscitation in programs that move newborns.
- CFRN stands for Certified Flight Registered Nurse. That credential is a strong sign the nurse has specialty knowledge in flight physiology, transport pharmacology, airway management, and ventilator care.
Why experience matters so much
Not every excellent nurse is ready for flight medicine. A medevac flight nurse often has to think across ICU care, emergency response, prehospital logistics, and transport safety all at once.
That's why programs commonly look for deep high-acuity experience before independent flight duty. A nurse who has managed unstable patients for years is more likely to recognize subtle changes early, before they become emergencies in the cabin.
The safest transport teams usually sound the least dramatic. They prepare early, ask detailed questions, and don't guess.
Questions worth asking a provider
If you're a family member or discharge planner, these questions are fair and useful:
- How much recent ICU or ER experience does the nurse have?
- Does the crew include flight-specific certifications such as CFRN?
- What trauma, pediatric, or neonatal training do they carry if that applies to my patient?
- Do they routinely transport patients like this one?
- What physical or operational limits affect case acceptance?
If you want a better sense of how specialized transport teams build readiness, Med Jets by Air Trek offers a page on patient transport training that gives useful context on the preparation behind medical transport work.
A quick benchmark table
| What to ask about | Why it matters to you |
|---|---|
| Critical care background | Tells you whether the nurse is used to unstable patients |
| Flight-specific certification | Shows transport medicine knowledge beyond bedside nursing |
| Pediatric or neonatal training | Important if the patient isn't an adult |
| Trauma preparation | Relevant for multi-system injury and urgent transfers |
| Operational requirements | Helps explain why some patients need a specific aircraft or crew mix |
Managing Care from Takeoff to Touchdown
The in-flight phase is where people most underestimate the job. Families may imagine the nurse checking a monitor and documenting vital signs. In reality, the nurse is often adjusting oxygen strategy, evaluating circulation, troubleshooting lines, managing medications, and watching for problems that can develop because the patient is now in the air.
Guidance for flight nursing describes the role as that of an autonomous critical-care provider in an ICU-like micro-environment. Cabin altitude can reduce available oxygen pressure and worsen hypoxemia, so the nurse may adjust FiO₂, modify ventilator settings, and treat gas-expansion risks such as pneumothorax before ascent, according to this air medical flight nurse job description PDF.
What the nurse is doing before wheels up
A strong flight starts on the ground.
Before departure, the nurse reviews the chart, confirms the diagnosis, checks allergies, verifies medication infusions, examines the airway plan, and tests equipment. If a patient has a chest injury, recent surgery, a ventilator, or unstable blood pressure, the nurse thinks through what altitude and motion might do to that condition.
Common preflight tasks include:
- Airway review: Is the airway secure, and is there a backup plan if it isn't?
- Medication setup: Are critical drips organized, labeled, and ready for transport?
- Monitoring plan: Which trends matter most during flight?
- Risk prevention: Could trapped gas, swelling, agitation, or secretions become dangerous after ascent?
What changes in the air
The aircraft isn't a quiet room. It's noisy, tight, and physically demanding. Vibration can affect equipment performance. Space can make even simple tasks more difficult. The nurse has to anticipate instead of react late.
Here's what that can look like in plain language:
- Ventilator management: The nurse watches oxygenation and breathing mechanics, then adjusts settings if the patient's condition changes.
- Vasoactive infusion oversight: If blood pressure support is running, the nurse monitors the effect closely and corrects problems quickly.
- Line and pump checks: In flight, every tube and connection matters. A kinked line can become a serious issue fast.
- Neurologic reassessment: For stroke, brain injury, or altered mental status, even subtle changes are important.
For families traveling with pets at other times, some of the same principles apply on a much simpler level. Preparation, calming strategies, and minimizing stress before air travel matter a lot, which is why resources like this guide to stress-free dog flights can be helpful for non-medical trips too.
The equipment side families rarely see
Transport medicine depends on smart packing and reliable gear. A flight team may bring portable monitoring, suction, oxygen delivery tools, infusion systems, and airway equipment sized to the patient's needs. If you want a sense of the kind of gear that supports these missions, this page on aero medical supplies is a useful reference.
Good in-flight care is proactive. The nurse is trying to prevent the problem that hasn't happened yet.
That's the heart of the work. The best missions feel uneventful to the family because the nurse spent the whole flight keeping them that way.
What to Expect During a Medical Flight
From the patient's side, a medical flight usually feels less like “boarding a plane” and more like a carefully staged hospital transfer. Every handoff matters. Every detail should be repeated and confirmed.
At the sending bedside
The process begins with a bedside report. The flight team receives the hospital handoff, reviews current status, confirms medications and recent changes, and checks that the patient is ready to move.
For families, this is a good time to ask:
- Who is my main point of contact today?
- What equipment is staying with the patient during transfer?
- What will the patient likely feel during loading and flight?
If the patient takes multiple medications and the family is trying to keep prescriptions organized for the broader trip, a practical resource like this worry-free prescription travel guide can help with medication documentation and travel planning questions outside the aircraft itself.
During loading and the flight
Loading is controlled and methodical. The patient is secured, equipment is positioned for access, and the clinical team confirms that nothing important is blocked or disconnected. Seniors may need extra cushioning, hearing support, or slower movement. Bariatric patients may require specialized lift planning and cabin setup that protects dignity as well as safety.
Inside the aircraft, the environment is more clinical than commonly anticipated. There may be monitor alarms, headset communication, and ongoing reassessment. Some patients sleep through much of the transport. Others need coaching and reassurance the whole way.
A few things families should know:
| What you may notice | What it usually means |
|---|---|
| Frequent checks by the nurse | The nurse is watching trends, not waiting for a crisis |
| Adjustments to oxygen or equipment | Normal part of keeping the patient stable in flight |
| Limited conversation during busy moments | The crew is prioritizing patient care and cockpit communication |
On arrival
Arrival is another handoff, not the end of care. The flight nurse gives a detailed report to the receiving team, including what happened during transport, what medications were given, and what the patient looked like on arrival.
That continuity matters. A strong receiving report helps the next team act quickly without repeating work or missing changes that happened in transit.
A well-run medical flight should feel connected from bed to bed, not broken into separate pieces.
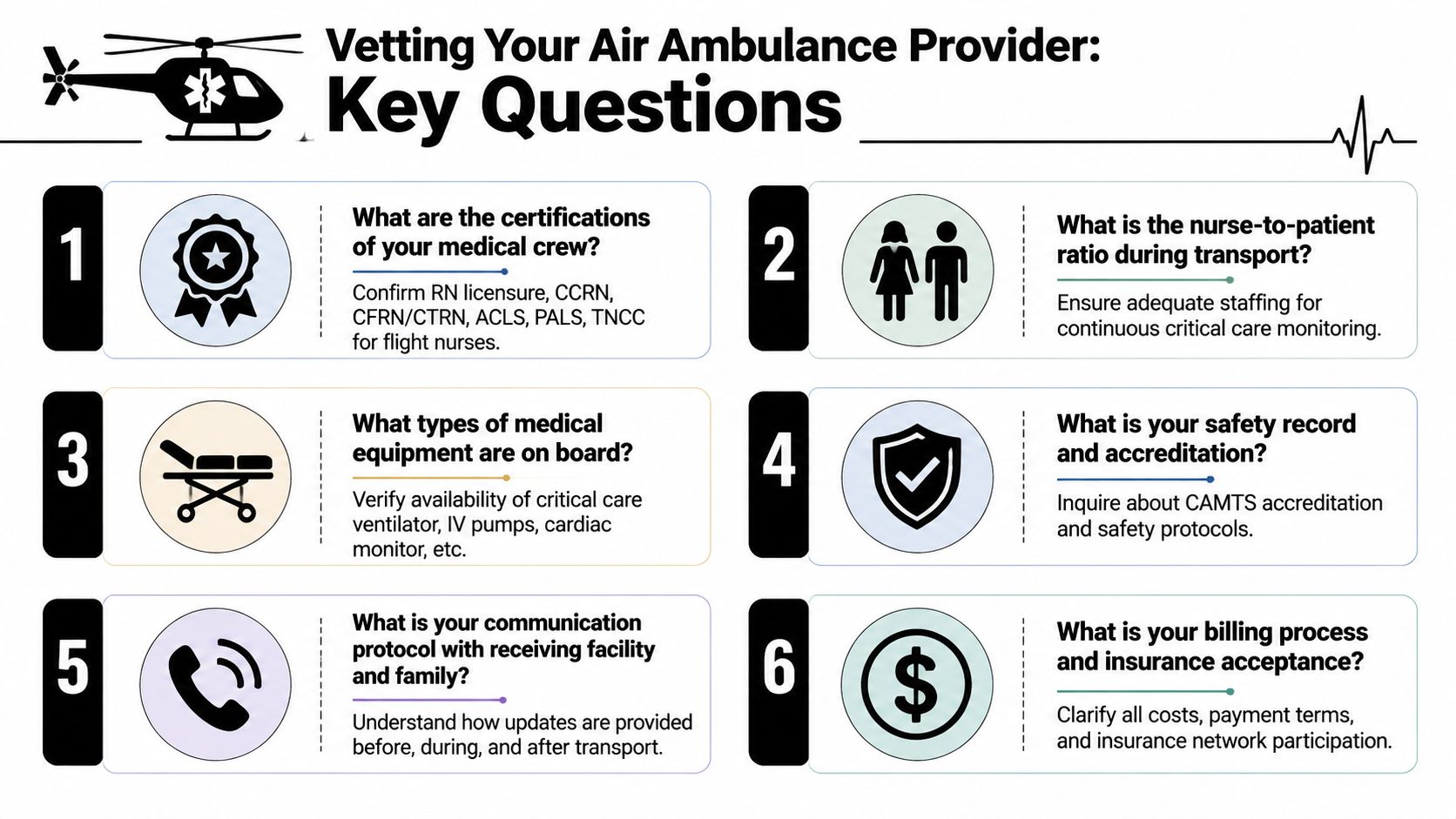
Questions to Ask Your Air Ambulance Provider
The most important decision often isn't whether to fly. It's what kind of flight service fits this patient's condition.
A dedicated air ambulance and a commercial medical escort are not interchangeable. Air medical services help bridge geographic access gaps, especially when local specialty care isn't available, but consumers often struggle to tell when a dedicated air ambulance is necessary versus when a commercial medical escort is enough, as discussed by Guardian Flight's consumer-facing air medical information.
Start with the care model
Ask this first: Is this a dedicated medical aircraft or a commercial escort?
A dedicated air ambulance is usually the better fit when the patient needs continuous clinical intervention, stretcher transport, oxygen management beyond simple support, ventilator care, complex medication infusions, or close coordination between facilities. A commercial medical escort may fit a stable traveler who can safely use a scheduled airline with professional nursing support.
The questions that reveal quality
Use this checklist when you call providers:
- Who exactly is on the crew? Ask whether the flight includes a registered nurse, paramedic, respiratory therapist, or another transport clinician depending on the case.
- What qualifications does the nurse have? Ask about recent ICU or ER experience and transport-specific credentials.
- Can you handle this diagnosis? Stroke, cardiac cases, bariatric transfers, pediatric needs, and ventilated patients all require different planning.
- How do you coordinate bed-to-bed logistics? You want to know who handles hospital communication, ground transport, records, and timing.
- How will you update the family? Clear communication reduces confusion when things move quickly.
- What are the payment terms? You should understand costs, timing, and financial paperwork before launch whenever possible. A practical starting point is reviewing medical flight payment terms and conditions.
A short video can also help families understand what to listen for when evaluating providers.
Dedicated air ambulance versus commercial escort
| If the patient needs | Usually points toward |
|---|---|
| Stretcher transport and onboard equipment | Dedicated air ambulance |
| ICU-level monitoring or intervention | Dedicated air ambulance |
| Stable travel with nursing oversight on a scheduled flight | Commercial medical escort |
| Complex bariatric or fragile transfer logistics | Often dedicated air ambulance |
The right provider won't rush past these distinctions. They'll ask careful questions, explain their reasoning, and tell you if a different transport model is safer.
Your Medevac Flight Nurse Questions Answered
Can a family member travel with the patient?
Sometimes yes, sometimes no. It depends on the aircraft, the patient's condition, space, weight-and-balance limits, and safety requirements. Ask early, because this affects planning.
Will the nurse talk to the sending and receiving hospitals?
Yes, that's a routine part of high-quality transport. The nurse helps maintain continuity by receiving a detailed handoff before departure and giving one again on arrival.
What if the patient gets worse in the air?
That's one of the core reasons a medevac flight nurse is on board. The nurse is there to recognize deterioration early and intervene during transport, not just after landing.
Is a medical escort the same as a medevac flight nurse on a private jet?
No. A commercial medical escort and a dedicated air ambulance serve different patient needs. If the patient may need active in-flight treatment or can't travel as a regular airline passenger, ask specifically whether a dedicated medical aircraft is the safer fit.
Can the nurse manage oxygen, monitors, and medications during flight?
Yes. That's central to the role in a critical care transport model.
What should I listen for when choosing a provider?
Listen for clarity. A trustworthy team should explain who the crew is, what care they can provide in the air, how they handle handoffs, and why they're recommending one transport option over another. If the answers are vague, keep asking until they aren't.
If you're comparing transport options for a loved one, ask the provider to walk you through the mission exactly as it will happen, from bedside pickup to receiving-facility handoff. The more clearly they can explain the nurse's role, the more confident you can feel in the care plan.