When the phone rings and a doctor says your family member needs urgent transport, you may hear only fragments. A trauma center. A higher level of care. A helicopter may be involved. You’re trying to absorb medical terms while also figuring out where your loved one is going, how fast the team can move, and what you’re supposed to do next.
That’s where clarity matters.
For families in Ohio, medflight of ohio is often part of that urgent path. It has been part of the state’s critical care transport system since 1995, and over time it grew into a self-sustaining nonprofit with helicopter and ground critical care options across the region, according to MedFlight’s history. In practice, that means hospitals, EMS crews, and emergency physicians already know how to activate it when time-sensitive transport is needed.
The hard part for families is that this usually happens in the middle of fear, not planning. You may be asking whether a helicopter is really necessary, whether ground transport would be safer or cheaper, whether your loved one is stable enough to move, or whether a different type of air ambulance makes more sense for a longer trip.
Those are the right questions.
This guide is written the way I’d explain it to a family member or hospital case manager at bedside. Plainly. Calmly. Without assuming you work in transport medicine every day. If you’re also trying to understand why transport timing matters so much in emergency medicine, this overview of the medical golden hour gives helpful context.
Answering the Call in a Crisis
A common scenario looks like this. A patient is at a smaller hospital after a stroke, serious trauma, cardiac event, or another condition that needs services the current facility can’t provide quickly enough. The bedside team starts arranging transfer. The family hears “MedFlight” and assumes that only means a helicopter. It doesn’t.
What matters first is the level of care needed during transport. The transport team and sending clinicians are deciding two things at once:
- How fast the patient needs to move
- What kind of medical support must happen during that move
If the patient needs rapid access to a Level 1 or Level 2 trauma center from an accident scene, a helicopter may be the right answer. If the patient is critically ill but the route, weather, distance, or landing logistics make ground more practical, a critical care ground unit may be the better choice. The decision is clinical first, logistical second.
Practical rule: The best transport mode isn’t the most dramatic one. It’s the one that gets the patient to the right facility with the right medical team and the fewest avoidable delays.
That distinction matters because families often feel pressure to “approve” something instantly. In reality, emergency field transports are usually driven by first responders and medical protocols. Interfacility transfers involve more coordination, but the same principle applies. The transport method should match the patient’s condition, destination, and operational reality on that day.
MedFlight’s role in Ohio is important because it sits inside that emergency transfer system rather than outside it. When people say “they’re calling MedFlight,” they usually mean the local clinical team has determined that a critical care transport resource is needed, not merely that a helicopter sounds faster.
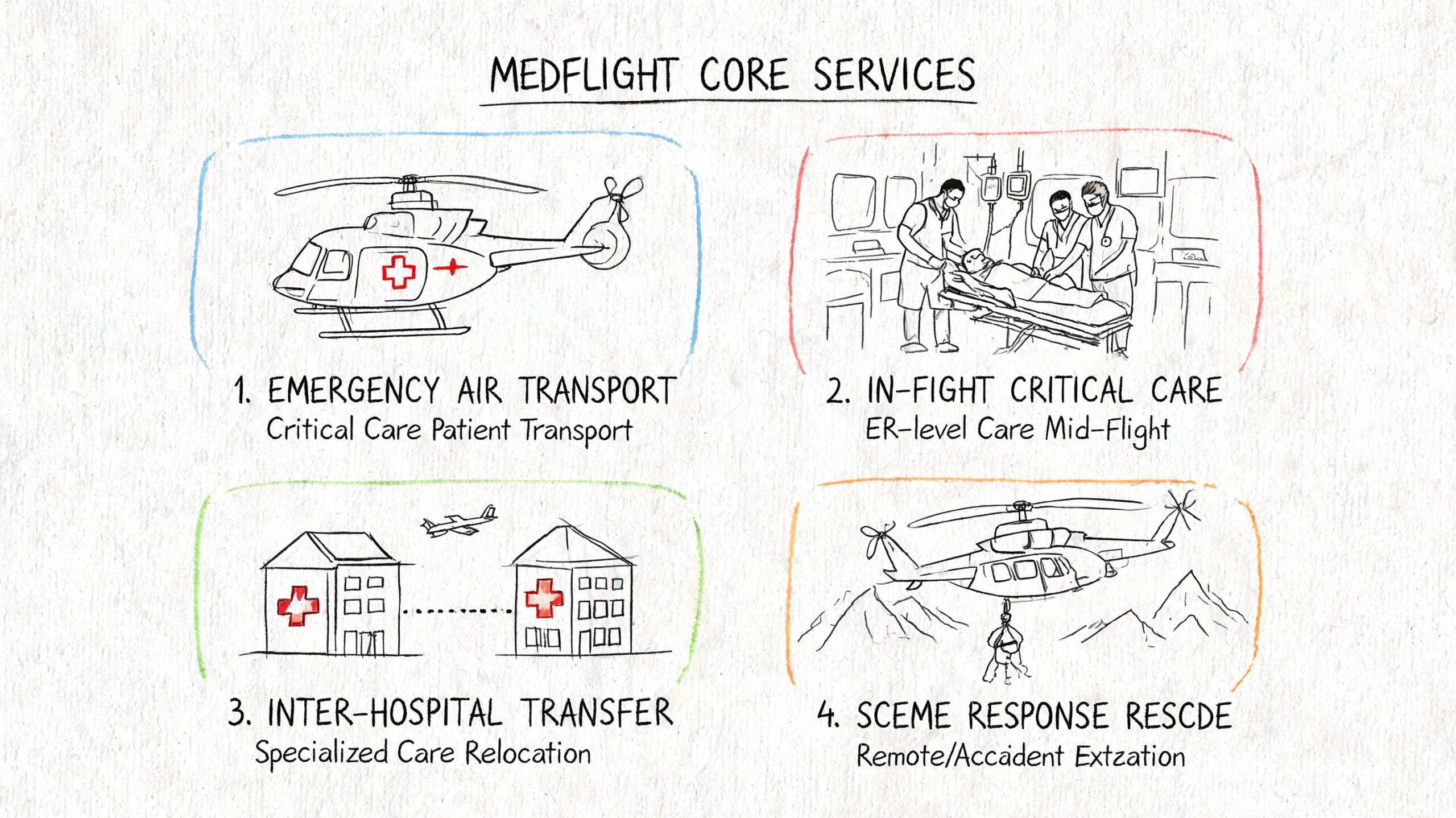
Understanding MedFlight's Core Services
MedFlight works like a critical care transport toolkit. It doesn’t rely on one vehicle for every problem. It uses helicopters for some missions and Mobile Intensive Care Units for others.
When the helicopter is the right tool
MedFlight of Ohio operates a standardized fleet of ten EC-130 helicopters through Metro Aviation, serving approximately 66 of Ohio’s 88 counties, according to MedFlight’s locations page. The EC-130 is used because it fits rapid medical response well, and using the same aircraft type across the fleet supports more consistent maintenance, pilot training, and patient care setup.
For families, that standardization matters more than it may seem. A standardized fleet usually means crews work in a more familiar cabin layout with predictable equipment placement and workflows. In high-acuity transport, consistency helps.
A helicopter is often chosen when:
- Scene response is urgent: The patient is being picked up from an accident scene or another setting where speed to a trauma center matters.
- Geography is working against time: Rural distance, traffic, or road access would slow a ground team too much.
- The receiving hospital has capabilities the current location lacks: Trauma, cardiovascular, pediatric, or other advanced services may be needed quickly.
If you want a simple explanation of how helicopters compare with airplane-based air ambulances, this guide to fixed-wing vs rotary-wing medical transport is useful.
When the MICU makes more sense
MedFlight also operates Mobile Intensive Care Units, commonly called MICUs. These are not standard ambulances. They are critical care ground units used for patients who need a high clinical level during transfer but may not benefit from rotor transport.
A MICU is often the better fit when:
- Weather limits safe helicopter operations
- The transfer is inter-hospital and ground time is acceptable
- The patient’s condition needs intensive in-transit monitoring, but not necessarily air transport
- Landing zone logistics would add delay rather than reduce it
What works and what doesn’t
Here’s the trade-off families should understand.
| Situation | Usually the better fit | Why |
|---|---|---|
| Serious trauma from a scene | Helicopter | Faster access to trauma care when distance and time matter |
| Critical interfacility transfer within a manageable driving radius | MICU | High-level care without air-specific constraints |
| Poor flying conditions | MICU or delayed air decision | Safety governs transport mode |
| Very long state-to-state transport | Often a fixed-wing alternative | Helicopters are not the usual answer for long-distance transfer |
What doesn’t work is assuming “air” always means “best.” In transport medicine, appropriate beats dramatic every time.
MedFlight Coverage Area and Partner Hospitals
A family in a small Ohio hospital may hear two things at once: the patient needs a higher level of care, and transport has to happen fast. At that point, coverage area is not a marketing detail. It decides whether MedFlight is a practical option now, whether a MICU will do the job safely, or whether the case needs a different transport plan.
How the base network supports response
MedFlight operates from Columbus and places aircraft and critical care resources around the state so crews can reach both major metro areas and communities where specialty care is farther away. Public information from the program shows helicopter bases in multiple Ohio regions, with headquarters at the Ohio State University Airport and ground critical care units based in Columbus and Chillicothe.
For case managers, the practical point is simple. Base placement affects response time, aircraft availability, and how often a patient can be moved directly to the accepting facility instead of waiting for a more distant crew.
That matters most in central and southern Ohio, where referral patterns often pull patients toward larger trauma, cardiac, stroke, pediatric, or tertiary centers.
What partner hospitals mean for families
Families often ask whether MedFlight only serves one hospital system. In practice, transport decisions are driven by the patient’s diagnosis, the accepting physician, and the level of care available at the receiving hospital.
MedFlight is tied into referral relationships with major Ohio providers, including OhioHealth and Nationwide Children’s Hospital. For a family, that usually means the crew is entering a system where handoff expectations, communication channels, and specialty receiving pathways are already familiar to the teams involved. That does not guarantee a specific destination. It does improve coordination when the patient needs trauma care, pediatric specialty support, or another service that the local hospital cannot provide.
I tell families to focus on one question: Is the receiving hospital the right clinical fit? The aircraft name matters less than whether the destination can treat the problem.
Coverage does not guarantee dispatch
A wide service area still has limits. MedFlight may cover a region and still decline or defer a flight if another mode is safer or faster for that patient.
Common reasons include:
- Weather or visibility that does not support safe flight
- A landing zone problem at the sending location
- The patient’s condition being better suited to critical care ground transport
- Aircraft already committed to a higher-acuity mission
- Delay in confirming the receiving facility and accepting team
This is the part families and discharge planners need to hear clearly. “Within the coverage area” does not mean “automatic helicopter.”
For regional Ohio transfers, MedFlight is often a strong fit when the destination is within its normal operating pattern and rapid access to specialty care will change the patient’s outcome. For longer interstate moves, the decision can shift. If the patient is going several states away, a fixed-wing jet service may be more practical because it handles distance more efficiently and usually avoids the operational limits that make helicopter transport less useful on long routes.
How to Arrange a MedFlight Transport
Families rarely make the transport call themselves. In most cases, the process starts with a physician, hospital transfer center, EMS agency, or first responder. That’s appropriate. The request has to include clinical information, destination planning, and operational details that the transport team needs to evaluate.
What usually happens first
The sequence is typically straightforward:
- The sending team identifies the need for higher-level care.
- A transport request is placed through the appropriate communication pathway.
- Clinical and logistical details are reviewed.
- The transport mode is chosen.
- The crew moves the patient and hands off to the receiving facility.
For the family, the most important thing is to know who your point person is. In the emergency department, that may be the attending physician or bedside nurse. In an inpatient transfer, it may be the case manager, house supervisor, or transfer center staff.
What information the transport team needs
Even when families don’t place the request, they can help by staying organized.
The sending team usually needs to confirm:
- Patient identity and current location
- Current diagnosis or working emergency concern
- Receiving hospital acceptance
- Weight, mobility, and any special handling issues if relevant
- Current stability and major interventions in progress
- Family contact information
If you’re the case manager, delays often come from missing acceptance details, incomplete records, or uncertainty about who is covering the patient on arrival. If you’re family, your role is smaller but still important. Make sure the team has the correct contact number for updates and knows who the primary family spokesperson is.
What happens during the transport
The crew’s focus is patient care, not family communication in real time. Once the patient is loaded, the clinical team manages monitoring, medications, airway support if needed, and a direct handoff at the receiving hospital.
The smoothest transfers happen when the sending team has already clarified the destination physician, sent key records, and prepared the family for the fact that transport crews may move quickly and speak in brief, direct terms.
At arrival, the transport team gives report to the receiving clinicians. That handoff matters as much as the flight or drive itself. Good transport isn’t just movement. It’s continuity.
Verifying Safety Credentials and Medical Expertise
When a family hears “helicopter transport,” one concern is immediate and reasonable. Is this safe? The right way to answer that question is to look at accreditation, crew structure, aviation oversight, and operational experience.
What CAMTS accreditation means in practice
MedFlight of Ohio is CAMTS-accredited, completed 3,709 helicopter transports in the fiscal year ending June 30, 2024, and operates 10 helicopters through Metro Aviation, with nurse-paramedic crews supervised by medical control physicians, according to Metro Aviation’s MedFlight profile.
For a family, the term CAMTS matters because it signals that the service is measured against recognized transport standards. Accreditation does not mean zero risk. Nothing in emergency transport can promise that. What it does mean is that the organization is expected to maintain structured practices around safety, clinical care, training, and operations.
Why the crew model matters
A helicopter is only a platform. The key question is who is taking care of the patient inside it.
MedFlight’s public description identifies nurse-paramedic crews operating under physician supervision. That combination is a familiar and credible critical care transport model. It matters because transport medicine sits in an awkward space between emergency care and ICU care. Crews need to stabilize, monitor, anticipate deterioration, and communicate effectively with both sending and receiving teams.
For families, here’s the simplest way to understand it:
- Pilot function: Safe aircraft operation
- Medical crew function: Ongoing critical care
- Physician oversight: Protocols, medical control, and clinical governance
What high volume does and doesn’t tell you
A transport program handling 3,709 helicopter transports in a single fiscal year has meaningful operational experience. That volume suggests a system that is active, practiced, and fully integrated into emergency care.
At the same time, don’t use volume as the only test. Ask a more useful question: Is this crew trained and equipped for my patient’s condition? For trauma, cardiovascular, and pediatric cases, MedFlight’s published clinical structure supports confidence. For highly specialized needs outside typical rotary or regional critical care transport patterns, a different service model may still be more appropriate.
Safety isn’t just about the aircraft. It’s about accreditation, crew discipline, dispatch judgment, and whether the mission matches the tool.
Navigating Costs Membership and Insurance
At 2 a.m., families rarely ask first about rotor speed or accreditation. They ask who will pay, what insurance covers, and whether this transport will leave a bill they cannot handle. With medflight of ohio, those are reasonable questions, and they should be asked early if the patient’s condition allows it.
What is known and what is still unclear
MedFlight is a not-for-profit, CAMTS-accredited organization, but public information on out-of-pocket costs for uninsured patients, financial assistance programs, and typical billing timelines isn’t readily available, according to its community outreach information.
For a family or case manager, that means one thing. Do not assume the billing side will be simple just because the service is nonprofit. Nonprofit status does not automatically tell you what the patient will owe, how quickly statements will arrive, or whether hardship review is available.
If you need a broader primer before speaking with billing staff, this guide to medical flight costs gives useful background on how air medical charges are usually structured.
Questions to ask before transport or as soon as the patient is stable
In bedside coordination, the best financial decisions usually come from a short, written checklist. A five-minute conversation now can prevent days of confusion later.
Ask:
- Who submits the claim? Confirm whether MedFlight bills the patient’s insurance directly.
- What information is needed right away? Ask whether the family or sending hospital must provide insurance cards, policy numbers, or authorization details.
- What could remain after insurance pays? Get a plain answer on possible patient responsibility.
- What happens if the patient is uninsured? Ask for the correct billing or financial counseling contact on the first call.
- Are payment plans or hardship options available? If they exist, ask how to apply and what documents are required.
- When should the first statement arrive? Families often expect an immediate bill, but the actual timeline can vary.
Case managers sometimes compare more than medical capability. They also review the insurance and compliance framework behind transport operations, especially when they are weighing several vendors. A plain-language overview of commercial vehicle insurance requirements can help non-transport professionals understand why liability and regulatory questions still matter around medical transport services.
About membership questions
Regarding membership, people often ask whether MedFlight offers a program that reduces or eliminates out-of-pocket costs after insurance. The verified public information provided here does not document membership terms, benefits, or exclusions.
That puts the burden on verification. Families and discharge planners should not assume a membership exists, applies to this trip, or replaces insurance review unless MedFlight confirms the details directly through its billing team and, ideally, in writing.
This is also where decision-making matters. If the transfer is regional and medically urgent, MedFlight may still be the right tool even if billing details are incomplete at the bedside. If the patient is traveling a much longer distance and the case manager is comparing rotary transport with a fixed-wing option, cost structure and insurance handling may look very different. In those situations, ask both providers the same questions and compare the answers line by line.
Patient Logistics and Family Considerations
The medical team may be focused on blood pressure, airway status, or receiving-bed availability. Families are often focused on a different set of questions. Can I go with them? Where do their belongings go? Who calls me when they land?
Those questions are not secondary. They affect whether the transfer feels manageable.
What families should expect
In a helicopter, space is limited and the medical crew needs room to work. That means a family member often won’t be able to ride with the patient. If the transport is by ground critical care unit, accompaniment policies can differ, but you should still ask rather than assume.
Belongings usually need a plan before departure. In bedside coordination, the least chaotic approach is this:
- Phone and wallet: Confirm whether they stay with the patient or with family
- Medication list and identification: Make sure the sending team has accurate information
- Clothing and personal items: Expect that these may travel separately from the patient
- Hearing aids, glasses, dentures: Ask specifically so they’re not left behind
Communication during the move
Families often expect updates from the aircraft or ambulance itself. Sometimes that happens, but often the cleaner update comes from the sending or receiving hospital once the patient arrives.
If you’re the family spokesperson, give one cell number to the hospital team and ask exactly who will call you after arrival. One clear contact path avoids missed updates and repeated calls to the wrong department.
For families who later need help sorting statements or understanding coding workflows in Ohio, resources that explain the basics of medical billing in Springfield Ohio can make the paperwork side less intimidating.
The best practical mindset is this: the crew’s first job is moving the patient safely. The family’s job is to stay reachable, keep records, and head to the receiving facility only after confirming where the patient is being admitted.
Common Questions and When to Consider Alternatives
Some questions come up in almost every transport conversation, and the answers can save time.
Common questions families ask
Is MedFlight the same as a regular ambulance?
No. A regular 911 ambulance handles many emergency responses and routine transports. MedFlight is a critical care transport resource used when the patient needs a higher level of transport capability.
Can we request a helicopter because it seems faster?
Usually not in the way people imagine. In emergency scenes, first responders and medical protocols drive that decision. In hospital transfers, the sending team and transport service decide based on clinical and operational factors.
Does a helicopter always beat ground?
No. Weather, landing logistics, loading time, patient condition, and route length all affect the actual answer.
When MedFlight is usually the right choice
MedFlight is often the right fit when the need is regional, urgent, and clinically complex. That includes scene trauma, time-sensitive transfers to higher-level Ohio facilities, and hospital-to-hospital moves where critical care support must continue during transport.
It’s especially strong when the patient is staying within the service pattern MedFlight was built to support. In those situations, local integration matters. Dispatch familiarity, hospital relationships, and established handoff routines can make a real difference.
When to consider alternatives
There are times when another transport model may fit better.
Consider alternatives when:
- The transfer is long-distance or state-to-state. A fixed-wing jet service is often more practical than a helicopter for that mission profile.
- The move is planned rather than emergent. Repatriation or scheduled medical relocation follows a different workflow than emergency dispatch.
- The patient has special transport needs. Bariatric configuration, extended family accompaniment, or unique cabin requirements may call for a different aircraft type.
- The receiving destination is far outside MedFlight’s normal operational pattern. Regional helicopter systems are not designed for every long-range mission.
The key decision framework is simple. Ask three questions:
- How urgent is the move?
- What level of care is needed during transport?
- What vehicle type matches the distance and logistics?
If the answer points to rapid regional critical care, medflight of ohio is often the natural solution. If the answer points to long-range medical aviation, a fixed-wing provider may be the better path.
If you’re trying to arrange a longer-distance transfer, a bariatric medical flight, or a hospital-to-hospital move beyond Ohio’s regional helicopter pattern, Med Jets by Air Trek can help evaluate options and coordinate the right level of transport. You can learn more through Med Jets by Air Trek.