
At many hospitals, the problem starts before anyone calls it a disaster. The emergency department fills fast. ICU beds tighten. A patient needs a higher level of care that your facility can't provide on site, and the transfer window is narrow. In that moment, the worst time to discuss transport terms, credentialing, liability, or reimbursement is right then.
That's why mutual aid agreements matter in healthcare. They turn professional goodwill into an operating system. Instead of relying on favors, assumptions, or a chain of improvised phone calls, they define who can request help, what kind of help can be sent, how staff and equipment are cleared, and how costs are handled.
For hospitals, that can mean the difference between delay and continuity of care. It also matters far beyond public agencies. Healthcare mutual aid often depends on public-private coordination, including hospitals, specialty transport providers, labs, vendors, and regional response partners.
Why Pre-Planning Is Critical in a Crisis
A regional hospital can absorb routine surges. It struggles when several pressures hit at once.
A highway pileup sends multiple trauma patients to the emergency department. At the same time, a cardiac patient needs urgent transfer to a specialty center far away. Staff are working at capacity. Bed management is stretched. Clinical leaders are making triage decisions in real time. If transport arrangements still need to be negotiated, the hospital has already lost valuable time.
What fails when nothing is written down
In healthcare, delays rarely come from a lack of effort. They come from unanswered operational questions.
- Who can activate help: If only one administrator is authorized to approve outside support and that person is unavailable, the request stalls.
- What resources are included: A hospital may assume an outside partner can provide a clinical crew, specialty equipment, or bariatric capability. The partner may assume the opposite.
- How information moves: Patient transfer breaks down if clinical handoff protocols, contact points, and documentation requirements aren't already agreed.
- Who pays: Finance uncertainty can freeze decision-making, especially when private providers or cross-jurisdictional partners are involved.
Practical rule: If your team needs to negotiate terms during an incident, you don't have a response framework. You have a hope-based plan.
Pre-planning fixes that. A strong agreement establishes authority, workflow, and escalation paths before the first urgent call. It also creates a shared understanding between hospital leaders, emergency managers, legal counsel, transport coordinators, and outside partners.
Why hospitals need this even for non-disaster events
Healthcare leaders sometimes hear “mutual aid” and think hurricanes, mass casualty events, or regional emergencies. Those are obvious use cases, but the daily value is broader. Transfers, temporary capability gaps, staffing strain, and specialized transport needs all benefit from prearranged support relationships.
Hospitals that map these contingencies ahead of time usually coordinate faster because they've already answered the practical questions. A useful reference point is this overview of emergency medical response coordination, which shows how quickly medical transport decisions become operational, not theoretical.
Mutual aid agreements don't eliminate pressure. They remove avoidable friction.
Understanding Mutual Aid Agreements
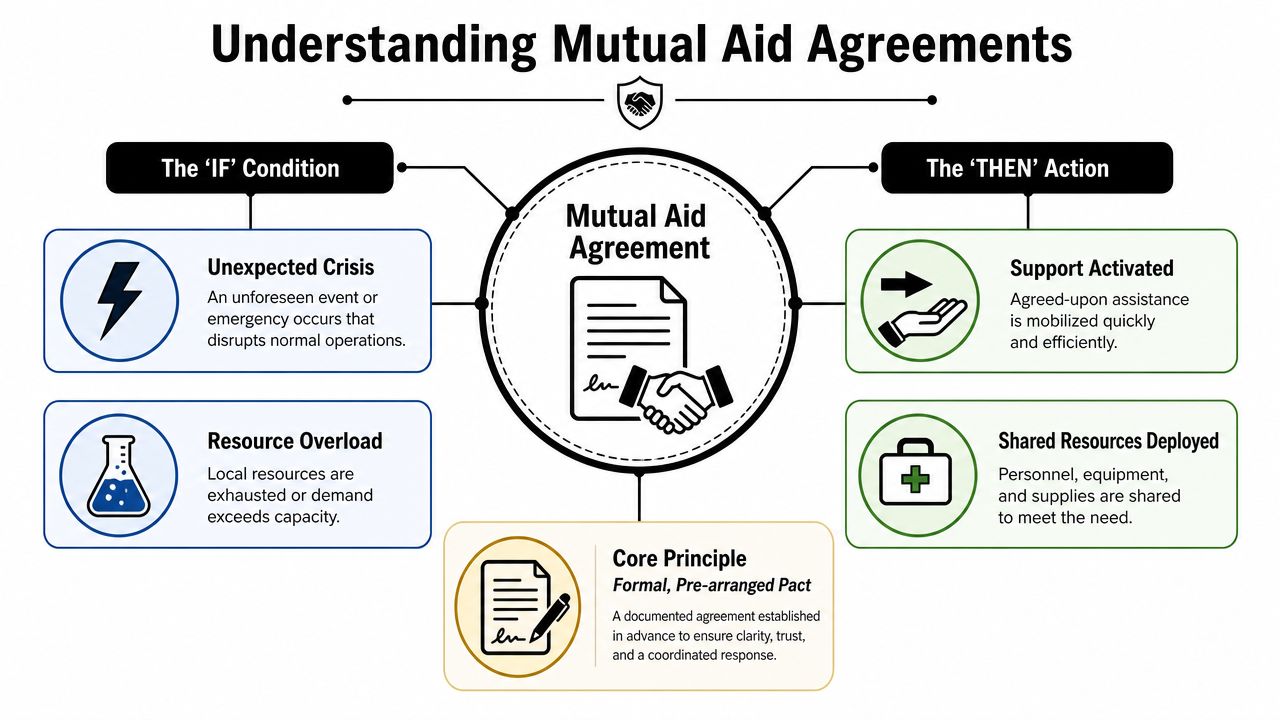
A mutual aid agreement is best understood as a formal if-then pact.
If a hospital, public agency, or healthcare partner faces a situation that exceeds its immediate capability, then another defined partner can provide specified support under terms that were settled in advance. That support might include personnel, equipment, supplies, information-sharing, transport coordination, or patient movement.
The difference between courtesy and capability
Hospitals often have informal partner relationships. Those relationships matter, but they aren't enough when conditions are strained.
An informal arrangement usually depends on memory, goodwill, and whoever answers the phone first. A mutual aid agreement turns that into a repeatable system. It states what triggers assistance, who has authority to request it, what obligations each side has, and what legal and operational rules apply once support begins.
That matters in healthcare because patient movement isn't just logistics. It involves protected information, clinical responsibility, transport risk, receiving-facility coordination, and documentation. Vague cooperation language won't carry that load.
Why the concept became a nationwide standard
A major U.S. milestone came after Hurricane Andrew in 1992, when the Emergency Management Assistance Compact (EMAC) was created. Congress approved it, and by the time of the CDC review it had been enacted in all 50 states, the District of Columbia, Puerto Rico, and the U.S. Virgin Islands, creating a standardized framework across 54 U.S. jurisdictions for sharing resources during disasters, according to the CDC's review of EMAC and mutual aid practice in Public Health Reports.
That history matters because it shows mutual aid isn't a niche legal concept. It became a broad, standardized mechanism for moving personnel, equipment, and other resources across boundaries when local capability wasn't enough.
In practice, the biggest value of mutual aid is predictability. People know what they can ask for, what they're expected to send, and what happens next.
For healthcare facilities, that same logic applies at a smaller operational scale. You may not be invoking interstate disaster support, but you are solving the same basic problem. One organization can't always meet demand alone. A formal, prearranged framework makes outside help usable under pressure.
Key Types of Agreements for Healthcare Providers
Not every healthcare mutual aid agreement should look the same. The right structure depends on the gap you're trying to solve.
A community hospital that needs reciprocal support from nearby peers has one set of priorities. A hospital working with a state agency during public health emergencies has another. A facility that depends on a private air ambulance provider for high-acuity transfers needs a different model again.
Horizontal agreements between peer providers
These are agreements between organizations operating at roughly the same level. In healthcare, that often means hospital-to-hospital or hospital-to-health system coordination.
They work best when partners may need to share:
- Beds and patient placement: Diversion support, specialty unit capacity, or overflow coordination
- Clinical resources: Pharmacy support, specialty staff, equipment, or temporary service backup
- Operational support: Lab capacity, supply sharing, or coordinated incident communications
Horizontal agreements succeed when both parties are realistic about limits. Peer hospitals can help each other, but they often face the same regional stressors. If the agreement assumes unlimited support during a shared crisis, it will disappoint everyone involved.
Vertical agreements with public agencies
These agreements connect a facility to a broader government or emergency management structure. In practical terms, they matter when a hospital's needs intersect with county, regional, or state authority.
This model is useful for public health response, emergency declarations, coordination with emergency management, and access to wider resource systems. The strength of a vertical agreement is reach. The weakness is that activation can be more formal, and hospitals need to understand how requests move through the chain.
Public-private agreements for specialized capability
Many healthcare leaders need sharper planning.
Hospitals regularly depend on private entities for capabilities they don't maintain internally. That can include air ambulance transport, medical escorts, specialty vehicles, vendor-managed equipment, or niche clinical services. These aren't side arrangements. In many transfers, they are core components of patient care continuity.
A public-private agreement is especially valuable when the provider brings something the hospital can't improvise, such as long-distance critical care transport, bariatric transport capability, aircraft configuration for specific patient needs, or coordinated bedside-to-bedside movement.
The most durable healthcare mutual aid networks mix public coordination with private execution.
A useful test is simple. Ask what happens if your first-choice specialty partner is needed tonight, not next quarter. If activation, clinical handoff, dispatch contacts, credential review, and payment terms are still unsettled, the relationship is not operational yet.
Essential Clauses Every Agreement Must Include
The fastest way to weaken a mutual aid agreement is to keep it high level. In healthcare, broad language sounds cooperative but performs poorly when a transfer request becomes urgent.
FEMA-aligned guidance says effective agreements should predefine request procedures, payment and reimbursement rules, interoperable communications, liability and immunity treatment, recognition of qualifications, and relationships with other agreements, so responders can deploy without negotiating terms during the incident, as outlined in the Federal Highway Administration's evacuation and agreements guidance.
What belongs in the document
Start with authority. The agreement should identify who can request assistance, who can approve deployment, and what circumstances justify activation. Hospitals often stumble here because internal authority is less clear than people think, especially after hours.
Then define scope. Spell out whether the agreement covers staff, patient transport, equipment, pharmaceuticals, communications support, specialty teams, or information-sharing. If air medical transport or other private specialty services are part of the relationship, state that directly.
Mutual Aid Agreement Clause Checklist
| Clause Category | Key Item to Define | Why It's Critical |
|---|---|---|
| Activation authority | Which roles may request and approve aid | Prevents delay and confusion during nights, weekends, and incident escalation |
| Trigger conditions | What level of need activates the agreement | Stops disputes over whether the event qualifies |
| Resource scope | Which staff, equipment, transport assets, or services can be shared | Keeps assumptions from derailing response |
| Communications | Contact methods, escalation paths, and handoff protocols | Supports clean coordination across dispatch, clinical, and administrative teams |
| Credentialing | How licenses, qualifications, and privileges are recognized | Reduces delay for incoming personnel and specialty partners |
| Liability | Responsibility for acts, omissions, and equipment use | Protects both sides from avoidable legal ambiguity |
| Reimbursement | Billable costs, timing, documentation, and exclusions | Prevents finance disputes from slowing decisions |
| Records and documentation | Required forms, patient information flow, and post-incident reporting | Preserves compliance and continuity of care |
| Demobilization | How aid ends and resources return to normal service | Avoids open-ended obligations |
| Relationship to other agreements | Which contract controls if terms overlap | Prevents conflict between procurement, transport, and emergency agreements |
Clauses that often get overlooked
Some of the most important terms are easy to miss because they sound administrative rather than clinical.
- Retention of needed resources: A responding organization should be able to keep resources necessary for its own reasonable protection. Otherwise, a partner may hesitate to commit support.
- Verbal activation with written follow-up: In a real incident, waiting for signatures can slow response. Many workable models allow a verbal request first and written confirmation as soon as practical.
- Exercises and drills: If the agreement only exists for real emergencies, teams won't know whether the process works until it's put to the test in a real incident.
Hospital teams that need a drafting starting point often review Standard agreement forms before routing a document to legal counsel. Templates don't replace operational design, but they do help teams avoid missing core provisions.
A good agreement doesn't try to sound comprehensive. It tries to be executable at 2 a.m.
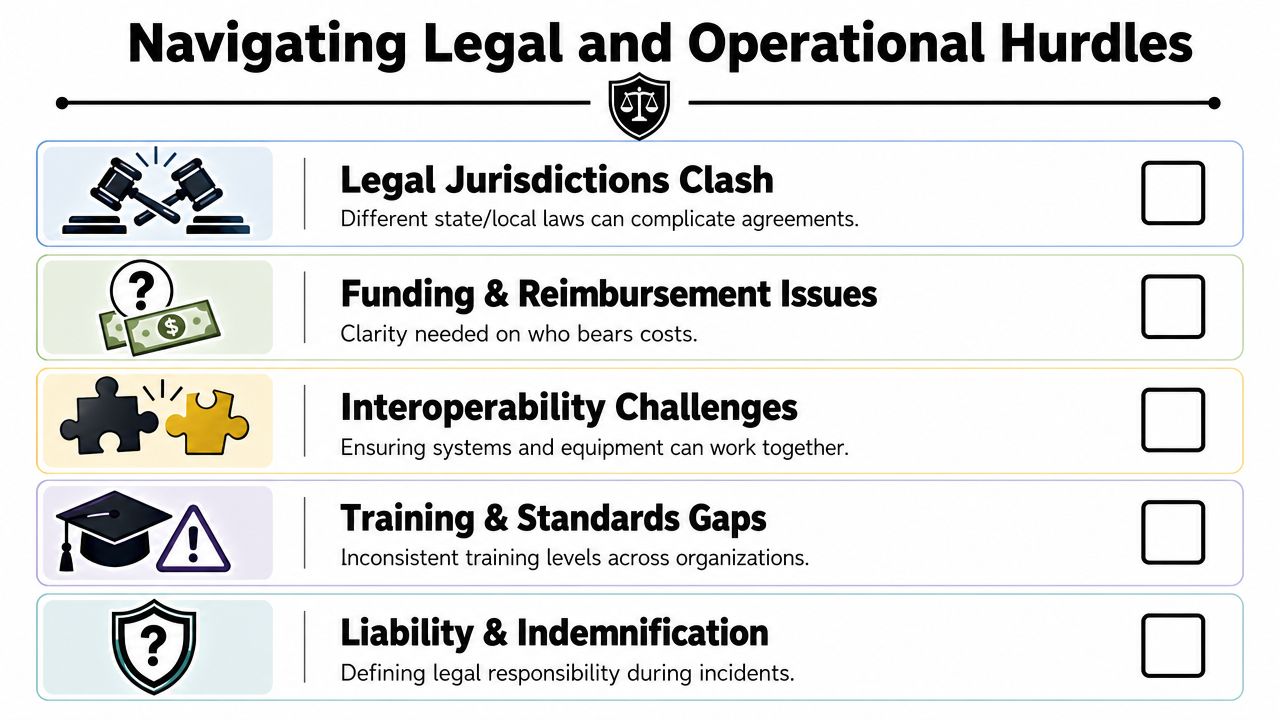
Navigating Legal and Operational Hurdles
A signed agreement can still fail on first use. In healthcare, the breakdown usually happens in three places: credentialing, liability, and reimbursement.
Each one affects whether a partner can respond quickly and whether they're willing to respond at all.
Credentialing and cross-jurisdiction practice
Healthcare leaders often assume clinical qualifications are the hard part. They aren't. The hard part is deciding how those qualifications will be recognized by the receiving organization under stress.
If a hospital works with outside clinical teams, transport crews, or specialty contractors, the agreement should state how credentials are reviewed, accepted, and documented. Without that, operations staff end up improvising a solution while the patient is waiting.
The same problem appears with communications and equipment. Even when two organizations both have capable teams, they may use different workflows, documentation expectations, or dispatch practices. Interoperability isn't just radios. It's whether people can work together without creating new risk.
Liability and financial friction
Liability terms deserve plain language. Who is responsible for deployed personnel? What happens if equipment is damaged? How are workers' compensation questions handled? These aren't side issues. They shape whether counsel approves the agreement and whether a partner sees the arrangement as workable.
Reimbursement terms are even more practical. Tennessee's framework shows how specific these provisions can be. Under that model, a responding party is entitled to 50% of reimbursable costs for the first six hours of assistance and 100% after six hours, while invoices must be submitted within 60 days after assistance ends, according to the Tennessee guidance on mutual assistance and mutual aid agreements.
That kind of schedule matters because smaller agencies and specialty partners can't lend people or equipment indefinitely without clarity on cost recovery.
For hospitals working with air medical partners, families often ask whether transport costs will be covered and by whom. That question becomes part of transfer planning fast, which is why resources on air ambulance insurance coverage are useful for case managers and discharge teams.
If reimbursement language is vague, someone in finance will slow the process, and they'll have good reason to do it.
What works in practice
The agreements that hold up operationally tend to do a few things well:
- They use named roles, not vague offices: “Administrator on call” is better than “appropriate representative.”
- They tie reimbursement to documentation: Itemized records, timing, and submission rules reduce disputes later.
- They settle legal friction before an incident: Counsel should argue over indemnity language before activation, not during it.
- They get tested: A tabletop exercise will expose confusion faster than a polished PDF.
Mutual Aid in Action Hospital and Air Ambulance Coordination
A rural or regional hospital stabilizes a critically ill patient, but the patient needs care available only at a distant specialty center. Ground transport would take too long or create clinical risk. The patient also has complex mobility needs, so the transfer requires equipment and crew capability the sending facility doesn't maintain.
That's where a healthcare-specific mutual aid agreement proves its value.
How the activation actually unfolds
The hospital doesn't start by negotiating terms. It follows the agreed activation path. A designated hospital representative contacts the transport partner through a known channel. Dispatch confirms the request type, patient condition, receiving destination, and operational constraints.
The clinical handoff moves faster because expectations were set before the incident. Required documentation, bedside report format, equipment compatibility, and family communication steps are already understood. The air medical crew arrives inside a framework, not a fog of assumptions.
That matters even more when the transfer is clinically sensitive. If the patient is bariatric, ventilated, hemodynamically unstable, or moving between teams with different workflows, standardization reduces friction and protects continuity of care.
In a strong hospital-transport partnership, the agreement does the administrative thinking so the clinicians can focus on the patient.
A plain-language explainer on what an air ambulance really does helps families understand why these transfers involve more than aircraft availability.
The operational side is easier to see in motion:
What this example shows
The value isn't only speed. It's reduced uncertainty.
The hospital knows who to call. The transport provider knows what authority supports the request. The receiving team gets information through an established process. Billing, documentation, and liability questions don't disappear, but they no longer block action at the worst possible moment.
That's what healthcare mutual aid should do. It should make a hard transfer clinically manageable and operationally routine.
Frequently Asked Questions About Mutual Aid
Hospital leaders and case managers usually ask the same practical questions once drafting starts.
Is a mutual aid agreement the same as a vendor contract
Not always. A standard fee-for-service contract usually focuses on purchasing a service. A mutual aid agreement focuses on shared response under defined conditions.
In healthcare, the two can overlap. A private transport provider may still bill for service, but the mutual aid structure adds activation rules, operational coordination, communication standards, and emergency-use terms that a simple vendor agreement may not cover.
Can these agreements be used outside declared disasters
Yes. Modern models are designed to function before, during, and after emergencies, and some allow requests to be made verbally or in writing, with written follow-up required as soon as practical, according to the EMAC intrastate mutual aid model at EMAC's intrastate mutual aid resource.
That flexibility matters in healthcare because many real-world activations aren't headline disasters. They're surge events, service disruptions, planned high-attendance events, or urgent patient movement needs.
How often should a hospital review an agreement
Review it whenever operations change in a meaningful way. That includes changes in service lines, transfer partners, contact roles, dispatch processes, legal requirements, or reimbursement practices.
A document can be legally valid and still be operationally obsolete. If the phone numbers, approval roles, or clinical workflows no longer match reality, the agreement needs revision.
Should agreements be tested in drills
Yes. A tabletop exercise is often enough to expose weak points.
Try a realistic scenario. Use actual call trees, actual documentation steps, and actual after-hours leadership roles. Most hospitals discover gaps in authority, handoff expectations, or finance workflow long before they find problems in legal language.
What's the most common drafting mistake
Teams write broad promises instead of process.
The best agreements answer concrete questions. Who calls whom. What gets shared. Which credentials are accepted. How communication happens. When reimbursement starts. What paperwork follows. If the document can't guide a transfer coordinator or administrator on call, it isn't finished.
If your organization is building or refining transfer partnerships, it helps to work with operators who understand both clinical transport and hospital coordination. Med Jets by Air Trek supports end-to-end medical transportation, including air ambulance flights, medical escorts, and ground coordination. You can learn more about their services at Med Jets by Air Trek.