A call comes in. A transplant team has an organ available. A family member is trying to process what that means. A hospital case manager is already thinking three steps ahead. Which airport, which crew, which handoff, what paperwork, what timing?
In that moment, the organ transport box stops being a vague piece of equipment and becomes something much more personal. It is the system carrying a donor organ through a chain of decisions, vehicles, and people, all under intense time pressure.
If you're coordinating an organ flight, you probably don't need marketing language. You need clear answers. What does the box do? Why are some boxes more advanced than others? Who handles it? What happens during an air ambulance transfer? Those are the questions that matter when a transplant window is open and the margin for error is small.
The Most Important Delivery in the World
When an organ becomes available, nobody experiences it as a simple shipment.
A family may hear, “We have a match.” A case manager may hear, “We need transport locked in now.” The transplant team hears something else: the clock has already started. In the United States, 109,423 people were on the transplant waiting list, including 61,798 active candidates, and the time available to move an organ varies sharply by organ type. Kidneys can be preserved for up to 36 hours, while hearts and lungs generally have only 2 to 6 hours according to UNOS-related market reporting on transplant box logistics.
That difference changes everything.
A kidney flight still has urgency, but a heart or lung transfer often demands a far tighter transport plan. Ground delays matter. Flight availability matters. Handoffs matter. Even small disruptions can force a team to rethink routing, escorting, and receiving readiness.
The organ transport box isn't “the package.” It's part of the clinical plan.
Families often ask, “Why can't they just put it on the next flight?” Sometimes they can't, because organs aren't moved like ordinary cargo. They travel inside systems built to protect temperature, sterility, and handling conditions while the procurement team, transport crew, and receiving hospital stay in constant coordination.
Hospital coordinators often ask a different question: “What information do I need to have ready?” Usually, the answer starts with the organ type, the pickup and destination facilities, the expected handoff timing, and whether the preservation method is passive cold storage or an active perfusion system.
An experienced flight crew sees the same truth every time. The box matters because the organ inside has one job left to do. Reach the recipient in usable condition.
What Is an Organ Transport Box
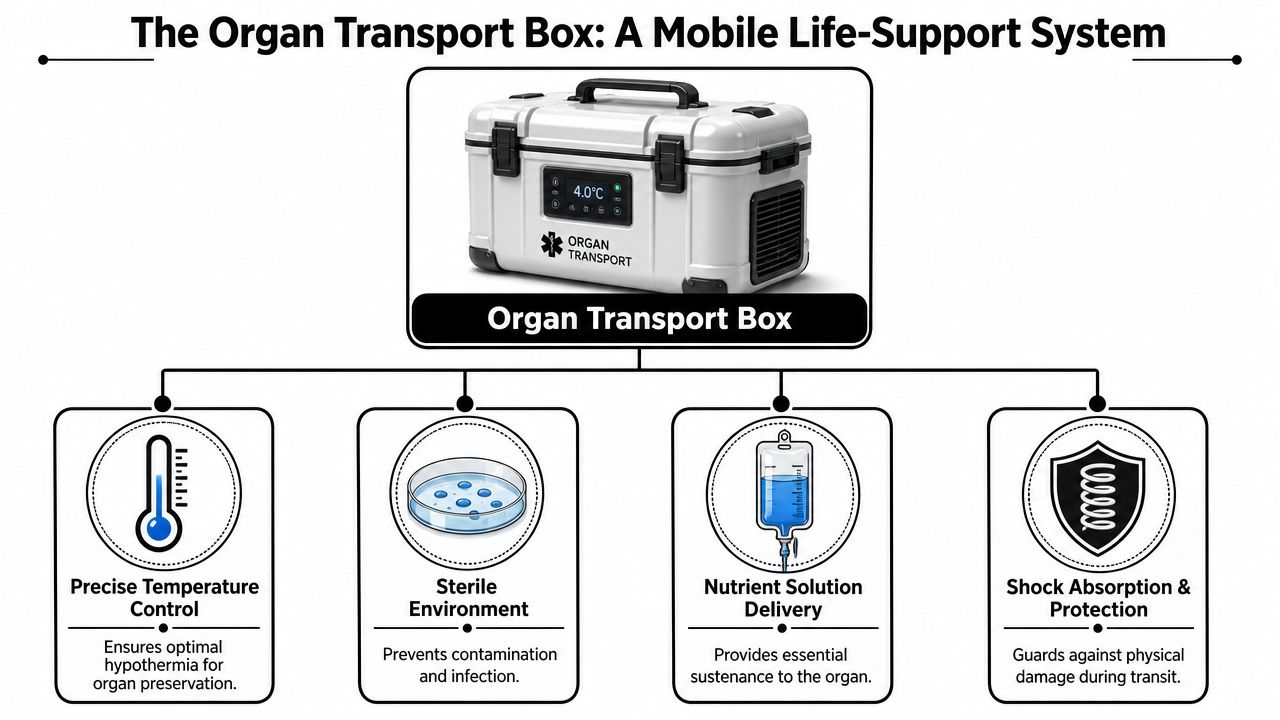
Think of an organ transport box as a mobile protective environment.
It isn't just a hard shell. It's the physical system that helps maintain the organ's required conditions while teams move it from donor hospital to recipient hospital. Depending on the setup, that can mean controlled cooling, sterile packaging, impact protection, and continuous documentation of conditions during transit.
For non-specialists, the easiest way to think about it is this: it's a temporary life-support bubble for an organ that can't protect itself.
From ice chest to controlled transport
For many years, the long-standing clinical standard was a triple-bag system inside an ice box. Medical literature describes that setup as the conventional method before newer devices appeared. That same literature describes the Paragonix Sherpa Pak system as maintaining donor-fluid temperatures in the clinically acceptable range of 4°C to 8°C, holding that range for 24 hours under temperature stress and 30 hours at a constant ambient temperature of 22°C in testing, as reported in this medical review of donor-organ transport technology.
That change may sound technical, but the practical meaning is simple. Older methods relied more heavily on basic insulation and ice. Newer systems are designed and validated to control temperature much more precisely.
What the box is trying to prevent
An organ in transit faces several risks at once:
- Temperature drift can damage tissue if the organ gets too warm or is exposed to uncontrolled conditions.
- Contamination risk has to be minimized through sterile packaging and disciplined handling.
- Physical shock from loading, unloading, and movement can't be ignored.
- Documentation gaps create trouble during handoff, especially when multiple teams are involved.
That's why people get confused when they hear “organ transport box” and assume it's just a cooler. Sometimes the preservation method is mostly passive and the box is the main protective device. Other times, the box is only one part of a larger preservation platform.
Practical rule: Ask whether you're talking about the container, the preservation method, or both. Those are related, but they aren't the same thing.
A common point of confusion
Families sometimes search online for “organ transport box” and end up seeing content that doesn't explain real medical use very well. In actual transplant logistics, the meaningful question isn't what the box looks like. It's what conditions it maintains, how the organ is preserved inside it, and how reliably the transport team can move it without breaking procedure.
That distinction matters during air transport, because the flight plan has to support the preservation method, not just the route.
Passive vs Active Transport Systems
Not every organ transport box works the same way.
Some systems are passive. They preserve the organ by keeping it cold in a controlled container. Others are active. They go beyond cooling and help maintain the organ in a more supported physiologic state during transport.
If you're coordinating a transfer, this isn't an academic distinction. It affects portability, staffing, equipment needs, and how the flight is planned.
What passive systems do well
Passive systems are the familiar workhorses of organ transport. They use insulation, conditioned cooling elements, and validated packaging to maintain the needed temperature range.
They're often chosen because they're simpler to move through airports, ambulances, helipads, and hospital corridors. They also tend to fit more easily into tightly timed logistics where every extra component adds another variable.
A passive system is often the right answer when the preservation strategy is cold static storage and the route is organized around that method.
What active systems change
Active systems treat transport more like portable organ support.
Stanford's MoTEC concept uses a two-compartment thermoelectric design, with an outer recirculating water cooling unit and an inner organ chamber, maintaining tissue at 10°C ± 1°C for over 6 hours with wireless feedback control and up to 4 hours of standalone battery operation. In the same Stanford technology summary, Duke reports that the FDA-cleared TransMedics Organ Care System keeps organs in a functioning state with warm, oxygen- and nutrient-rich blood, and that the heart unit can run on batteries for up to 10 hours while continuously monitoring organ condition during transport. You can see that design approach summarized in Stanford's overview of organ transport technologies including MoTEC and TransMedics OCS.
That's a very different philosophy. Instead of slowing deterioration with cold storage, active systems aim to preserve and assess the organ in a more dynamic way.
For readers who want more background on how these devices fit into transport planning, Med Jets also has a page on the Organ Care System in medical transport.
Passive vs Active Organ Transport Systems at a Glance
| Feature | Passive Systems (e.g., SherpaPak) | Active Systems (e.g., TransMedics OCS) |
|---|---|---|
| Core approach | Cold preservation in a controlled container | Perfusion or active physiologic support during transport |
| Main strength | Simplicity and easier logistics | More data and a more supported transport environment |
| Equipment burden | Lower | Higher |
| Portability | Easier through routine handoffs | More complex to move and set up |
| Monitoring | Usually focused on temperature and handling conditions | Includes ongoing organ-condition monitoring |
| Best fit | Straightforward cold-storage pathways | Cases where physiologic support may expand transport options |
Which one should a coordinator expect
Case managers often ask, “Which system is better?”
The honest answer is that the right system depends on the organ, the clinical plan, the transplant center's protocol, and the route. Better for one case may be unnecessarily complex for another. The transport team has to match the aircraft, ground support, timing, and handoff process to the preservation method already chosen by the clinical side.
That's why a flight coordinator should ask one early question: Is the organ traveling in passive cold storage or on an active support platform? That answer shapes the whole movement plan.
Critical Specs for Organ Viability
The most important numbers in organ transport aren't there for paperwork. They exist because tissue changes minute by minute once blood supply is interrupted.
An organ removed for transplant enters a period clinicians often describe through cold ischemia, the time the organ is without normal blood supply while preservation methods try to slow damage. Cooling the organ reduces metabolic demand. That buys time, but only if the temperature is controlled carefully.
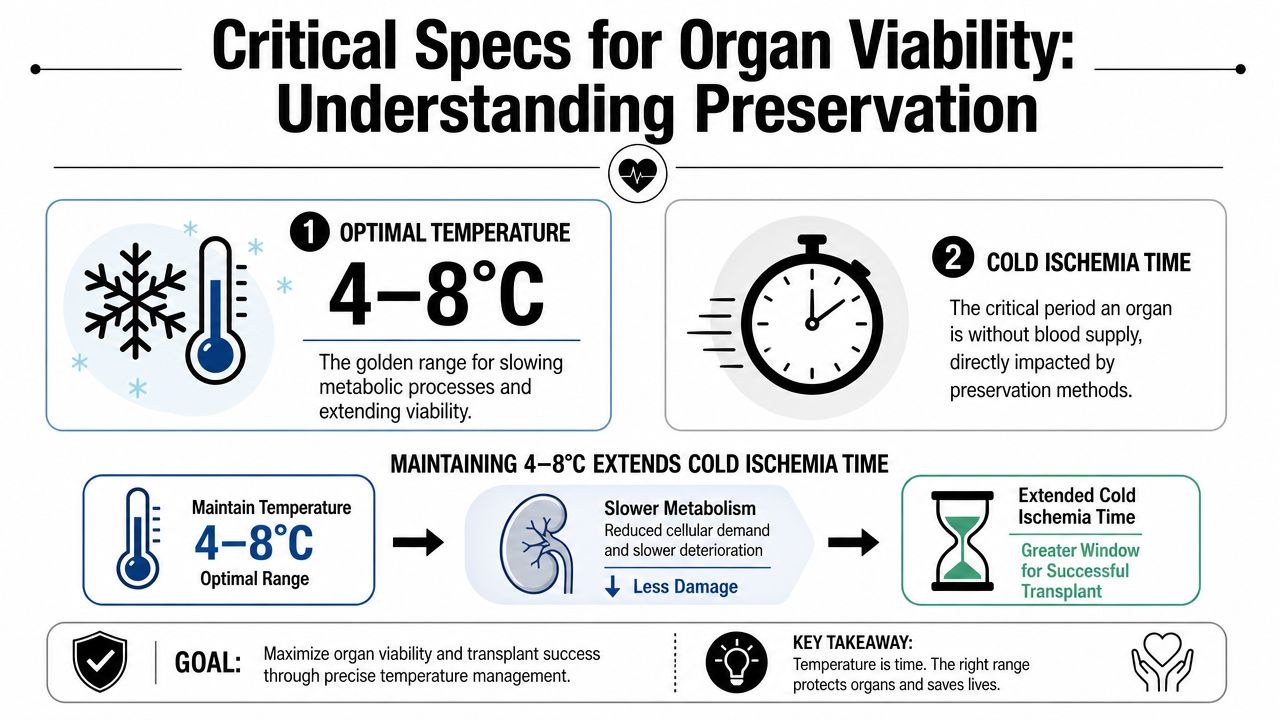
Why the temperature window matters
When people hear that a passive transport system aims for 4°C to 8°C, it can sound oddly narrow. But that range matters because the goal isn't just “keep it cold.” The goal is to slow the organ's metabolism without exposing it to uncontrolled conditions that can create new problems.
In plain language, the organ needs a protected middle ground. Too much variation creates risk. Too little control leaves too much to chance.
That's why validated transport systems matter. Validation means the device has been tested to show it can hold the required range under real-world stress, not just in ideal lab conditions.
Why coordinators should care about validation
A coordinator may never touch the box itself, but they still need to understand what the specs mean operationally.
If a system is validated, the transport team can plan around known performance instead of guessing. That affects routing, tarmac exposure, handoff timing, and contingency planning. It also helps the receiving center trust the documentation that arrives with the organ.
Keep asking one question during planning: “How is the organ's condition being protected and verified during every leg of the trip?”
This same mindset shows up in other medical cold-chain fields. For readers who want a practical look at how temperature-controlled handling is managed in another sensitive healthcare context, BFC Logistics' pharma cold transport is a useful comparison point. The products are different, but the operational discipline around controlled conditions is easy to recognize.
What to confirm before transport starts
A hospital coordinator doesn't need to become an engineer. They do need a short checklist:
- Preservation method: Confirm whether the organ is in passive cold storage or an active support system.
- Monitoring record: Ask what data will travel with the organ, such as temperature documentation or device-readout records.
- Transfer timing: Make sure every team knows the planned handoff windows.
- Receiving readiness: Verify that the destination team is prepared to accept the organ immediately on arrival.
If you're arranging air movement, the transport provider's role is to fit those requirements into the aircraft and ground sequence. Medically oriented transfer details for that kind of planning are outlined on medical organ transport coordination.
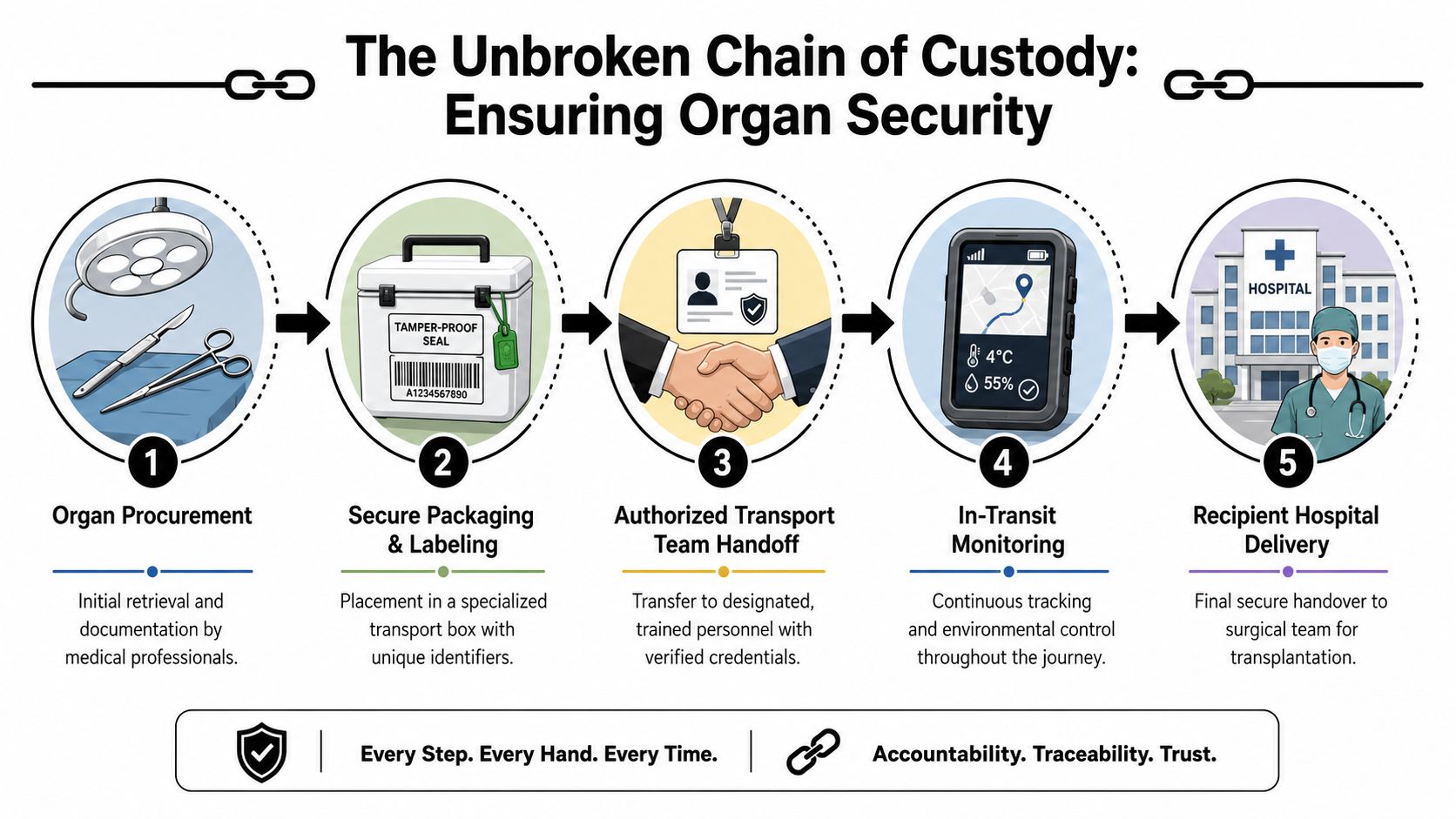
The Unbroken Chain of Custody
An organ flight is a relay. The box is the baton.
What keeps the process safe isn't one person holding it the whole time. Safety comes from a series of controlled handoffs where each team knows exactly when it receives the organ, what condition it's in, and who takes responsibility next.
That's what people mean by chain of custody.
Who handles the box
Public discussions sometimes treat an organ transport box like a sealed cooler that anyone can carry from point A to point B. Real transport isn't that casual.
The process involves documented handoffs between procurement teams, couriers, flight crews, and receiving hospitals, with emphasis on sterile handling, time tracking, and continuous monitoring to reduce risk from delays or disruptions, as described in this discussion of the practical chain-of-custody issue around organ transport handling and monitoring.
In practice, only authorized, trained personnel should be handling the box during movement. Even when family members are nearby, they usually aren't part of that custody chain.
What happens at each handoff
A strong handoff is more than passing the container to another set of hands. It usually includes:
Identity confirmation
The team confirms the organ and destination details against documentation and labeling.Condition review
The receiving handler checks that the packaging and monitoring status appear correct.Time logging
The exact handoff time is documented because time matters clinically and operationally.Responsibility transfer
One team releases custody only when the next team has formally accepted it.
That's why an apparently small delay at the loading area can matter. It isn't just waiting. It may interrupt documentation flow, environmental control, or the timing of the next leg.
A clean chain of custody reassures everyone involved, from the transplant surgeon to the family waiting at the destination.
Questions families often ask
Families sometimes ask, “Is the organ ever left unattended?”
The goal of professional transport planning is to avoid that. The movement should be organized so the organ remains under active responsibility throughout the trip, including during airport, ambulance, and hospital transitions.
Another common question is, “What if a commercial flight is delayed?” That concern is one reason transplant logistics may rely on dedicated medical or specialized transport arrangements instead of routine travel pathways for time-sensitive organs.
For coordinators, the key takeaway is simple. Don't think only about the aircraft. Think about every doorway, elevator, ramp, and receiving desk between the donor site and the OR.
Coordinating an Air Ambulance Organ Transfer
When an organ transfer involves an aircraft, the medical and aviation plans have to run together.
That means the crew has to know more than the airport pair. They need the pickup point inside the sending facility, the receiving team's contact path, the preservation setup, the expected handoff sequence, and how ground transport connects to the flight segment.
What to have ready when you call
If you're a hospital case manager or transplant coordinator, gather these details before speaking with the flight provider:
- Sending and receiving facilities with exact locations for handoff
- Organ type and the preservation approach being used
- Current timing for procurement completion and readiness for departure
- Receiving contact information for the transplant center team
- Ground transport needs on both ends of the flight
- Any special equipment considerations tied to the transport system
Those details help the flight team decide aircraft loading, crew positioning, departure timing, and ground coordination.
One example of a provider that coordinates this type of mission is Med Jets organ recovery transport, which describes the operational side of aligning air and ground movement around time-sensitive medical transfers.
What the day of transport usually looks like
On the day itself, the process often feels fast because the planning has already been compressed.
The organ is packaged and documented by the clinical team. It moves through an authorized handoff to the transport team. Ground movement to the aircraft is synchronized to reduce idle time. During flight, the crew protects the environment around the transport system and stays in communication with the receiving side so the arrival handoff happens without unnecessary waiting.
A short visual overview can help if you're new to this workflow:
What families should expect
Families usually aren't managing the box itself. Their role is different.
They may be updated on timing, destination hospital readiness, and the larger transplant plan, but the organ transport chain is handled by the trained teams assigned to it. The most helpful thing a family can do is stay reachable and direct logistical questions through the care team or transport coordinator rather than trying to intervene in the handoff process.
That separation can feel unsettling at first. It is a safety feature. The fewer improvised steps, the better.
Frequently Asked Questions for Organ Flights
Can a family member ride with the organ
Usually, families don't travel as part of the organ's custody chain. The organ moves under the control of authorized medical and transport personnel. Family travel, when arranged separately, follows a different plan.
What if weather or airport congestion becomes a problem
Teams plan around that risk with route choices, timing buffers where possible, and constant communication across the handoff chain. For urgent organs, the transport decision often reflects how little delay the clinical window can tolerate.
Who is responsible during each leg of the trip
Responsibility transfers through documented handoffs. The procurement team, courier or ground team, flight crew, and receiving hospital each have defined custody points. That's one reason the process looks so formal. It needs to.
Is an organ transport box the same as organ preservation technology
Not always. Sometimes the box is mainly a controlled container for cold storage. In other cases, the transport setup includes active preservation technology as part of the system.
Do all hospitals use the same transport pathway
No. Capabilities differ by region, organ type, available aircraft, and the preservation method selected by the transplant program. If you want a broader logistics perspective on sensitive human tissue and organ handling, AUSFF's specialized freight solutions offer a useful example of how specialized transport providers frame these requirements.
What should a case manager ask first
Start with three points: What organ is being moved, how is it being preserved, and what are the exact handoff locations and times? Those answers usually clarify the rest of the transport plan quickly.
An organ transport box can look simple from the outside. In real transplant work, it's one of the most carefully managed pieces of equipment in the entire chain. When families and coordinators understand what it does, why the specs matter, and how custody is maintained, the process becomes less mysterious and much easier to support.
If you're coordinating a time-sensitive medical transfer and need help understanding the flight side of the process, contact the appropriate transplant and air medical teams early. Clear timing, clear custody, and clear communication give the organ its best chance to arrive ready for the patient who needs it.