A hospital discharge is set for this afternoon. Your mother cannot sit upright for long, the nurse says she needs monitoring on the way, and someone asks whether the trip home or to another facility should be by ambulance. The next question usually comes fast: will Medicare pay, or is this going to turn into a bill the family did not expect?
Medicare can pay for ambulance service in some situations, but coverage depends on more than whether a doctor ordered the ride or a facility arranged it. If Medicare does cover the trip, Part B generally pays 80% of the Medicare-approved amount after the deductible is met. For 2026, the Part B deductible is $257, according to Medicare's official guidance.
The hard part is that families often hear “transport is needed” and assume that means “transport is covered.” Medicare does not use those terms the same way. A ride can be appropriate from a care planning standpoint and still fail Medicare's coverage rules if the record does not clearly show why a car, wheelchair van, or other option would have been unsafe.
That is why paperwork matters almost as much as the ride itself.
Before transport, you want a clear reason the patient needs ambulance-level care. During transport, the crew's notes should match the patient's condition and the services provided. After transport, the claim needs to tell a consistent story. If one piece is vague or missing, coverage gets harder.
This article is built for that real-world problem. It will help families and case managers work through the rules, spot the documentation that matters, and use simple checklists before, during, and after a trip so there is a better chance Medicare will pay and fewer surprises if it does not.
When Is an Ambulance Ride Covered by Medicare
A common scene looks like this: a hospital tells a family their loved one can't safely ride home by car, or a nursing facility says a patient needs transfer to a hospital for urgent evaluation. In that moment, people often assume that if an ambulance is used, Medicare will pay.
Sometimes it will. Sometimes it won't.
The rule that decides almost everything
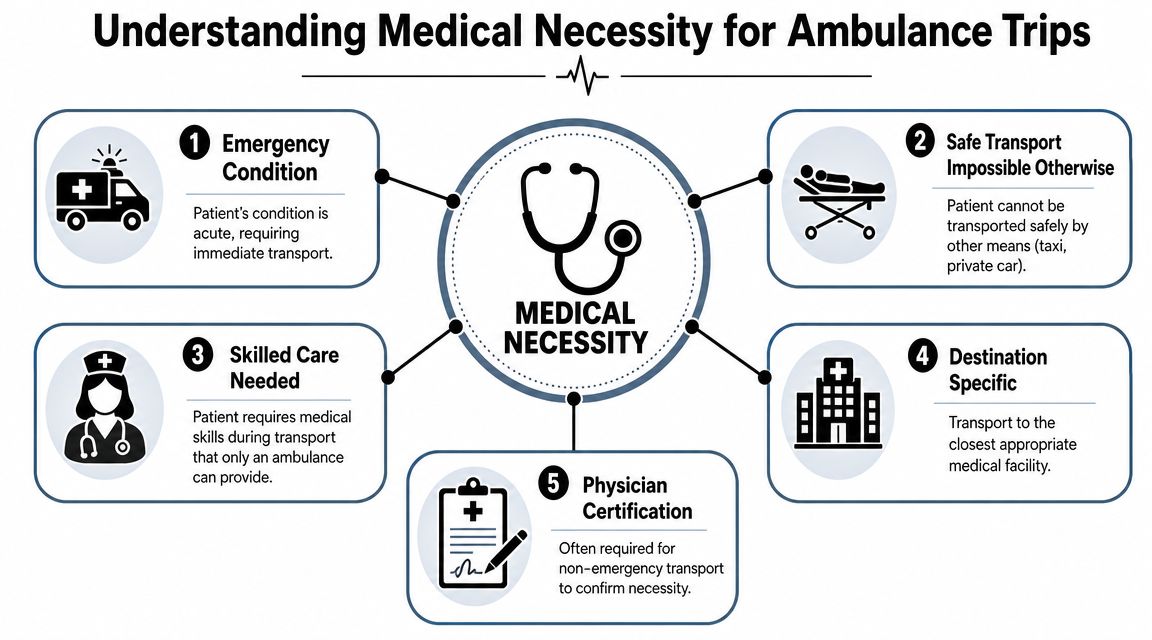
The key word is medical necessity. Medicare covers ambulance transportation under Part B when the patient's condition is such that transportation by car, taxi, wheelchair van, or another non-ambulance vehicle would be unsafe.
That means the ambulance itself must be the appropriate level of transport for the patient's condition. The fact that a person is elderly, weak, in pain, or has no family available to drive does not automatically make ambulance transport covered.
Practical rule: Ask one question first: "What would make a regular vehicle unsafe for this patient today?" If no one can answer that clearly, coverage may be difficult.
What Medicare is looking for
Medicare's standard rule focuses on a few basic issues:
- The patient's condition: The patient must need ambulance-level transport because another vehicle could put their health at risk.
- The destination: The ride usually must go to the nearest appropriate facility able to provide the needed care.
- The type of trip: Emergency trips are often easier to justify than scheduled, non-emergency transfers, but both can be covered if the facts support them.
- The level of transport: Ground ambulance is the default. Air ambulance may be covered in narrower situations when ground transport can't provide the needed speed or access.
Where families get tripped up
People often confuse three different ideas:
- A doctor ordered it
- The patient needs help getting there
- Medicare considers the ambulance medically necessary
Those are not the same thing.
A physician order helps, especially for planned transport, but Medicare still looks at the actual medical facts. If the record doesn't show why a private car or other vehicle would have been unsafe, a claim can still be denied.
The practical takeaway
When people ask, "Will Medicare pay for ambulance service?" the honest answer is: Yes, but only if the ride meets strict coverage rules. The strongest claims are the ones where the record clearly shows what the patient could not safely tolerate, what care was needed during transport, and why the chosen destination was appropriate.
What Medically Necessary Really Means for Ambulance Trips
A family often hears, “The doctor ordered an ambulance,” and assumes coverage will follow. That is where many claims go off track. Medicare looks for proof that the patient needed ambulance-level transport at that moment, not just proof that the patient was ill or that the ride was ordered.
The question Medicare is really asking
The practical test is simple: what would likely happen if this person went by car, wheelchair van, or another lower level of transport?
That framing helps because families often focus on the diagnosis, while Medicare focuses on the transport risk. A stroke workup, severe breathing trouble, uncontrolled pain with movement, oxygen needs, confusion that makes safe sitting impossible, or the need for monitoring during the ride can support coverage. A serious diagnosis by itself does not settle the issue.
A good working rule is this: the chart should show why another vehicle would have been unsafe, not just inconvenient.
What counts as medical necessity in real life
Medical necessity usually becomes clearer when you picture the ride itself.
More likely to fit the rule
- The patient cannot safely sit upright or transfer into a car. For example, severe weakness, spinal precautions, uncontrolled vomiting, or pain that sharply worsens with movement.
- The patient needs care during transport. Oxygen management, monitoring, suction, or trained staff ready to respond if the condition changes.
- The patient's condition could worsen from delay or ordinary transport. Time-sensitive symptoms or unstable vital signs often matter more than the diagnosis label.
- The record explains the current problem in specific terms. “Unable to tolerate sitting more than a few minutes” is stronger than “needs assistance.”
Less likely to fit the rule
- The patient needs a ride, but not ambulance-level care. This is common with routine office visits or scheduled follow-up appointments.
- The trip would be difficult, but not medically unsafe, by another vehicle.
- The reason is convenience. Family distance, lack of a driver, or general preference for an ambulance usually does not establish coverage.
A signed physician order supports the plan. It does not prove coverage by itself.
The paperwork that helps claims hold up
Families and case managers can improve the odds of payment by treating the chart like a checklist. If the record leaves out the “why,” Medicare may decide the ride could have happened another way.
Before transport, try to confirm that the record answers these questions:
- What can the patient not do safely right now? Sit upright, bear weight, transfer, protect the airway, remain calm, or travel without observation.
- What skilled service is needed during the ride? Monitoring, oxygen, suction, stretcher transport, restraint for safety, or rapid clinical response.
- What changed today? Coverage decisions often turn on the patient's present condition, not a past diagnosis.
- Why is a lower level of transport unsafe? This point should be written plainly.
During the handoff, ask staff to document facts, not shorthand. “Bed confined” alone may not tell the full story. A stronger note describes mobility limits, mental status, fall risk, oxygen needs, pain with movement, recent symptoms, and what happened when staff tried to reposition or transfer the patient.
After the ride, keep copies of everything you can get. That includes the transport record, sending notes, discharge papers, physician certification if one was used, and any notice showing the destination and level of service. If the claim is questioned later, those records become your proof.
Families dealing with aircraft transport often run into an even higher documentation bar. This guide on when Medicare covers air ambulance can help you compare what ground and air claims usually need.
A short explainer can help if you're dealing with this in real time:
Questions to ask before agreeing to transport
If you are arranging a non-emergency trip, ask these before the patient leaves:
- What specific medical risk makes a car or wheelchair van unsafe today?
- Where is that risk documented in the chart?
- Does the note describe the patient's current condition, not just the diagnosis?
- What care or monitoring is expected during transport?
- If a physician certification is needed, has it been completed and added to the record?
Those questions can feel uncomfortable in a stressful moment. They still matter. A two-minute clarification before the ride can prevent a much bigger fight after the bill arrives.
Ground vs Air Ambulance Medicare Rules You Must Know
Ground and air ambulance rides don't get reviewed the same way. Medicare generally treats ground ambulance as the standard option and air ambulance as the narrower exception.
A simple way to think about it is this: in Medicare's eyes, a helicopter or medical jet is usually a last-resort transport, not a first choice.
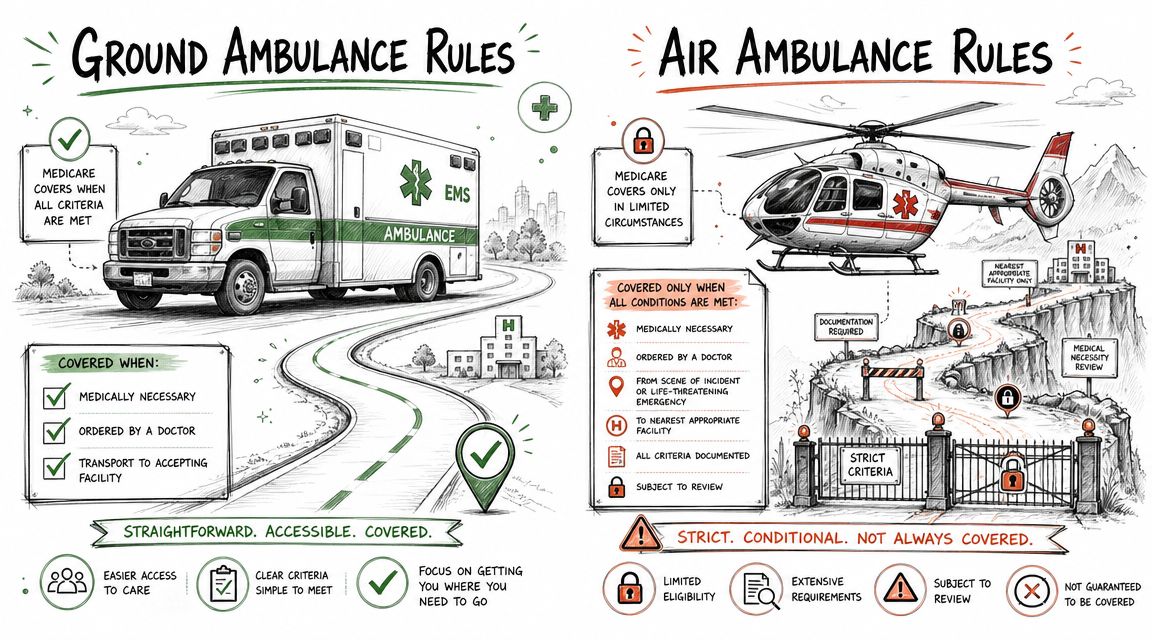
How ground ambulance is usually evaluated
Ground ambulance claims usually rise or fall on the patient's condition and whether another vehicle would have been unsafe. If a patient needed stretcher transport, urgent medical supervision, or transport to a facility that could provide the needed care, a ground claim may fit the rules.
Ground transport is also the comparison point when an air claim is reviewed. Medicare asks whether a ground ambulance could have handled the trip safely and appropriately.
When air ambulance enters the picture
Air ambulance can come into play when ground transport can't provide the needed speed or access. That may happen because of distance, location, terrain, or the patient's condition. The issue isn't whether air transport is impressive or faster in general. The issue is whether it was necessary for this patient, on this trip.
For families trying to sort out those distinctions, this explanation of whether Medicare covers air ambulance is a useful background read.
The nearest appropriate facility rule matters more than people expect
One of the costliest misunderstandings involves destination choice. Families often want transfer to a hospital they already know, a larger city, or a physician they prefer. Medicare's rule is narrower.
CMS states that ambulance transport must go to the nearest hospital, critical access hospital, or skilled nursing facility capable of furnishing the needed level of care. If the patient is taken farther away by choice, Medicare generally pays only up to the cost of transport to the nearest appropriate facility, as explained in Medicare's ambulance coverage publication.
If the debate is between "best known hospital" and "nearest appropriate hospital," Medicare cares about the second one.
Questions to ask during transfer planning
Use these questions before approving a ground or air move:
- Why isn't ground enough? Ask for the clinical reason, not a general statement.
- What makes the destination the nearest appropriate facility? That phrase should appear in the transfer reasoning.
- Is this move based on medical need or family preference? If it's preference, expect possible payment limits.
- Who is documenting the need for speed, access, or specialty care? Air claims need that reasoning in the record.
If you're coordinating a transfer, those answers should come from the treating team and appear in the medical file, not just in verbal conversation.
How Medicare Parts A B and Advantage Cover Ambulance Costs
Most families hear "Medicare" and think of it as one bucket. It isn't. Ambulance billing gets confusing because different parts of Medicare may apply, and Medicare Advantage plans can add their own administrative rules.
The short version
For most ambulance rides, Part B is the part people need to understand first. That's where the core ambulance coverage rules usually sit.
Part A can matter in some facility-based situations, but it isn't where most families should start when they receive an ambulance bill. Medicare Advantage can cover ambulance services too, but plan rules may affect how the claim is processed.
Medicare ambulance coverage by part
| Medicare Part | Typical Use Case | Cost Sharing (after deductible) | Key Considerations |
|---|---|---|---|
| Part A | Certain inpatient or facility-related episodes where transport is tied to covered institutional care | Varies by the underlying inpatient or facility coverage situation | Often less straightforward for families reviewing a separate ambulance bill |
| Part B | Most emergency and non-emergency ambulance claims reviewed under Medicare's ambulance rules | If covered, the patient generally owes 20% after the deductible because Medicare pays 80% of the approved amount | This is the part most people are dealing with when asking whether Medicare will pay |
| Medicare Advantage | Ambulance coverage through a private plan that must provide at least Medicare-covered services | Depends on the plan's terms, copays, and claim rules | Prior authorization, plan procedures, and provider requirements can matter |
What families should do with Original Medicare
If the patient has Original Medicare, focus on four questions:
- Was the ambulance medically necessary?
- Was the destination appropriate?
- Was this the nearest suitable facility?
- What documentation supports the level of transport?
Those questions often matter more than anything else.
What changes with Medicare Advantage
Medicare Advantage plans must cover Medicare-covered services, but the process may not look the same as Original Medicare. A plan may require pre-service review for some non-emergency transport situations, have specific claims procedures, or involve contracted providers.
That means the family or case manager should never assume "Medicare rules" are the whole story if the patient has an Advantage plan. The plan documents and member services line matter.
If you're comparing broader insurance issues around ambulance billing, this overview of whether medical insurance covers ambulance transport can help frame the differences.
The fastest way to avoid a billing surprise with Medicare Advantage is to call the plan before a scheduled transport and document the call reference, the representative's name, and what you were told.
A practical way to think about costs
People often ask whether Medicare pays the full ambulance bill. Usually, the answer is no. Even when a ride is covered, patients may still owe their share under the applicable Medicare or Medicare Advantage rules.
That's why it's smart to ask the ambulance provider whether they participate with Medicare, whether they expect any upfront paperwork, and whether they believe the transport meets Medicare's medical necessity standard.
Your Pre-Flight Checklist for Arranging Medical Transport
When a transport is scheduled instead of happening through 911, you have a chance to reduce billing problems before the wheels move. In such instances, families and case managers can make the biggest difference.
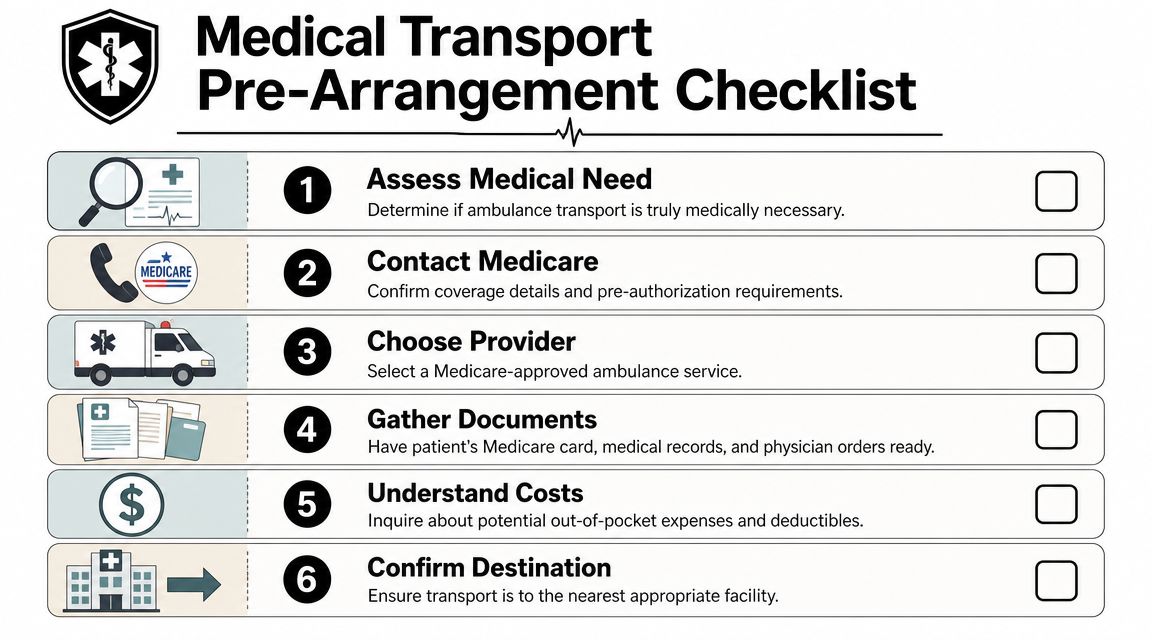
Before you book the transport
Start with the medical reason. Don't ask, "Can we get an ambulance?" Ask, "What documentation shows this patient needs ambulance-level transport?"
Then build your file.
- Get the physician order: For scheduled transports, ask for the written order and any certification used to support medical necessity.
- Pull the current clinical notes: The strongest notes describe present condition, mobility limits, monitoring needs, and transfer risks.
- Confirm the receiving facility: Make sure the chart reflects why that destination is clinically appropriate.
- Check the patient's coverage type: Original Medicare and Medicare Advantage may follow different administrative paths.
Questions for the ambulance company
This part matters. The provider may submit the claim, but your documentation affects whether it stands up.
Ask these questions plainly:
- Are you enrolled in Medicare?
- What records do you need from the sending facility before transport?
- If this is non-emergency, do you require physician certification or additional forms?
- What destination will appear on the transport record?
- Who should receive any follow-up records request after the claim is filed?
If the move involves a higher-acuity transfer, one available option in the market is Med Jets by Air Trek, which coordinates medical flights, ground components, and transfer logistics. That doesn't change Medicare's rules, but it shows why documentation and destination planning need to happen early.
What should travel with the patient
A smooth transport often depends on basic paperwork being ready at pickup.
- Insurance and identification: Medicare card, plan details if there is a Medicare Advantage plan, and patient identifiers.
- Clinical packet: Recent history and physical, medication list, nursing notes, physician order, and reason for transfer.
- Receiving acceptance details: Name of facility, accepting service, and contact information.
- Special transport needs: Oxygen needs, bariatric handling concerns, isolation precautions, or escort information.
A missing chart note can create more claim trouble than a missing family explanation. Medicare pays based on the medical record, not the family's memory of what happened.
A same-day transport checklist
Use this quick review before departure:
- Verify the current condition: Make sure the chart reflects the patient's status on the day of transport.
- Confirm the destination: The paperwork should match the actual receiving facility.
- Match the vehicle to the patient: Ground, air, stretcher, monitoring level, and crew skill should fit the documented need.
- Document handoff names: Note who gave report and who accepted the patient.
- Keep copies: Families and case managers should keep the order, certification, and transfer notes when possible.
When those items are handled up front, the claim is easier to defend later.
What to Do When Medicare Denies Ambulance Coverage
A denial letter feels personal, especially when the transport happened during a crisis. It usually isn't personal. It usually means the claim record didn't prove what Medicare needed to see, or the contractor believes the transport didn't meet a coverage rule.
That still leaves room to respond.
Start with the denial reason
Read the notice carefully. Most ambulance denials point back to one of a few issues:
- Medical necessity wasn't established
- The destination wasn't considered appropriate under Medicare's rules
- The documentation was incomplete
- The transport level wasn't justified
Don't argue in general terms. Respond to the stated reason with records that fill the gap.
A workable appeal approach
Think of the first appeal like building the file Medicare should have had from the beginning.
- Pull the run sheet: The ambulance record often includes the patient's condition during pickup and transport.
- Get hospital and facility notes: Sending and receiving notes can show why the transfer was clinically appropriate.
- Ask the physician for a focused statement: The best statements explain why another form of transport would have endangered the patient, using the patient's condition at the time.
- Submit the appeal promptly: Delay doesn't improve the file.
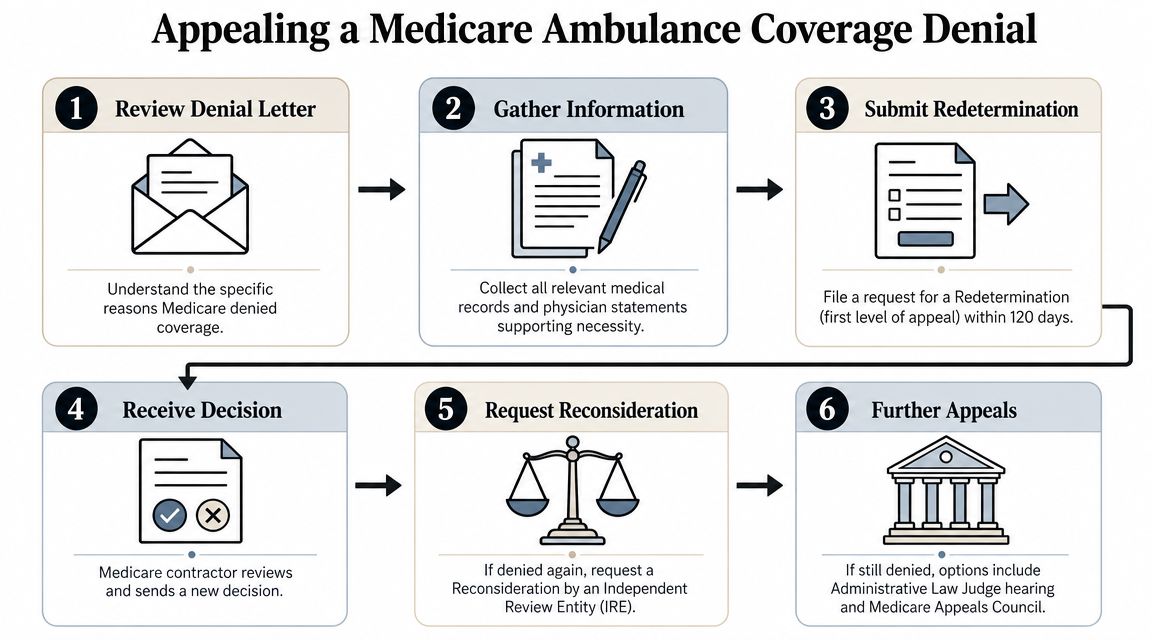
The first level of appeal is called a Redetermination, and the appeal process can continue beyond that if needed. If the first appeal fails, the next step is a Reconsideration by an independent reviewer.
What a stronger appeal sounds like
A weak appeal says: "The patient needed the ambulance."
A stronger appeal says: "On the date of transport, the patient could not safely travel by private vehicle because of the documented condition, required stretcher transport, and needed medical supervision during transfer."
That difference matters.
If the denied transport involved air medical services or a higher-acuity move, this guide on whether insurance covers air ambulance may help you think through how insurers often analyze these claims.
Appeals work best when they stay factual, specific, and tied to the medical record. Emotion explains why the bill matters. Documentation explains why the claim should be paid.
Your Top Ambulance Coverage Questions Answered
Families usually end up with a handful of very specific questions after reading the rules. These are the ones I hear most often.
Will Medicare cover an ambulance to a doctor's office
Usually, this is a hard sell unless the patient's condition required ambulance-level transport and the destination fit Medicare's coverage rules. In most routine office-visit situations, Medicare is less likely to view an ambulance as necessary if another safe transportation option existed.
The practical question isn't whether the appointment matters. It's whether the ambulance was the only safe way to get the patient there.
What if the ambulance company says Medicare may not pay
Take that warning seriously. It often means the provider sees a documentation gap or believes the trip falls outside Medicare's standard criteria.
Ask for specifics:
- What part of the trip may not qualify?
- Is the concern medical necessity, destination, or plan rules?
- What additional records would support the claim?
If a denial has already happened and you're trying to understand next steps more broadly, this consumer guide on what to do if insurance denies claim offers a practical way to think through records, deadlines, and written follow-up.
Will Medicare pay if the family asks for a farther hospital
Many people find this surprising. If a patient is taken beyond the nearest facility that can provide the needed care because of family or patient preference, Medicare may limit payment to what it would have paid for transport to the nearest appropriate facility.
That doesn't mean the farther transfer can never happen. It means the extra distance may create a larger bill unless the record shows why the more distant facility was medically required.
Does a doctor's order guarantee coverage
No. It helps, but it doesn't guarantee payment.
Medicare looks at the patient's condition, the transport risks, and the record supporting the need for ambulance-level service. The order should match the facts already in the chart.
What should families save after the trip
Keep a file with:
- The ambulance bill and any Medicare Summary Notice
- The physician order or certification
- Sending and receiving facility paperwork
- Any denial letters or requests for records
- Notes from calls with the plan or provider
That file makes a big difference if the claim stalls or gets denied.
When people ask, Will Medicare pay for ambulance service, the safest answer is this: it can, but only when the facts, destination, and documentation all line up with Medicare's rules. If you're helping a loved one, don't wait until the bill arrives to ask questions. The best time to protect coverage is before the transport starts.
If you're coordinating a medically complex transfer, keep the paperwork tight, confirm the destination rationale, and ask the transport team exactly how the ride meets Medicare's medical necessity standard. Those few steps can save weeks of confusion later.