A donor organ is available. The recipient team is ready. The problem is distance, time, and risk.
That's the moment when case managers, transplant coordinators, and families start asking the same questions. Can the organ make it in time? Is the organ still viable after transport? Does the flight team understand the equipment? Who is coordinating the handoff from donor hospital to aircraft to transplant center?
An Organ Care System, or OCS, changes that conversation. Instead of treating transport as a race against cold-storage decline, it gives transplant teams a way to preserve and assess certain organs in a more physiologic state during travel. For hospitals, that can mean more options. For families, it can mean a chance that might not have existed under older transport limits. For air medical coordination, it means the mission has to be planned with far more precision than “cooler on board and wheels up.”
The New Era of Organ Viability
A case manager might get the call late in the evening. A heart is available, but the donor hospital is far enough away that traditional timing becomes uncomfortable fast. The receiving surgeon wants the organ moved without unnecessary delay. The family wants a simple answer. Can this be done safely?
That's exactly where the Organ Care System has changed modern transplant logistics.
Why this matters right now
The OCS is no longer an experimental concept sitting at the edge of transplant medicine. It's part of a growing operational reality. One market analysis valued the organ care system market at about USD 225.0 million in 2024 and projected a 14.1% CAGR, with heart applications making up an estimated 43% of total OCS revenue in 2024 according to Strategic Market Research's Organ Care System market analysis.
That kind of growth usually points to a simple truth. Hospitals adopt technology when it answers a real problem. In this case, the problem is that conventional preservation has limits, especially when procurement distance, donor complexity, or recipient readiness create a narrow window.
For case managers, the practical takeaway is straightforward. The transport question is no longer only about miles. It's about whether the organ is being moved in a passive state or an actively managed one.
What changes on the ground
With OCS-supported procurement, transport planning becomes more deliberate and often more complex. The organ isn't just packaged and sent. It may require dedicated device handling, perfusion oversight, power awareness, secure loading, and tighter communication between the donor team, flight crew, and receiving center.
Operational reality: The best OCS missions succeed because the clinical team and transport team build one timeline, not two separate ones.
That's why case managers often benefit from working with teams familiar with organ transport coordination before a mission is underway. The technology can extend possibilities, but only if the transport plan supports it from the start.
What Is an Organ Care System
The easiest way to explain an Organ Care System to a non-engineer is this. It's a portable ICU for an organ.
Instead of placing an organ in static cold storage and waiting until arrival to find out how it tolerated the trip, the OCS gives the transplant team an active platform for preservation and monitoring during transit.
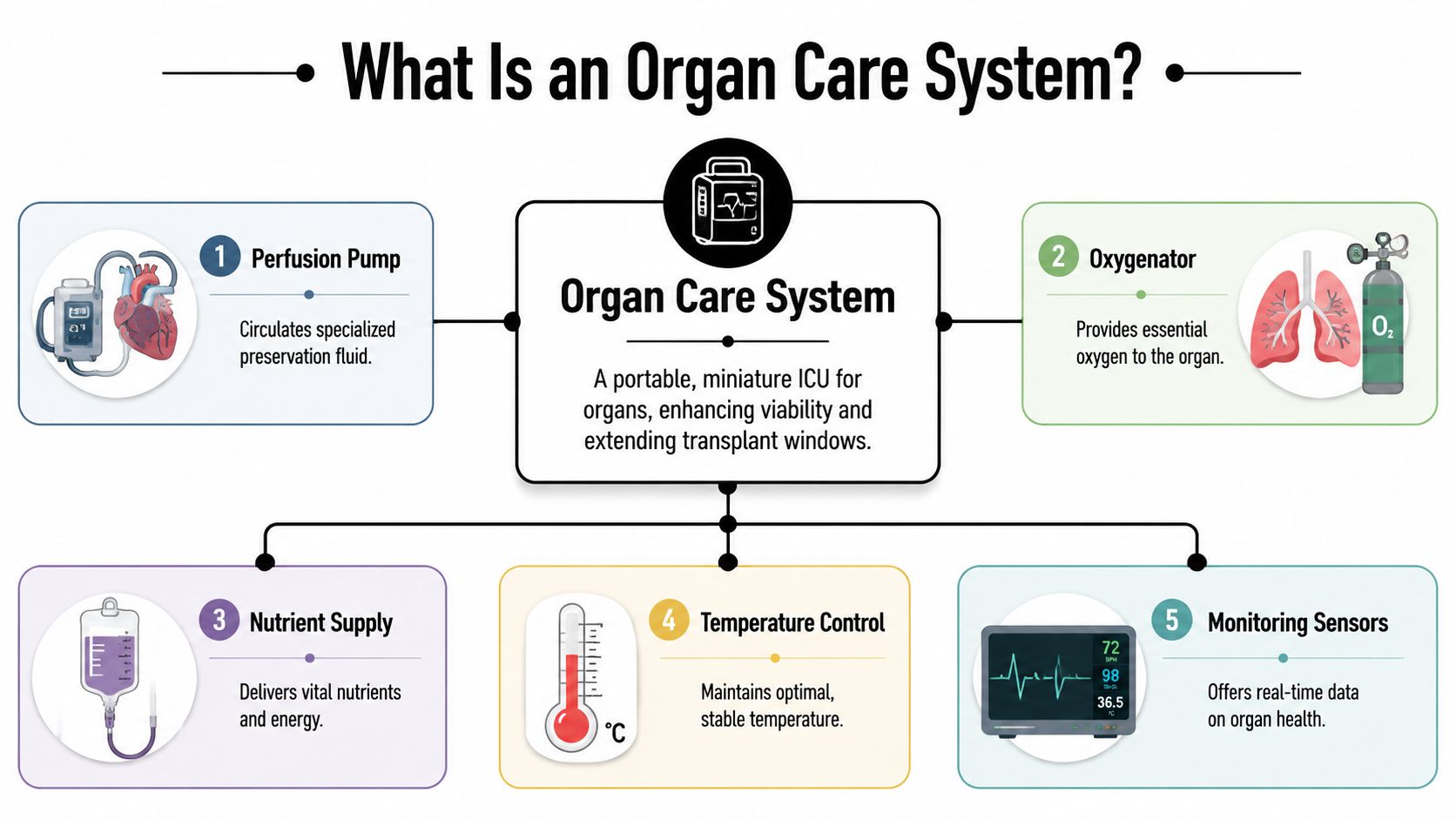
The three main parts
The FDA documentation describes the OCS architecture as an organ-specific console, a single-use sterile perfusion module, and a solution set, with closed-loop instrumentation for pressure, flow, and oxygenation that supports real-time assessment during transit in the FDA device summary for the OCS Heart System.
Here's what that means in plain terms:
- The console handles the core mechanics and monitoring. In the heart configuration, it includes the pump, battery support, warming capability, and key displays.
- The perfusion module is the sterile, organ-facing component. It contains the circuits and embedded sensors that help clinicians track how the organ is doing.
- The solution set supports the perfusion environment. It's part of the system that allows the organ to be managed outside the body under controlled conditions.
Why the sensors matter
This is the biggest difference from a cooler. With static cold storage, the organ is largely a black box until it arrives. With an Organ Care System, clinicians can monitor parameters in transit and adjust management based on what the organ is showing them.
That changes decision-making.
A surgeon or perfusion team isn't waiting until the receiving hospital to discover a problem that started hours earlier. They have a better view of organ status during the trip itself. For air transport teams, that means the device has to be treated as active medical equipment, not luggage.
What a case manager should understand
You don't need to know every engineering detail to coordinate an OCS move well. You do need to understand the implications.
| OCS component | What it does in practice | Why transport teams care |
|---|---|---|
| Console | Runs perfusion and displays monitored values | Needs secure placement and handling |
| Sterile perfusion module | Interfaces directly with the organ | Must remain protected and undisturbed |
| Solution set | Supports the preservation process | Requires correct setup and readiness |
The transport team has one job beyond speed. Protect the clinical environment the OCS is creating.
That's why experienced coordination matters. Delays, rushed loading, poor handoff communication, or inadequate cabin planning can undermine the very advantage the device is supposed to provide.
How OCS Warm Perfusion Outperforms Cold Storage
At 2 a.m., the difference between cold storage and warm perfusion shows up fast. The recovery team is leaving the donor hospital, the receiving OR is adjusting timing, weather is starting to shift, and every handoff matters. In that setting, cold storage gives the transport team less room to absorb delays. OCS gives the clinical team more visibility and, in many cases, more usable time.
Cold storage still works, and it remains common for good reasons. It is simpler to set up, easier to transport, and familiar to donor and recipient hospitals. For a short, clean route with minimal handoff risk, that simplicity can be an advantage.
The trade-off is limited insight during transit.
With static cold storage, the organ is cooled and metabolism is reduced, but the team cannot evaluate it in the same active way while it is moving. If the mission runs long because of aircraft repositioning, ground congestion, or a delayed departure from the donor site, the tolerance for disruption shrinks. A case manager may only hear that the flight is delayed by 40 minutes. Clinically, that same delay can force a harder conversation at the receiving center.
Warm perfusion changes that operating picture. The OCS Heart maintains the organ in a near-normothermic state with oxygenated donor blood, which allows ongoing perfusion and assessment during transport, as described in this clinical overview of the OCS Heart platform.
For transport coordination, that matters because the mission is no longer built around a cooler and a countdown alone. It is built around preserving function while the organ is in motion. The aircraft plan, loading sequence, cabin layout, power planning, and handoff timing all need to support an active preservation process.
What cold storage does well, and where it falls short
Cold storage has clear operational advantages. It is lighter, less equipment-intensive, and easier to move through hospitals, ramps, and ambulance transfers. Teams can execute it with fewer moving parts.
Its weakness is exposure to uncertainty. There is less ability to assess organ condition during the trip, and less flexibility when the schedule stops being ideal. In air medical work, that is not a theoretical problem. Delays happen on the ground more often than people expect, and they often happen at the worst point in the chain, after recovery and before wheels up.
How warm perfusion changes the mission
Warm perfusion gives the transplant team more than preservation. It gives them data during the transport interval and a better chance to manage longer or more complex routes with intention.
That does not make OCS easier.
It makes the mission more demanding in a different way. The device adds weight, space requirements, setup considerations, and a stricter need for experienced coordination. Crews need a secure loading plan. Ground teams need disciplined handoffs. The receiving hospital needs accurate arrival updates because OCS supports the organ during transport, but it does not remove the need for synchronized OR readiness.
Side by side comparison
Organ Preservation Methods Compared: Cold Storage vs. Organ Care System (OCS)
| Feature | Traditional Cold Storage | Organ Care System (Warm Perfusion) |
|---|---|---|
| Preservation approach | Static cold storage | Active warm perfusion |
| Organ state during transport | Metabolically suppressed | Closer to physiologic state |
| Assessment during transit | Limited | Real-time physiologic assessment |
| Response to longer transport | Narrower margin | Better suited to extended transport planning |
| Equipment complexity | Lower | Higher |
| Staffing and coordination burden | Lower | Higher |
What works and what doesn't
Successful OCS transport depends on disciplined execution. The clinical benefit is tied to operations. If the donor hospital handoff is disorganized, the ambulance crew is not briefed on device handling, or the aircraft cabin is not configured before arrival, the mission becomes harder than it needs to be.
I tell case managers to watch three points closely. Confirm who is responsible for the device at each handoff. Confirm how the aircraft will secure and position the system. Confirm that recipient-side timing is being updated in real time, not assumed from the original schedule.
A common planning mistake is focusing on airborne time and underestimating ground time. The higher-risk interval is often the period between organ recovery and departure, when teams are transferring custody, loading equipment, and solving last-minute access problems.
For families, this can sound technical. In practice, the distinction is simple. Cold storage is a race against a tighter clock. OCS supports the organ in a more active state while the transport team works through the realities of distance, weather, handoffs, and hospital timing.
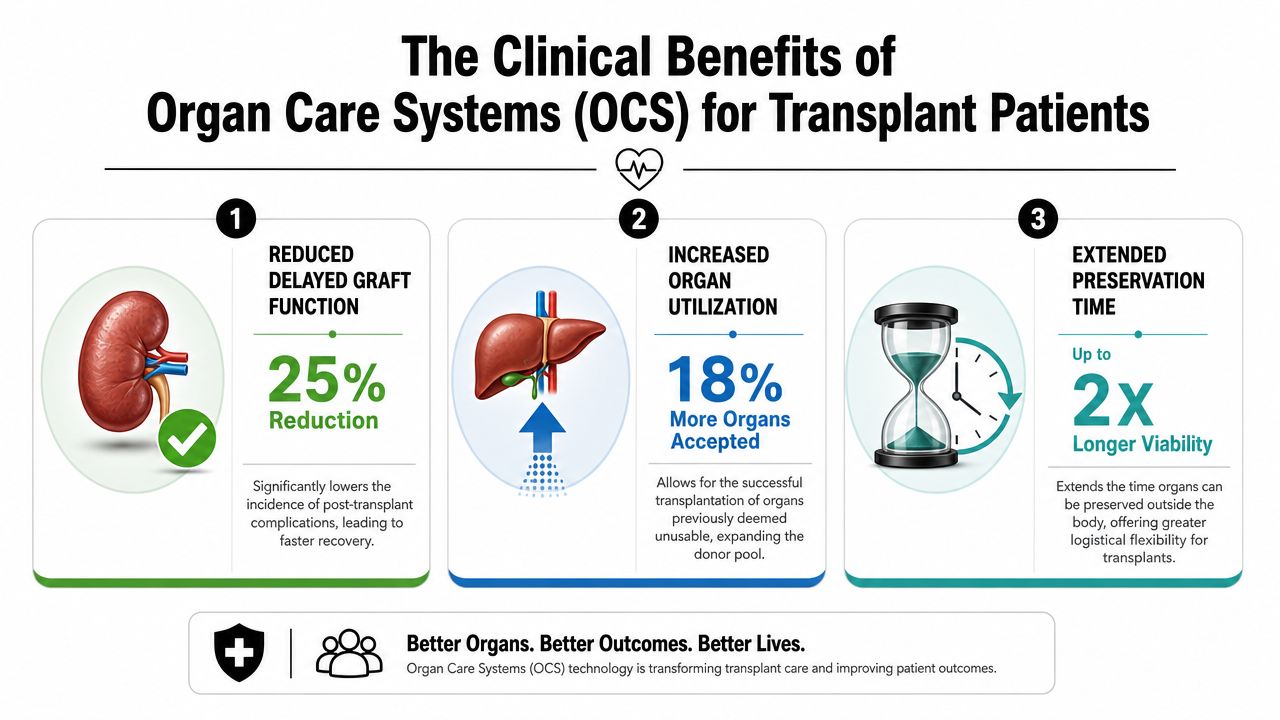
The Clinical Benefits of OCS for Transplant Patients
A case manager usually sees the clinical value of OCS at the same moment the logistics become more demanding. The donor hospital is ready, the recipient team is watching the clock, weather may narrow the flight options, and the transplant surgeons still want enough information to decide with confidence. OCS helps on the clinical side because it can preserve organ function in a more active state and give the team more data before implantation.
An Organ Care System matters to transplant recipients for three practical reasons. It can expand access to organs that may have been declined under tighter preservation limits, support better organ assessment before implant, and improve early graft performance in selected cases.
Better outcomes that matter at the bedside
The core question is simple. Does OCS give the transplant team a better chance to deliver a functioning organ to the recipient under workable conditions?
In selected heart transplant settings, published clinical literature has linked OCS use with strong survival and lower rates of severe early graft dysfunction. Rather than repeat the same source cited earlier, the practical takeaway is this: teams use OCS because the benefit can extend past transport and into the first hours and days after implant, when graft performance drives ICU course, mechanical support needs, and recovery planning.
That distinction matters to hospital staff. If the organ functions well early, the downstream effect can include fewer emergency interventions, a more predictable postoperative course, and clearer communication with families.
From the transport side, that is why medical organ transport planning for transplant teams and families cannot be treated as a shipping exercise. The clinical goal and the flight plan are tied together.
Why pre-implant assessment changes decisions
OCS gives the transplant team a chance to evaluate the organ during preservation instead of relying only on retrieval findings and ischemic time. That added visibility can influence whether the organ is accepted, how the recipient team prepares, and how much risk the surgeons believe is reasonable.
I explain it this way to case managers. OCS does not remove risk. It gives clinicians a better basis for judgment while the organ is still in transit and while the recipient hospital is making time-sensitive decisions.
That is most useful in cases with longer distance, more complex donor characteristics, or a narrower margin for error in the recipient. The technology can support acceptance of an organ that might otherwise be passed over because the team has more than a static snapshot.
A useful explainer for families and care teams is below.
Questions families and case managers ask
- Does OCS guarantee a successful transplant? No. Recipient condition, donor factors, surgical execution, and timing still affect the outcome.
- Can it make more organs usable? Yes, in some cases. That is one reason transplant programs accept the extra staffing, equipment, and coordination burden.
- Is the benefit only about longer travel distance? No. The added value is also the ability to assess the organ during preservation and make a more informed implant decision.
- Does every center run OCS cases the same way? No. Programs differ in procurement workflows, staffing depth, device familiarity, and flight coordination standards.
- Why does aircraft planning matter if the system is already preserving the organ? Because the device still has to be secured, powered, monitored, and handed off without delay. Hospitals that are understanding aircraft operational models tend to ask better questions about readiness, control, and transport responsibility.
A well-run OCS mission reduces avoidable uncertainty. For families, that usually means the team has more information and more options. For case managers, it means tighter coordination between the transplant service, procurement team, and air medical operator so the clinical promise of the technology is not lost during transport.
Navigating the Regulatory and Practical Landscape
The regulatory picture matters because it tells hospitals what the technology is cleared to do. The practical picture matters because it tells them what it takes to do it well.
The FDA expanded the indication for the OCS Heart System to include donation-after-circulatory-death donor hearts, and in the supporting study 94 of 100 DCD-heart recipients were alive at 6 months versus 91 of 100 recipients of DBD hearts preserved with standard cold storage, according to the FDA announcement on the OCS Heart indication expansion.
Why the DCD expansion matters
For transplant teams, DCD heart use is not a minor administrative update. It broadens the donor pathway. That can create opportunities for patients who might otherwise wait longer or miss an offer entirely.
But regulatory expansion is the easy part compared with implementation. Once a hospital chooses to pursue OCS-supported cases, the burden shifts to staffing, training, on-call readiness, procurement coordination, airport access, and device-specific transport planning.
The trade-offs hospitals really face
At this point, the conversation often gets more honest.
OCS is promising, but it isn't operationally simple. Hospitals still have to answer difficult questions:
- Which patients benefit most from the added complexity?
- Which organ types and donor scenarios justify the overhead?
- Can the center support the staffing model needed for these missions?
- How will reimbursement and internal cost review be handled?
- What happens after hours, when donor recovery, airport movement, and recipient preparation all tighten at once?
A separate concern is fairness. Broader transplant-system discussion has highlighted ongoing equity and cost-effectiveness challenges in organ allocation. OCS can extend out-of-body time to at least 8 hours and enable longer-distance procurement, but its benefits may be uneven if the centers with the infrastructure are clustered in major hubs, as discussed in this review of organ preservation and allocation challenges.
That's a real issue. Advanced preservation can widen opportunity, but if access to procurement teams, transport resources, and reimbursement support is uneven, it can also concentrate advantage.
Why aviation details also matter
Case managers sometimes underestimate how much the aircraft side affects organ transport reliability. Not every operator structure, dispatch model, or flight readiness standard is the same. A useful primer for non-aviation teams is understanding aircraft operational models, because the way an aircraft is operated can affect oversight, crew readiness, and mission planning assumptions.
For hospitals trying to organize these cases, specialized medical organ transport coordination becomes less about convenience and more about reducing points of failure.
Decision point: The hardest question isn't whether OCS works. It's where the incremental clinical benefit outweighs the operational burden.
That's the right way to frame it. Not every case needs OCS. But when a center decides the clinical upside is worth it, the transport plan has to match the seriousness of that choice.
Coordinating Air Transport for OCS A Checklist
When an Organ Care System is part of the mission, air transport coordination has to be exact. Timing drift, incomplete paperwork, weak handoffs, or a crew unfamiliar with the device can create avoidable risk.
This is the checklist I'd want a case manager to work from before the aircraft is dispatched.
Confirm the clinical plan first
Before anyone talks about departure time, confirm the basics with the transplant and procurement teams.
Verify the organ and device match
Confirm which organ is moving, which OCS configuration is in use, and who is responsible for perfusion management.Identify the clinical decision-maker
One physician or designated clinical lead should be the final authority for go, hold, or change decisions during transport.Clarify the acceptance pathway
Know whether the organ is fully accepted, conditionally accepted, or still under active assessment.
If this part is vague, the aviation piece won't fix it.
Build the transport timeline around handoffs
A good OCS mission is a chain of controlled transitions.
- Donor hospital release point
Who physically brings the device and organ from the recovery area to the transport team? - Ground-to-airport move
Who manages vehicle loading, security access, and tarmac timing? - Aircraft loading sequence
Who supervises secure placement, power awareness, and cabin access? - Arrival handoff
Who receives the organ at the destination and how quickly can the team move from aircraft to hospital?
When a family has multiple people trying to reach the airport or recipient center, separate logistics may be needed. In those situations, planners sometimes look at services like Max's Luxury Rides for group travel for non-clinical ground movement, so the medical team can stay focused on the organ mission itself.
Documentation and communication checklist
The transport provider should know exactly what documents and communication points are required before departure.
- Medical documentation
Include donor and recipient transport-related paperwork required by the transplant process and the transport handoff. - Device responsibility
Identify who travels with the OCS and who is authorized to manage it. - Contact tree
List direct phone numbers for donor OR contact, procurement lead, flight operations, receiving transplant coordinator, and destination receiving team. - Airport access details
Confirm FBO or airport handling arrangements, security procedures, and after-hours access points. - Contingency protocol
Decide in advance who gets called first if there's a delay, reroute, weather issue, or recipient-side timing change.
Missed communication hurts these missions faster than bad weather does.
Questions to ask the air transport provider
Not every provider is built for this kind of case. Ask direct questions.
| Question | Why it matters |
|---|---|
| Have you transported organs with an OCS on board before? | Experience reduces handling mistakes |
| Who coordinates the airport handoffs? | Ground delays often create the biggest problems |
| How is the device secured in the cabin? | Stability matters during all phases of flight |
| Who is the primary operations contact during the mission? | Case managers need one reliable control point |
| What happens if departure timing changes at the donor site? | Flexibility is critical in transplant work |
A specialized organ recovery transport team should be able to answer those questions clearly, without vague promises or generic charter language.
What families need to hear
Families don't need every technical detail. They need clarity.
Tell them who is coordinating the move, how updates will be communicated, and what parts of the process may still change. OCS-supported transport improves options, but it doesn't make transplant logistics simple. Honest expectations usually reduce panic better than over-reassurance.
If you're arranging an organ or transplant-related medical flight and need experienced coordination, Med Jets by Air Trek can help guide the process from first call through arrival.