A hospital doctor says your loved one is stable enough to move, but not safe to travel on a commercial flight. The receiving hospital has a bed. The air ambulance team is ready to coordinate. Then someone says, “We still need prior authorization.”
That's the moment many families freeze. They hear a term that sounds administrative, but the situation feels urgent, emotional, and very personal. Case managers feel it too. Everyone knows the transfer matters, but nobody wants to guess who's responsible for the insurance piece or risk a delay caused by missing paperwork.
That confusion isn't just your impression. The AMA says payers often leave patients and physicians in the dark about approval criteria and denial reasons, which helps explain why prior authorization feels so opaque when families first run into it in a crisis AMA on fixing prior auth transparency.
Air ambulance transport raises the stakes because the clinical need is serious, the coordination is complex, and the paperwork has to match the medical story precisely. Families are often trying to process ICU updates, speak with nurses, answer insurer questions, and decide whether they can travel with the patient, all at the same time.
If you're in that position now, take a breath. Prior authorization is frustrating, but it's not random. Once you understand who submits what, what the insurer is reviewing, and how to document medical necessity for a flight, the process becomes more manageable.
Your Guide to Navigating Medical Flight Approvals
A daughter gets a call that her father needs transfer to a specialty center in another state. The sending hospital says ground transport would take too long and the clinical team is recommending air medical transport. She assumes the medical decision is the hard part. Then the insurer asks for authorization, clinical records, and details about why this specific level of transport is necessary.
That's a common turning point. Families think they're waiting for a plane, when in fact they're waiting for a documentation packet, a reviewer decision, or a callback between hospital staff and the plan.
Why this feels harder than it should
Air ambulance prior authorization combines two stressful systems at once. One is clinical. Is the patient stable enough to move, and what support is needed during the flight? The other is administrative. Does the insurer agree that this transfer meets the plan's rules for coverage?
The family usually sits in the middle, hearing partial updates from multiple people. A nurse may focus on care. A case manager may focus on placement and records. The insurer may focus on policy language. The air ambulance coordinator may focus on logistics and bedside-to-bedside timing.
Prior authorization often feels like a moving target because each party sees only one piece of the transfer.
What families usually want to know right away
Many individuals ask some version of the same questions:
Who is supposed to request approval
Usually the treating team or hospital staff starts the process, but the transport provider may need to add flight-specific clinical details.Can the flight be arranged before approval
Coordination can begin, but coverage decisions usually depend on the insurer's review.What if the patient needs transfer quickly
The case should be framed with urgency and supported by clear clinical documentation.If we get denied, is that final
Not always. Denials can sometimes be appealed or revised with stronger documentation.
Families don't need more jargon. They need a map, a checklist, and language they can use on the phone. That's what the rest of this guide is built to provide.
What Is Prior Authorization in Healthcare
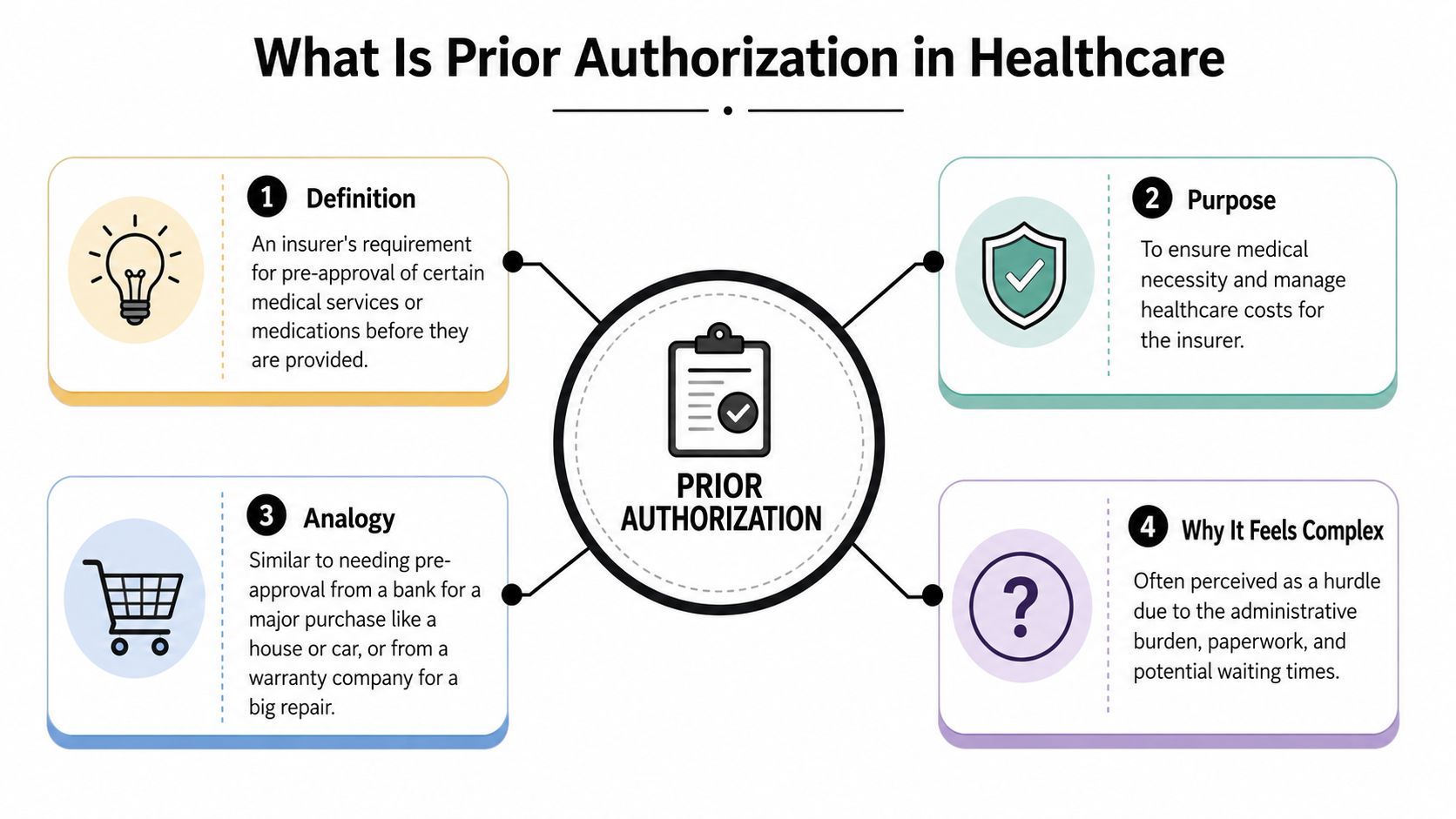
Prior authorization means the insurer wants advance approval before paying for certain services. A simple way to think about it is a permission slip tied to coverage. The doctor can order the service, but the plan may still require its own review before it agrees to pay.
The basic idea
Insurers use prior authorization for services they consider high-cost, high-risk, or sensitive to overuse. In plain terms, they're asking two questions:
- Is this medically necessary?
- Does it fit the plan's coverage rules?
That doesn't mean the service is inappropriate. It means the insurer wants documentation before the care is delivered or before the claim is paid.
A broader overview of prior authorization for healthcare practices can help if you want the office-side view of how teams handle these requests day to day.
Why air ambulance transport often triggers it
Air medical transport isn't a routine benefit in the way a standard office visit is. It's expensive, clinically complex, and highly specific to the patient's condition. For that reason, flights often draw close review around medical necessity, the level of care required during transport, and whether a safer or lower-cost alternative was available.
Prior authorization is also widespread across U.S. healthcare. A 2019 analysis found that 72.6% of Medicare Advantage enrollees were in plans requiring prior authorization for at least one service, and 72.2% of plans required it for durable medical equipment, a category that reflects similar cost sensitivity to medical transport AJMC analysis of prior authorization in Medicare Advantage.
A useful way to frame it
Think of prior authorization as a review of the request, not a judgment of the patient's worthiness. For an air ambulance case, the insurer is typically looking for a clear answer to questions like these:
- Why this patient
- Why this destination
- Why this level of transport
- Why now
Practical rule: If the chart says the patient needs a medical flight, but the submission doesn't explain why ground transport or another option won't work, the insurer may treat it as an incomplete case rather than an obvious one.
That distinction matters. Many families assume the urgency is self-evident. In prior authorization, urgency has to be documented in a way the payer can review.
The Prior Authorization Workflow for Medical Flights
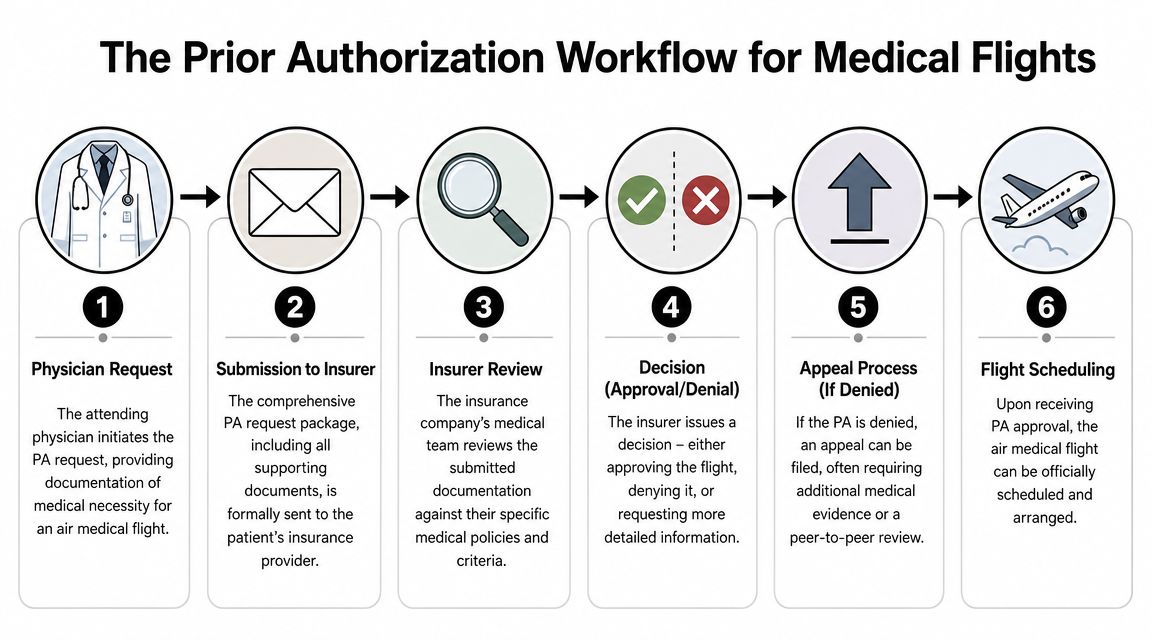
The workflow for a medical flight is easier to follow when you stop thinking of it as one big approval and start seeing it as a chain of handoffs. Each person has a role. Delays usually happen where one handoff is incomplete.
Who starts the request
The attending physician or hospital team identifies the need for transfer. In a flight case, that usually means the sending facility believes the patient requires care at another hospital and that air transport matches the patient's condition and timing needs.
The hospital case manager or discharge planner often becomes the operational lead. That person gathers insurance information, confirms the receiving facility can accept the patient, and helps assemble records.
The family still matters at this stage. Families often provide insurance cards, patient identifiers, consent information, travel preferences, and key history when records are scattered across systems.
What gets submitted
The request sent to the insurer usually includes the physician order, supporting chart notes, diagnosis information, and the transfer rationale. For an air ambulance, the transport team may also need to document why a medical flight is appropriate for this patient's condition and what level of onboard care is required.
An air ambulance coordinator may also help the family understand bedside-to-bedside logistics, such as airport transfer timing and whether a companion can travel. If you're comparing transfer options, this overview of return medical flight coordination shows how a transport provider may handle the larger movement plan around the patient.
What the insurer reviews
The payer's reviewers compare the packet to the plan's criteria. That's why two things can be true at once: the doctor can strongly support the transfer, and the insurer can still ask for more information.
The review may focus on:
Clinical necessity
Why the transfer is needed medically, not just logistically.Transport level
Why air ambulance is appropriate instead of ground or another mode.Destination support
Whether the receiving facility is identified and ready to accept the patient.Documentation completeness
Whether the submission includes the records required by that plan.
The three possible outcomes
Most requests land in one of three buckets:
Approved
The flight can move forward under the terms of the authorization.Pended or requesting more information
The insurer hasn't denied the case, but wants additional details before deciding.Denied
The insurer says the current submission doesn't meet its criteria.
When you hear “we need more information,” don't treat that as a small technicality. It often means the reviewer couldn't connect the records to the policy standard.
Where electronic prior auth is changing things
A meaningful operational shift is happening through the FHIR-based Prior Authorization API, also called the PARDD API. It's designed to automate requirements discovery, documentation guidance, and structured decision responses, so providers can query what needs authorization, see what data the payer wants, and receive a machine-readable decision instead of relying only on phone, fax, or unstructured back-and-forth FHIR Prior Authorization API overview.
That won't erase the need for strong documentation, but it can reduce ambiguity about missing elements and denial reasons.
Essential Documentation for a Successful Submission
For medical flights, prior authorization is often won or lost on the packet. The insurer isn't standing in the ICU. The reviewer sees only what the records show. If the paperwork leaves gaps, the payer may assume the medical case is weaker than it really is.
Published guidance on prior authorization workflow emphasizes that this is often a documentation-quality problem. Insurers may require diagnosis codes, chart notes, prior treatment failures, lab data, allergies, and proof of medical necessity. Strong submissions match the packet to the payer's criteria rather than stating that the service was ordered IHS prior authorization best practices PDF.
The documents that usually matter most
Use this as a working checklist for an air ambulance submission:
Physician order for transfer
This confirms the treating clinician is ordering the move, not just discussing it.Letter or statement of medical necessity
This should explain why the patient needs transfer, why the destination is appropriate, and why the chosen transport level is required.Recent clinical notes
Progress notes, consult notes, and nursing summaries help the insurer understand the patient's current status.Diagnosis and coding details
The payer may look for specific diagnosis information that ties the transport to a covered medical need.Medication list and current interventions
Ventilator support, drips, oxygen needs, monitoring requirements, and other active treatment details can justify the acuity of transport.Lab or imaging summaries when relevant
Not every case needs every result, but key findings can support urgency and medical complexity.Receiving facility acceptance
A confirmed accepting physician or bed supports the legitimacy and purpose of the transfer.
Why families should help organize records
Families can't usually write the medical justification, but they can reduce delay by keeping records and contact points organized. When the patient has had recent care at multiple facilities, fragmented records can slow the packet.
A practical tool for that side of the process is medical records sharing for families, especially when relatives are coordinating from different cities and need one place to track documents, updates, and permissions.
A complete packet doesn't just prove the patient is sick. It proves why this transport, at this time, is the covered and appropriate response.
How to tighten the packet before it goes out
Before submission, someone on the team should verify:
- Dates match across notes, orders, and transfer requests.
- The clinical story is consistent from physician order through transport rationale.
- The destination is named clearly, including accepting provider or facility details.
- The level of transport is explained, not assumed.
- Attachments are legible and current, especially if records were faxed or scanned.
If you're reviewing paperwork with a transport coordinator, a reference like medical documentation standards for patient transfers can help clarify what complete transport documentation generally looks like.
Common Denial Reasons and How to Avoid Them
Denials often feel arbitrary, but many come from predictable weaknesses in the request. That's one reason preparation matters so much. Physicians in an AMA survey reported 13 hours of staff time weekly spent on prior authorization, and 95% reported treatment delays when prior authorization is required prior authorization statistics summary.
Prior Authorization Denial Reasons and Prevention
| Denial Reason | What It Means | How to Prevent It |
|---|---|---|
| Not medically necessary | The payer doesn't think the records prove the flight meets its clinical standard | Ask the physician to explain the patient's current condition, why transfer is needed, why the destination is appropriate, and why this transport level is required |
| Incomplete or missing documentation | The packet lacks notes, coding, orders, or supporting records the reviewer expected | Use a checklist before submission and confirm that every attachment is included and readable |
| Level of care not justified | The insurer may agree a transfer is needed but not accept air ambulance as the necessary mode | Include details about monitoring, oxygen, drips, mobility limits, time sensitivity, or safety concerns that make lower-acuity transport inappropriate |
| Out-of-network concerns | The transport provider or receiving arrangements may trigger plan network questions | Verify network status early and ask the plan what documentation is needed if the clinically appropriate option is outside network |
| Destination not clearly supported | The insurer doesn't see a documented reason for that receiving facility | Include accepting physician or facility information and the clinical reason the patient must go there |
| Administrative mismatch | Names, policy numbers, dates, or identifiers don't line up | Double-check demographics, insurance details, and submission references before anything is sent |
Prevention starts before the denial
The safest approach is to assume the reviewer knows nothing beyond what's in the packet. If the transport need seems obvious to bedside staff, write it anyway. If the timeline matters, document why. If the receiving hospital offers a service the sending hospital can't provide, say that clearly.
For families trying to understand the financial side while reviewing these risks, this guide to whether insurance covers air ambulance transport can help frame the coverage questions that often arise alongside authorization.
Templates and Scripts for Families and Case Managers
When people are stressed, they often know what they want to ask but can't find the words in the moment. A short script helps keep the call focused and creates a record you can use later.
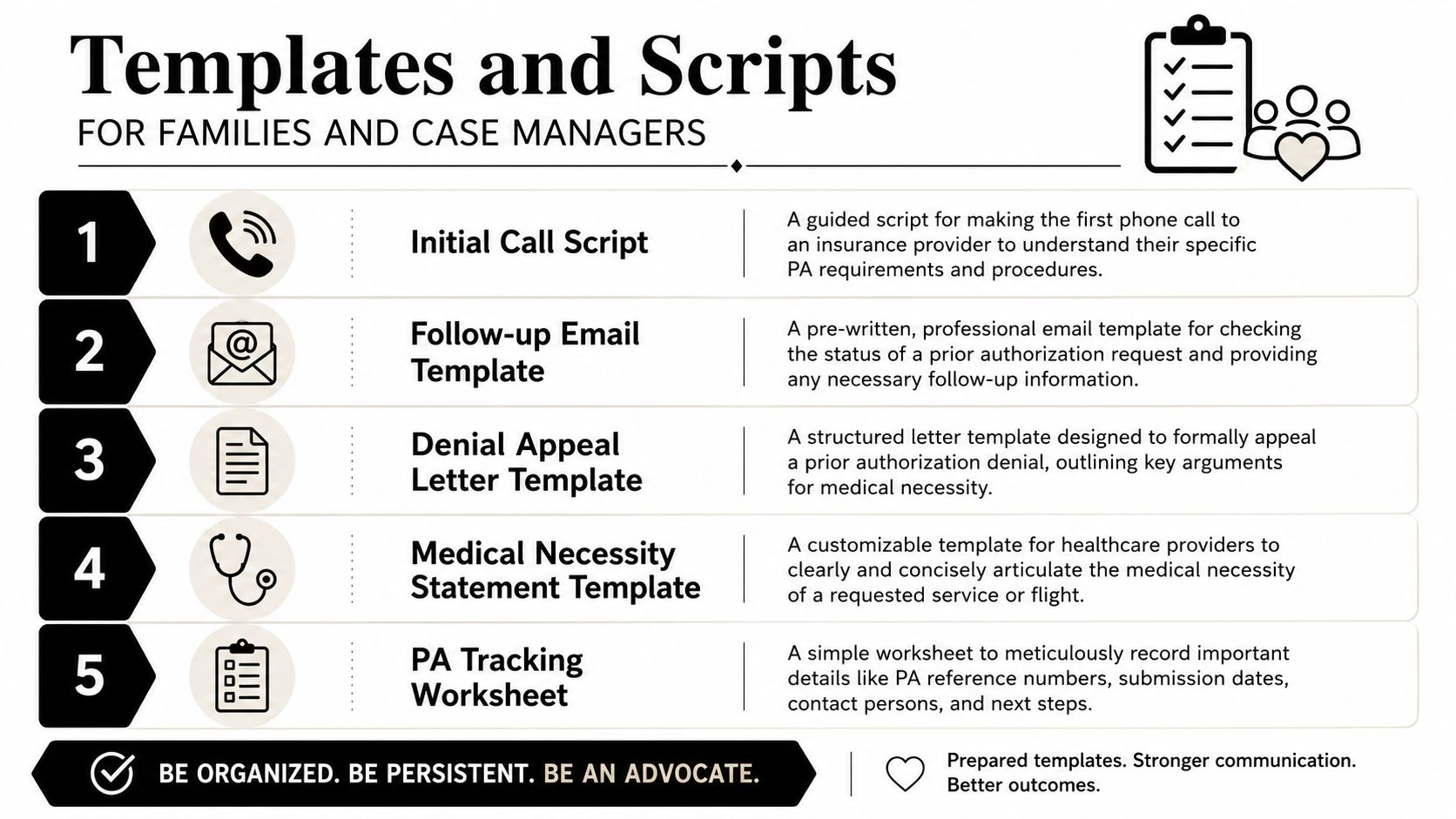
Initial call script to the insurer
Use this when you need to confirm the process, not debate the case.
“I'm calling about a hospital-to-hospital transfer for a patient who may need air ambulance transport. I want to confirm whether prior authorization is required under this plan, who must submit the request, what clinical documents are required, and whether this case can be reviewed as urgent. Please give me the reference number for this call, your name, and the fax or portal details for submission.”
If the representative sounds vague, add this:
“Please tell me the specific documentation categories required for review, including any physician statement, accepting facility information, or transport-level criteria.”
Follow-up email to a case manager
You can send this after the hospital says the request is in progress.
Subject: Prior Authorization Status for Air Medical Transfer
Hello [Name],
I'm following up on the prior authorization request for [Patient Name]. Can you confirm whether the request has been submitted, the date and time it was sent, the insurer reference number, and whether any additional records are still needed from the family or treating team? If the insurer has asked for more information, please let me know exactly what is missing so we can help gather it quickly.Thank you,
[Your Name]
[Relationship / Contact Information]
Questions to ask the transport provider
Don't just ask, “Do you take insurance?” Ask operational questions.
Who handles insurer communication
“Will your team submit flight-specific clinical information if the hospital starts the authorization?”What documents do you need from the hospital
“Do you need a physician order, accepting facility details, and recent notes before you can finalize the mission?”How do you track status
“Who will call us with updates if the insurer requests more information?”How do you support the paperwork
One option families consider is Med Jets by Air Trek, which coordinates medical transport and documentation support as part of transfer planning.
Simple tracking worksheet fields
Keep one running note with these fields:
- Patient identifiers
- Insurance plan and member ID
- Date submitted
- Who submitted it
- Authorization or reference number
- Insurer contact name
- What documents were sent
- What's still missing
- Next follow-up time
That worksheet can matter as much as the appeal letter. In understanding prior authorization, clean tracking often prevents duplicate confusion and missed callbacks.
Your Next Step to a Smooth and Safe Transfer
By the time a family hears the words “prior authorization,” they're usually already managing a lot. They're talking with doctors, updating relatives, weighing travel plans, and trying to make decisions fast. What helps most is narrowing the task into three practical goals: get the medical story documented clearly, confirm who owns each handoff, and keep a written record of every insurer contact.
That approach won't make the process pleasant, but it does make it more controllable. It also reduces the chance that a flight is delayed because one document, one phone note, or one unanswered payer question fell through the cracks.
This is the kind of transfer where experienced coordination matters. A flight isn't only an aircraft issue. It's a records issue, a coverage issue, a timing issue, and a receiving-facility issue all at once.

If you're arranging a transfer now and need help sorting the approval and transport steps, a direct call is often the fastest next move. You can reach the coordination team through Med Jets by Air Trek or call 1-800-MED-JETS for 24/7 assistance.
The goal isn't just getting an answer from insurance. It's getting your loved one moved safely, with fewer surprises, and with someone keeping the paperwork aligned to the medical need.