When a parent needs to get from one hospital to another, or a discharge planner mentions air ambulance involvement, the question isn't abstract travel. It's a very practical one: What is ground transportation, and how does it work when someone is sick, injured, fragile, or unable to travel in a regular car?
That confusion is common. Many people hear “ground transportation” and think of airport shuttles, taxis, or a ride home from baggage claim. In medical care, it means much more. It can be the vehicle that gets a patient safely from a bedside to an airport, from an airport to a receiving hospital, or across town for treatment when flying isn't needed.
The simplest definition is this: ground transportation is the movement of people or goods over land. In healthcare, that land-based movement becomes part of a larger care chain. It includes wheelchair vans, stretcher vehicles, non-emergency medical transport, and fully staffed ambulances. When air ambulance service is involved, ground transport is often the first and last step that makes the whole transfer possible.
Understanding Ground Transportation Beyond the Airport
A family may hear that a patient is flying by air ambulance and assume the plane is the hard part. In practice, the trip often depends just as much on what happens on the ground. Someone still has to get the patient from the hospital room to the aircraft, then from the arrival airport to the receiving facility, with the right equipment, timing, and clinical support in place.
That is why the usual travel definition of ground transportation is too limited for medical planning. In general use, the term covers land-based travel such as buses, trains, rideshares, rental cars, vans, and other road or rail services. In healthcare, that same idea expands into a care function. The vehicle is only one piece. The transfer also includes patient handling, medical equipment, communication between teams, and safe handoffs at each stop.
A simple way to frame it is this: ground transportation in medicine works like the connecting corridors in a hospital. The corridors are not the surgery, the ICU, or the imaging suite, but nothing reaches the right place without them. Ground transport plays the same role in the medical transport chain. It connects bedside, ambulance bay, airport, aircraft, and receiving unit in the correct order.
Why the term sounds simpler than the real process
The phrase can sound ordinary because many land trips are ordinary. A healthy traveler can step into a car and go.
A medically fragile patient may need a very different setup. The team may have to account for oxygen, stretcher loading, fall risk, isolation precautions, pain control, cardiac monitoring, or help with transfers in and out of bed. A missed detail at the ground stage can disrupt the entire itinerary, even if the flight itself is perfectly arranged.
For families and new case managers, it helps to stop picturing ground transport as a ride and start viewing it as a controlled handoff. The main question is not only where the patient is going. The main question is what has to stay stable during the trip.
Practical rule: If the patient cannot safely travel in a regular car without added help, the ground portion should be planned like part of the care plan, not treated as basic transportation.
Where confusion usually starts
Several terms get grouped together, even though they do different jobs:
- “Does ground transportation only mean an ambulance?” No. It can include wheelchair vans, stretcher vans, non-emergency medical vehicles, and ambulances with different staffing levels.
- “Is ground transport still part of the plan if the patient is flying?” Yes. Air ambulance transport rarely starts and ends at the runway. Ground crews usually handle the first leg, the final leg, or both.
- “Why does the land portion get so much attention?” Because many risks show up there first. Entry routes, lift access, bed transfers, oxygen supply, and timing with hospital staff all have to line up.
This broader medical view is important because patients do not move through the system the way travelers move through a vacation itinerary. They move through a chain of care. Ground transportation keeps that chain intact from one clinical setting to the next, including the parts before and after an air ambulance flight.
The Core Components of Ground Transport Systems
A strong transport plan doesn't start with a vehicle. It starts with coordination.
In technical logistics, ground transportation is defined as the coordinated movement of personnel and equipment by road-based vehicles, handled as a controlled system with dispatch, planning, operations analysis, licensing, and cost considerations, based on the U.S. Air Force ground transportation training framework. That definition comes from a military setting, but the structure is useful in civilian medical transport too.
Five parts that make the system work
When a transport coordinator looks at a case, these are usually the moving pieces:
Vehicles
The vehicle has to match the patient's condition. A wheelchair van, stretcher van, BLS ambulance, and ALS ambulance all solve different problems.Infrastructure
Roads, airport access points, receiving entrances, elevators, loading zones, and hospital handoff locations all affect the route.Personnel
Drivers, EMTs, paramedics, nurses, dispatchers, and hospital staff each have distinct roles. One weak handoff can delay the whole chain.Technology
Dispatch software, GPS, call logs, mobile communication, and real-time updates keep the plan synchronized.Regulations and processes
Licensing, driver qualifications, patient documentation, infection-control procedures, and clinical protocols shape what can happen and who can do it.
Three broad categories people often mix together
To keep the term clear, it helps to sort ground transportation into three buckets.
Public ground transportation
This system is commonly understood. Buses, rail, subway lines, and public shuttles move large numbers of people over land. These options are important for everyday mobility, but they usually aren't suitable for patients who need hands-on assistance or onboard medical support.
Commercial personal transportation
This bucket includes taxis, ride-shares, rental cars, hotel shuttles, and private car services. They can work for medically stable travelers who can sit upright, transfer independently, and travel without clinical monitoring.
Medical ground transportation
This is the category families and case managers usually need when health status changes the travel plan. It includes ambulances, stretcher transport, wheelchair transport, and specialized transfer vehicles.
A useful test is simple. If the trip requires medical judgment, mobility equipment, or a supervised handoff, you're no longer dealing with ordinary passenger transport.
Types of Medical Ground Transportation Explained
Not every patient needs the same kind of vehicle, and choosing too little support can create risk. Choosing too much can add cost and complexity that isn't necessary. The safest approach is to match the transport type to the patient's mobility, medical stability, and level of monitoring needed during the trip.
The main types families and case managers see
Some transports are urgent. Others are carefully scheduled. Some require clinical staff. Others focus mainly on safe mobility and transfer assistance.
| Medical Ground Transport Comparison | |||
|---|---|---|---|
| Transport Type | Typical Use Case | Onboard Staff | Best For |
| Wheelchair-accessible vehicle | Patient can sit upright but can't safely use a standard car seat | Driver, sometimes with mobility assistance depending on provider | Patients with limited walking ability who don't need clinical monitoring |
| Stretcher van | Patient must remain lying down but doesn't need active emergency care | Driver and sometimes attendant support, depending on service model | Stable patients who need flat transport for comfort or safety |
| Non-emergency medical transport | Scheduled trip to treatment, discharge destination, rehab, or appointment | Varies by provider and patient need | Patients who need arranged medical travel without emergency response |
| BLS ambulance | Transport with basic medical support and supervised patient handling | EMT-level crew | Patients who need ambulance-level transport but not advanced interventions |
| ALS ambulance | Higher-acuity transport with advanced assessment and interventions available | Paramedic-level crew, sometimes additional clinicians | Patients whose condition may change during transit or who need closer monitoring |
Wheelchair and ambulatory transport
This is often appropriate when the patient is medically stable but functionally limited. A person may be recovering from surgery, too weak to manage stairs safely, or dependent on a wheelchair for mobility.
Families sometimes assume this is “just a van.” It isn't. A proper wheelchair-accessible vehicle should fit the chair securely, allow safe boarding, and reduce the physical strain of transfers.
Stretcher transport
Stretcher vehicles fill an important middle ground. They help when the patient can't tolerate sitting for the full ride, can't transfer safely into a regular seat, or needs to remain reclined because of pain, weakness, or post-procedure restrictions.
This option is common in long-distance overland transfers when the patient needs positioning support but not full emergency care. If that's the situation you're dealing with, this overview of long-distance medical ground transportation gives a practical look at how those trips are arranged.
BLS and ALS ambulances
These are the two ambulance categories families hear most often, and they're easy to confuse.
BLS, or Basic Life Support, is typically used when a patient needs ambulance transport, safe handling, and basic monitoring, but not advanced interventions. A patient may be stable, on a predictable care plan, and still unable to ride in a personal vehicle.
ALS, or Advanced Life Support, is used when the patient's condition is more complex or may change during the trip. That can include a higher risk of deterioration, a need for advanced assessment, or medications and interventions that exceed basic ambulance scope.
How to think about the choice
Ask three questions first:
- Can the patient sit upright for the full trip?
- Does the patient need monitoring, oxygen, or clinical care en route?
- How risky would it be if the patient's condition changed during transport?
If the answers aren't clear, the sending facility, receiving team, and transport coordinator should work that out before the vehicle is booked.
Safety Regulations and Clinical Staffing Standards
Families usually want the same reassurance: Who will be with my loved one, and how do I know the trip will be safe?
That question matters because there are large safety differences across land travel modes. The National Safety Council reports that over the last 10 years, the death rate for passenger vehicles per 100,000,000 passenger miles was more than 70 times higher than for buses, according to the NSC transportation mode safety data. For medical transport planning, the takeaway isn't that every bus is a substitute for an ambulance. It's that mode, training, and system controls matter.
What safe and certified usually involves
A qualified medical transport service should be able to explain, in plain language, the basics of its operation.
Look for answers to these points:
Vehicle licensing
The vehicle should be authorized for the type of transport being performed.Crew credentials
You should know whether the trip is staffed by a driver, EMT, paramedic, nurse, or a mixed team.Clinical scope
Ask what the crew can do during the ride. Monitoring, oxygen management, suction, medication support, and emergency response are not interchangeable.Transfer capability
Safe transport includes getting the patient in and out of bed, onto the stretcher, through hallways, and into the receiving facility.
The staffing titles families hear most
The titles can sound similar, but they don't mean the same thing.
An EMT usually handles foundational emergency care and patient transport functions. A paramedic generally has a broader field scope and can manage more advanced clinical needs. A registered nurse may be added in more specialized transports where patient complexity calls for that level of assessment or treatment continuity.
If you want a simple primer for team preparation and transport competency, this page on patient transport training is helpful.
Ask the provider, “What level of clinician will be with the patient, and why is that level appropriate for this case?” A solid service should answer directly.
What safety looks like during the actual trip
Safety isn't only about certifications on paper. It's also about how the trip is run in real time.
That includes pre-trip communication, securing equipment, confirming medication and oxygen needs, route planning, monitoring during motion, and a structured handoff at arrival. Those details often matter more than families realize.
A short overview can make those standards easier to visualize:
Coordinating Ground and Air Ambulance Transfers
When an air ambulance is involved, ground transportation doesn't sit on the sidelines. It is part of the mission.
The phrase families often hear is bedside-to-bedside care. That means the patient isn't flown from airport to airport. The movement begins where the patient is, usually a hospital, rehab center, nursing facility, or home, and ends at the receiving facility. Ground teams and air teams have to work as one chain.
What the transfer looks like in real life
A typical case might start with a hospital case manager calling for a long-distance move. The patient needs to leave the current facility, reach the departure airport safely, transfer to the aircraft, then continue from the arrival airport to the receiving hospital.
None of those steps can be treated separately. If the sending floor isn't ready, the ground team waits. If airport access changes, the handoff timing shifts. If the receiving facility needs a revised arrival window, dispatch has to update both sides.
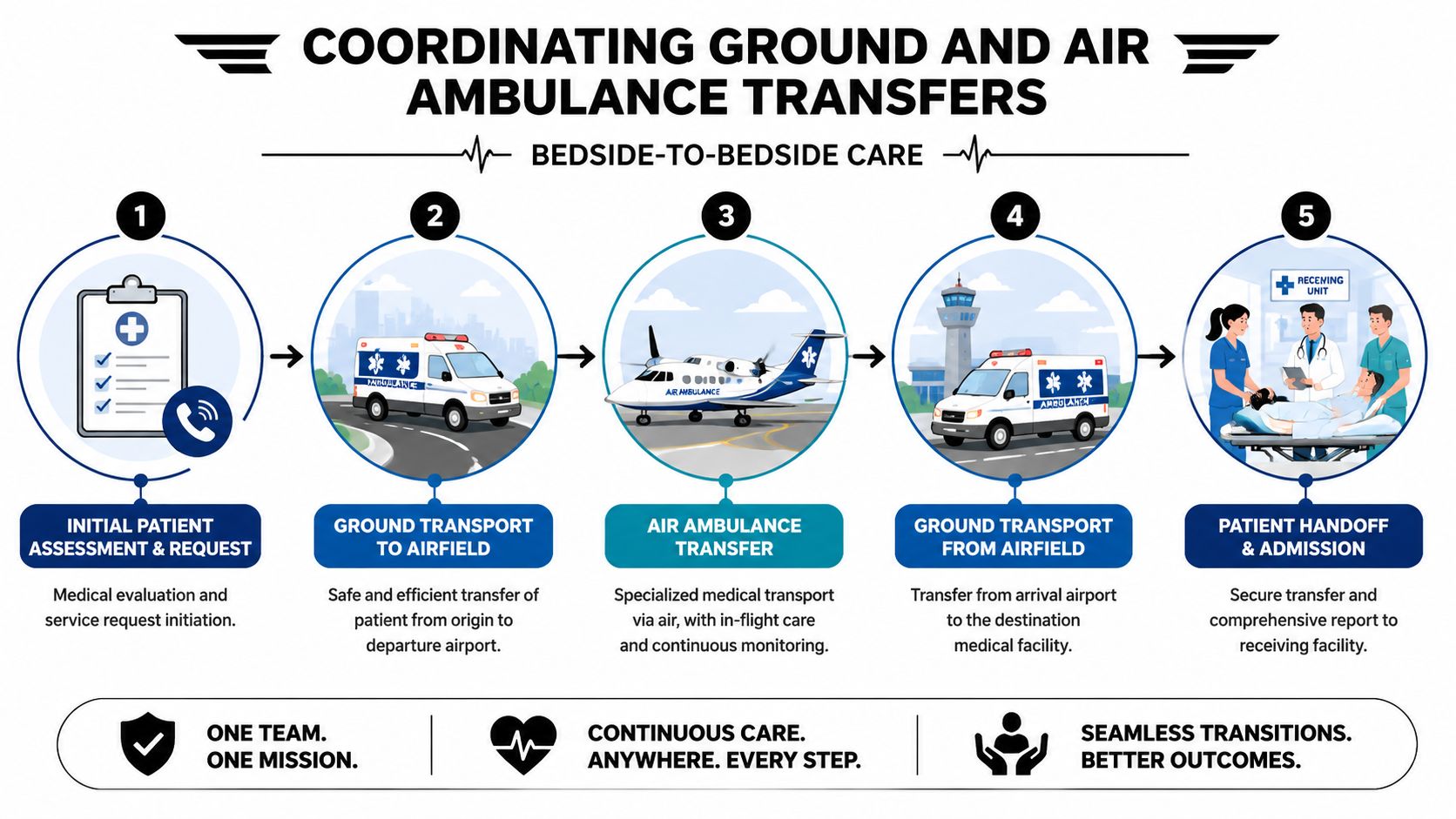
The five handoffs that have to stay aligned
Clinical acceptance
The sending and receiving teams confirm that the patient can travel and what support is needed during every segment.Origin pickup
The ground crew arrives with the right vehicle, transfer method, and staffing for the patient's condition.Airport transition
The patient is moved from ground ambulance to aircraft without losing continuity of care, equipment support, or documentation.Arrival-side pickup
A second ground team is positioned to meet the aircraft and continue the transfer.Receiving handoff
The crew gives report, transfers the patient safely, and closes the loop with the facility staff.
Why this coordination matters so much
Families sometimes focus on the flight because it's the most visible part. The risk points are often in the transitions.
A poorly planned tarmac handoff, a mismatch in stretcher height, missing paperwork, or a receiving delay can create stress for everyone involved. Good coordination prevents those avoidable problems.
Smooth medical transport usually depends less on speed alone and more on whether every handoff was planned before the wheels started moving.
For example, a provider such as Med Jets by Air Trek may coordinate the air segment together with the required ground legs so the family isn't left arranging separate pickup and drop-off services on their own. That's especially important when the patient needs continuous supervision instead of a simple airport transfer.
Navigating Payments and Choosing the Right Option
After the clinical questions come the practical ones. Who pays? What does insurance require? How do you choose between options when timing, comfort, and medical needs don't line up neatly?
The frustrating answer is that coverage varies. Some transports may require prior authorization. Some may be covered only under certain medical necessity standards. Some may involve private pay, partial reimbursement, or a combination of payer sources. For a plain-language starting point, this guide to medical transport insurance coverage can help you frame the conversation.
What to gather before you call
Have these details ready:
Patient condition
Current diagnosis, mobility level, oxygen use, isolation needs, and whether the patient can sit upright.Trip details
Pickup location, destination facility, preferred timing, and whether stairs or narrow entrances are involved.Clinical paperwork
Discharge summary, physician orders if applicable, medication list, and receiving facility contact information.Payment information
Insurance plan details, case manager contact, and whether pre-authorization has been requested.
How to compare options without getting lost
The cheapest option isn't always the right one. The fastest option isn't always the safest one either.
Use these filters:
Level of care needed
If the patient may decline during the trip, don't book a lower-acuity vehicle just because it's easier to arrange.Accessibility and transfer burden
Major airports maintain distinct ground transport options, including ADA-oriented shuttles and dedicated medical transport providers, as shown on the Salt Lake City airport ground transportation page. That matters because accessibility isn't an extra feature. It's part of whether the transfer can be completed safely.Continuity of care
Ask whether the same care plan follows the patient from origin to destination, especially if both ground and air are involved.
Questions worth asking every provider
- “What type of vehicle are you recommending, and why?”
- “Who will staff the transport?”
- “What equipment can travel with the patient?”
- “How are delays or condition changes handled?”
- “What portion may be billed to insurance, and what may be private pay?”
If you're involved in the billing or hospital side, it also helps to understand how claims and authorizations move through the financial process. This revenue cycle management guide gives useful context for how healthcare organizations track documentation, coverage, and payment workflows.
Your Ground Transportation Questions Answered
Is ground transportation only for airport trips
Ground transportation means movement by land. In everyday travel, that can mean buses, trains, taxis, or airport shuttles. In medical transport, it also includes wheelchair vans, stretcher vehicles, and ambulances that move a patient between home, hospitals, rehab centers, and airports.
That broader meaning matters in healthcare. For many patients, ground transport is the first and last leg of the trip. It gets them from bedside to aircraft, then from aircraft to the receiving facility, so the full transfer can happen without gaps in care.
How far in advance should I book medical ground transport
Earlier is better.
A simple discharge ride may be arranged quickly. A higher-acuity transfer usually needs more planning time so the transport team can review the patient's condition, confirm the right vehicle and crew, and line up pickup and arrival times with the sending and receiving facilities. If air ambulance is involved, timing matters even more because the ground team has to fit into the larger transfer plan.
Can a family member ride along
Sometimes. The answer depends on safety, space, the patient's condition, and company policy.
For example, one extra rider may be reasonable in a non-emergency vehicle with room for a companion. In a tightly staffed ambulance or an airport transfer tied to a medical flight, the crew may need every seat for equipment and clinical personnel. If the patient is anxious, confused, or needs help communicating, bring that up early so the coordinator can tell you what is possible.
What if the patient gets worse during the trip
The response depends on the type of transport you booked. An ambulance with clinical staff can assess changes and provide care within its licensed scope. A wheelchair or stretcher vehicle is meant for patients who are stable and do not need medical treatment during the ride.
This is why transport planning works a lot like choosing the right hospital unit. You would not place an ICU patient on a regular medical floor. In the same way, the vehicle and crew have to match the patient's expected needs during the trip, not just the distance on the map.
What's the simplest way to choose
Start with the patient's medical needs and work outward from there.
Ask one practical question first. What could happen during this ride, and who needs to be there if it does? That question usually clarifies whether the patient needs a basic ride, a medically supervised ground transfer, or a ground leg coordinated with an air ambulance.
If you are unsure, ask the sending team and transport provider to explain the recommendation in plain language. A good coordinator should be able to walk you through it step by step and explain how each part of the trip fits into the full bedside-to-bedside plan.